3808
Rapid 3D sub-millimeter isotropic T1ρ mapping of the knee using motion-robust interleaved spin-lock acquisition with compressed sensing1Saitama Medical University, Saitama, Japan, 2Philips Japan, Tokyo, Japan
Synopsis
For T1ρ quantification, a three-dimensional (3D) acquisition is desired to obtain high-resolution images. In order to achieve a rapid and robust acquisition of 3D T1 rho mapping data, we examined here the 3D sub-millimeter isotropic resolution sequences, applying them to the assessment of knee-joint. 3D isotropic resolution sequences can reduce partial-volume artifacts through the acquisition of thin continuous sections through joints. Furthermore, the isotropic source data can be used to create multiplanar reformations (MPRs). With the optimized voxel size (0.8mm3), we could obtain motion-robust high-quality isotropic images within the time constraints of a clinical exam (<10 minutes) .
Introduction
Spin-lattice relaxation in the rotating frame (T1ρ) has been shown to be sensitive to biochemical changes such as proteoglycan content of articular cartilage1. Conventional T1ρ-weighted imaging protocols often consist of two-dimensional (2D) anisotropic resolution sequences, which can be time consuming, and have relatively thick sections and gaps between sections that can lead to partial-volume artifacts. Three-dimensional (3D) isotropic resolution sequences can reduce partial-volume artifacts through the acquisition of thin continuous sections through joints2. Furthermore, the isotropic source data can be used to create multiplanar reformations (MPRs), thereby eliminating the need to repeat sequences in multiple planes. The use of 3D isotropic resolution sequences in clinical practice could markedly decrease examination times, which would improve patient comfort, reduce motion artifacts, and increase the clinical efficiency of the MR imaging unit.A T1ρ-map can be calculated from multiple T1ρ-weighted images with different spin-lock (SL) preparation times, which until now required different scans. Combining images from different scans is challenging even though in not-so moving organs, such as knee-joint, because small position changes during quite long scans (typically 10 minutes) will lead to artifacts in the resulting T1ρ-map.
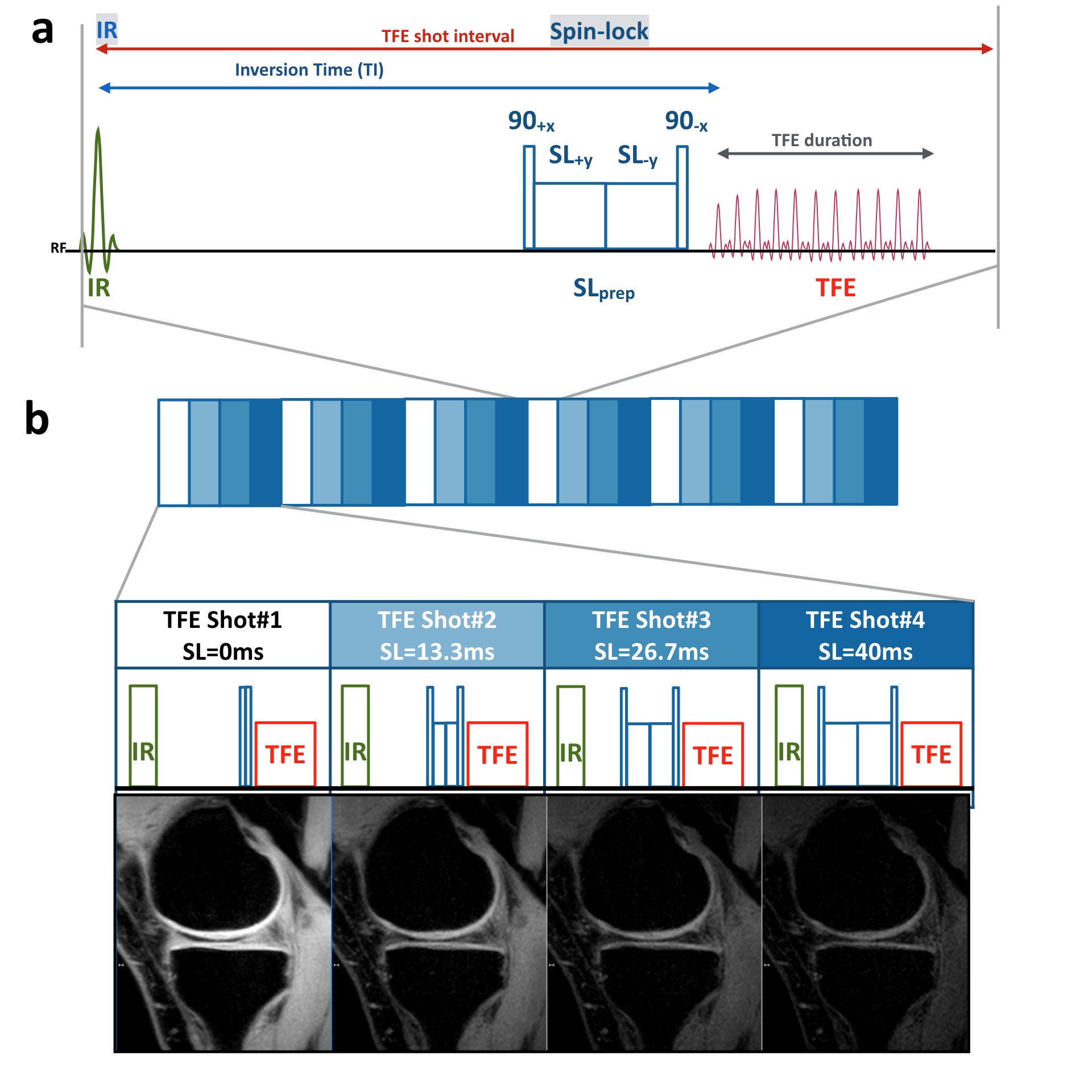
Recently, a unique interleaved spin-lock prepared steady-state free precession pulse sequence has been proposed to achieve single breath-hold T1ρ-Mapping of the heart3, which employs different SL pulses alternately before each gradient-echo train. Our strategy was to optimize and establish such interleaved SL-imaging for the knee-joint, which could be reducing inter-shot variability caused by motion or other factors related to quite long acquisition time.
On the other hand, a combination of parallel imaging and compressed sensing technique (Compressed SENSE, C-SENSE) has recently been developed to accelerate the acquisition time without increasing the image artifacts4,5. Accelerating the acquisition time can of course reduce the motion-related artifacts. We hypothesized that the combination of these new methods allows rapid and robust acquisition of 3D T1 rho mapping data. The purpose of this study was to demonstrate the feasibility of accelerated 3D sub-millimeter isotropic T1ρ-mapping of the knee-joint using motion-robust interleaved spin-lock acquisition with Compressed SENSE.
Methods
A total of 11 patients were examined on a 3.0T system (Ingenia Elition, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects.Scheme of the sequence for T1ρ-mapping we applied in this study is shown in Figure 1. T1ρ-mapping was performed using an inversion-recovery and T1ρ-prepared segmented gradient echo (turbo field-echo; TFE) sequence with water-selective excitation (ProSet). Inversion-recovery was used for suppressing synovial fluid. Four images with different SL preparation times (SL = 0, 13, 27, and 40ms) were acquired with interleaved acquisition. Amplitude of the SL pulse was set to 500 Hz.
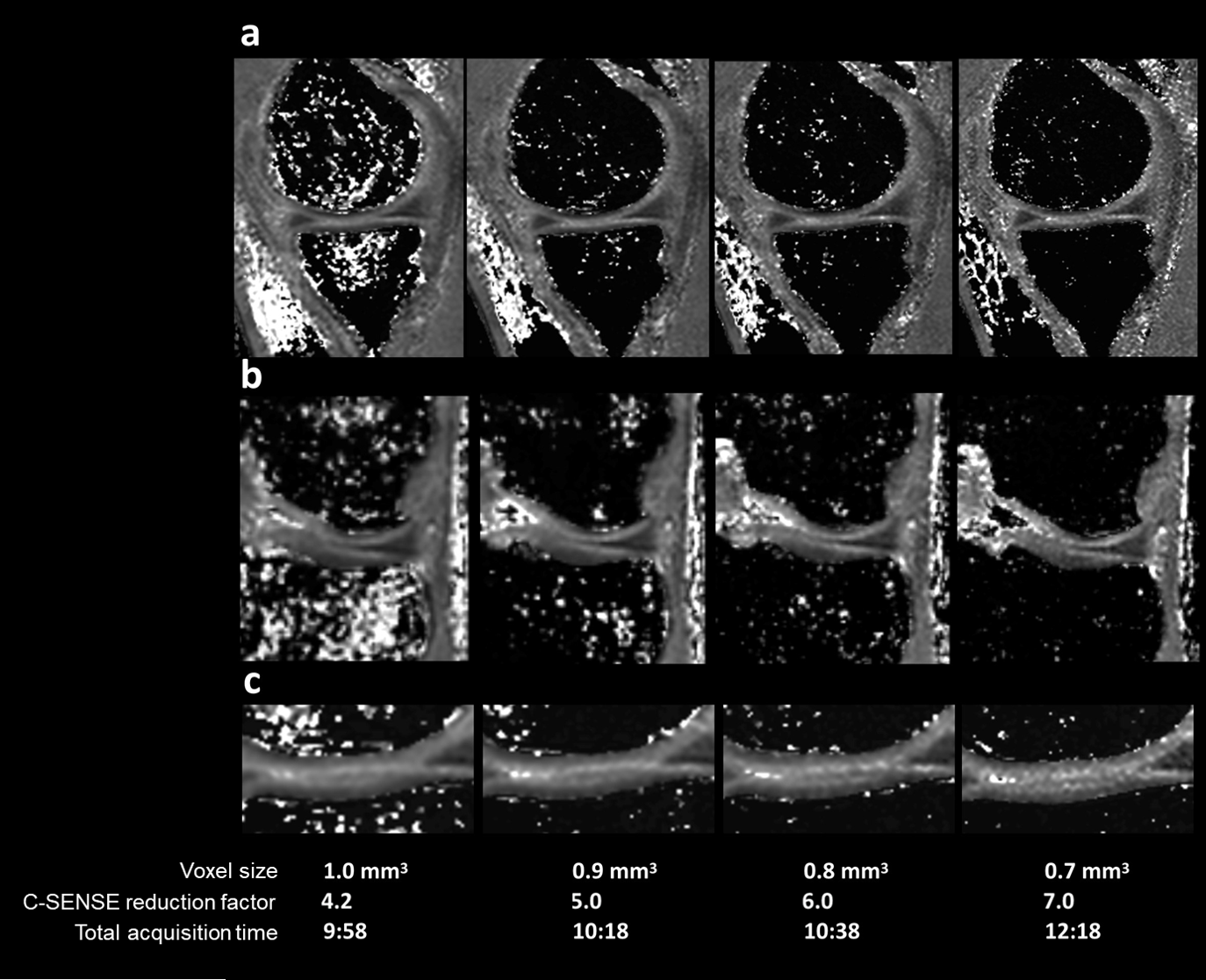
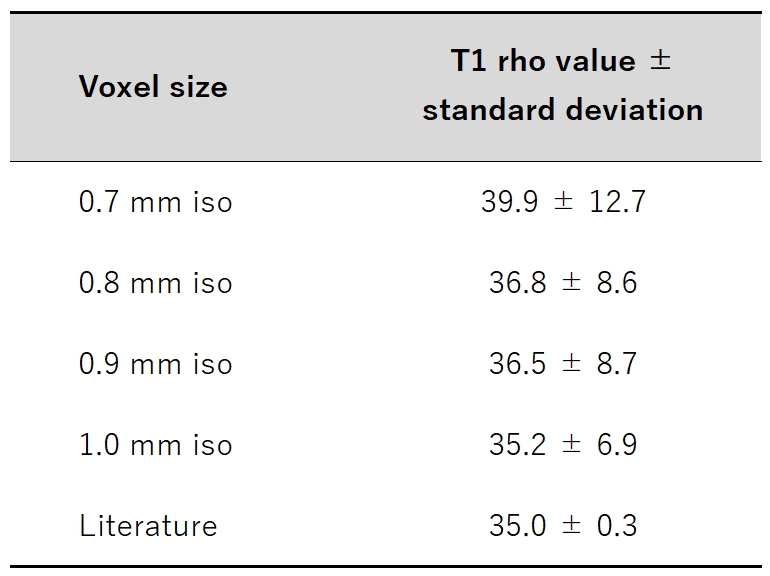
To optimize the scan protocol of 3D isotropic T1p mapping in the knee-joint, we compared the actual acquired voxel size (1.0, 0.9, 0.8, and 0.7 mm3), while maintaining the total acquisition time (10 minutes) by changing the C-SENSE reduction factors. To validate the obtained T1ρ values, sagittal T1ρ maps were quantitatively compared. The average T1ρ values and their standard deviations (SDs) in the region-of-interests (ROIs) of the knee cartilage were used for comparison among respective spatial resolutions. We also compared with the T1ρ values reported in literature6.
Imaging parameters for 3D isotropic T1p mapping were: sagittal, TR=8.5ms, TE=3.5ms, TFE factor=128, voxel size=1.0 to 0.7mm3 (1.0, 0.9, 0.8, and 0.7mm3), 100 to 143 slices, TFE shot interval=5000ms, inversion delay=1760ms, ProSet1331, C-SENSE reduction factor=4.2 to 7, and total acquisition time=9:58 to 12:18.
Results and Discussion
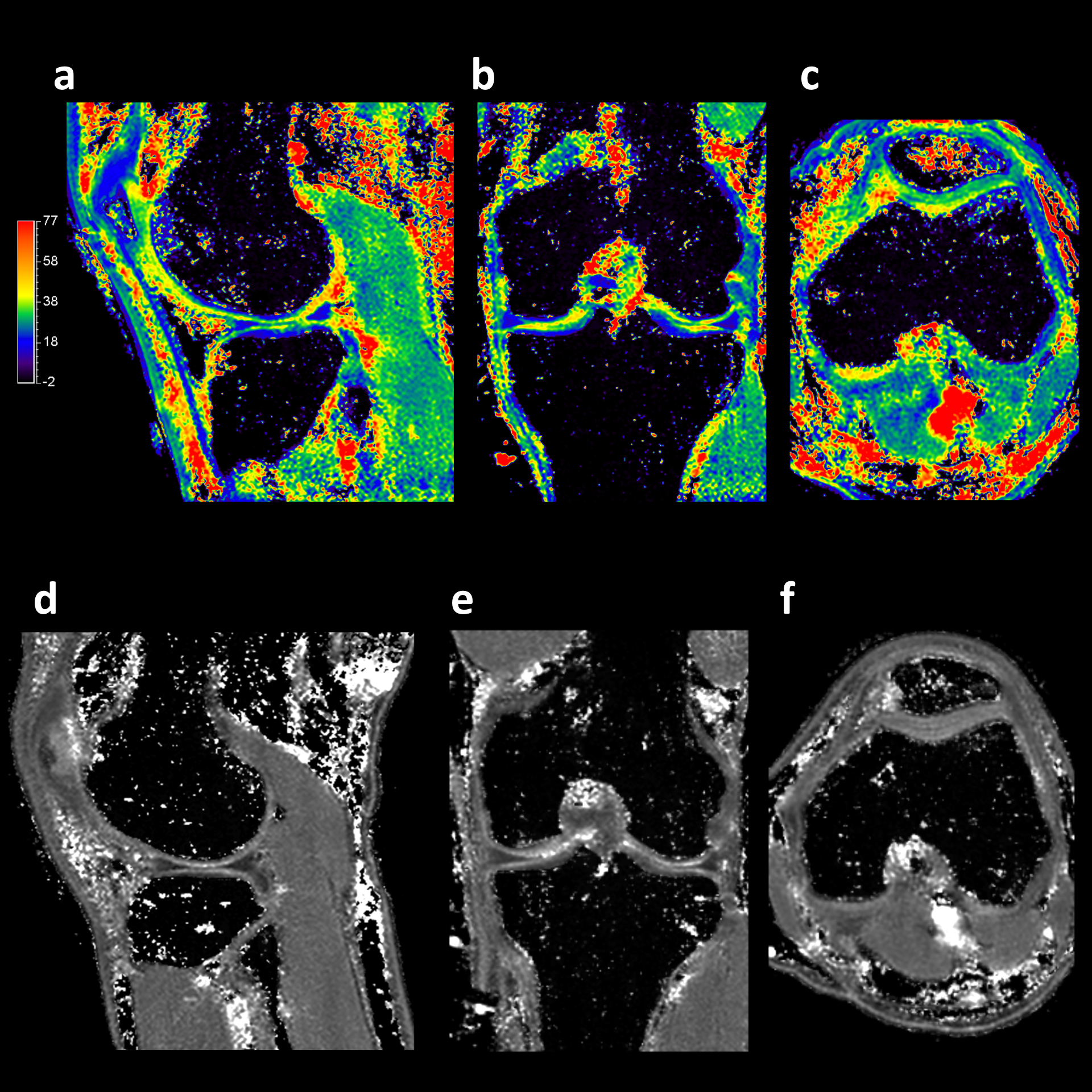
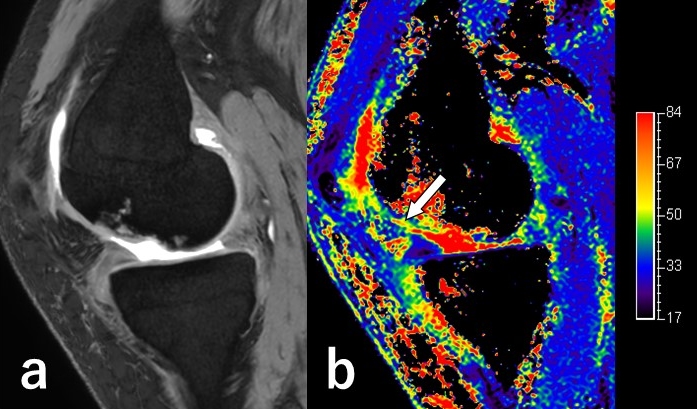
Comparison of T1ρ value with standard deviation (SD) among different acquired voxel sizes (1.0, 0.9, 0.8 and 0.7 mm3) measured at the central lateral portion of the femur was shown in Table 1. T1ρ values of all sequences were close to the values reported in literature6. Representative images of 3D isotropic T1ρ-mapping with were shown in Figure 2. Acquired voxel size of 0.7mm3 showed excellent MPR quality. However, as shown in Table 1, SD of T1ρ values with 0.7 mm3 acquisition was significantly higher than that of others due to presence of streak artifact probably caused by reduced SNR. Thus, we chose 0.8mm3 sequence for optimal 3D isotropic T1ρ-mapping. Representative MPR images of 3D isotropic T1ρ-mapping with 0.8mm3 acquisition were shown in Figure 3. The optimized sequence provided motion-insensitive high-quality isotropic images in 10 minutes. Figure 4 demonstrates one case with cartilage damage at the femoral condyle. Elevated T1ρ value is depicted on 3D isotropic T1ρ-mapping.Conclusion
The study demonstrated the feasibility of rapid 3D sub-millimeter (0.8mm3) isotropic T1ρ-mapping of the whole knee-joint in 10 minutes using motion-robust interleaved spin-lock acquisition with Compressed SENSE. This technique might be useful for decreasing examination times and motion artifacts, thereby improve the quality and efficiency of 3D T1ρ-mapping imaging.Acknowledgements
References
1. Wáng, Y. X., et al. T1ρ magnetic resonance: basic physics principles and applications in knee and intervertebral disc imaging. Quantitative imaging in medicine and surgery, 2015 Dec; 5(6): 858–885.
2. Pakin SK, et al. 3D-T1ρ quantitation of patellar cartilage at 3.0T. J Magn Reson Imaging. 2006 Dec; 24(6): 1357-63.
3. van Oorschot JW, et al. Single Breath-Hold T1ρ-Mapping of the Heart for Endogenous Assessment of Myocardial Fibrosis. Invest Radiol. 2016 Aug; 51(8): 505-12.
4. Geerts-Ossevoort L, et al. Compressed SENSE Speed done right. Every time. The Netherlands: Philips Healthcare; 2018 Jan. Report No: 4522 991 31821. https://www.philips.de/content/dam/b2bhc/de/resourcecatalog/landingpages/ingeniaelition/White_Paper_Compressed_SENSE-opt.pdf
5. Mönch S, et al. Magnetic Resonance Imaging of the Brain Using Compressed Sensing - Quality Assessment in Daily Clinical Routine. Clin Neuroradiol. 2019 May 16. doi: 10.1007/s00062-019-00789-x. [Epub ahead of print]
6. Baboli R et al. Isotropic morphometry and multicomponent T1ρ mapping of human knee articular cartilage in vivo at 3T. J Magn Reson Imaging. 2018 Dec; 48(6): 1707-1716.
Figures