3719
Fast Distortion-Free DWI using PSF-EPI on A 1.5T Clinical MRI Scanner with An 8-Channel Head Coil1Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China, 2Shenzhen Anke High-tech Co., Ltd., Shenzhen, China, 3Philips Healthcare, Beijing, China
Synopsis
DWI is valuable for diagnosing diseases such as stroke and brain tumor. The traditional single-shot EPI is widely used in DWI because of its high acquisition speed, but it suffers from severe geometric distortions. A recently proposed technique, point-spread-function encoded EPI (PSF-EPI) that is highly accelerated by tilted-CAIPI, can achieve fast distortion-free DWI images on 3T scanners with a 32-channel head coil. This study investigated the feasibility of tilted-CAIPI accelerated PSF-EPI on a 1.5T clinical MRI scanner with an 8-channel head coil. Images with high anatomical fidelity and satisfactory SNR were obtained in 1~2.5 min using this technique.
Introduction
DWI has been proved valuable in diseases such as stroke, brain tumor, and cerebral infarction 1-4. Single-shot echo planar imaging (SS-EPI) is the mostly adopted technique for DWI due to its high acquisition efficiency and insensitivity to bulk motion. However, SS-EPI suffers from T2* blurring and severe geometric distortions. A recently proposed technique, tilted-CAIPI accelerated point-spread-function encoded EPI (PSF-EPI), enables fast, distortion- and blurring-free DWI on 3T MRI scanners with a 32-channel head coil 5-8. Although there is a growing interest in the use and increasing availability of 3T MRI scanners, 1.5T MRI scanners are still widely used in clinical practice, due to the less cost of equipment purchase, installation, maintenance and operation 9, less magnetic field heterogeneity, less biological effects 10, etc. On 1.5T scanners, array coils with a large number of elements (e.g., 32), are often not available. In this study, we tested the feasibility of fast distortion-free DWI on a clinical 1.5T MRI scanner with an 8-channel head coil, using PSF-EPI that was highly-accelerated by tilted-CAIPI.Methods
This study was approved by the local Institutional Review Board and written informed consents were obtained from the healthy volunteers. Whole-brain data were acquired on an Anke 1.5T SuperMark scanner (Shenzhen Anke High-tech Co., ltd., China), using an 8-channel head coil. The maximum gradient strength and slew rate are 25 mT/m and 60 T/m/s, respectively.In the PSF-EPI sequence, an additional step-wise phase encoding gradient was applied before the EPI readout of the 2D SS-EPI sequence, in a multi-shot manner 8. This generates a 3D k-space, which consists of kx (readout), ky (phase encoding, PE) and ks (PSF-encoding) dimensions. Distortion-free images were obtained along kx-ks.
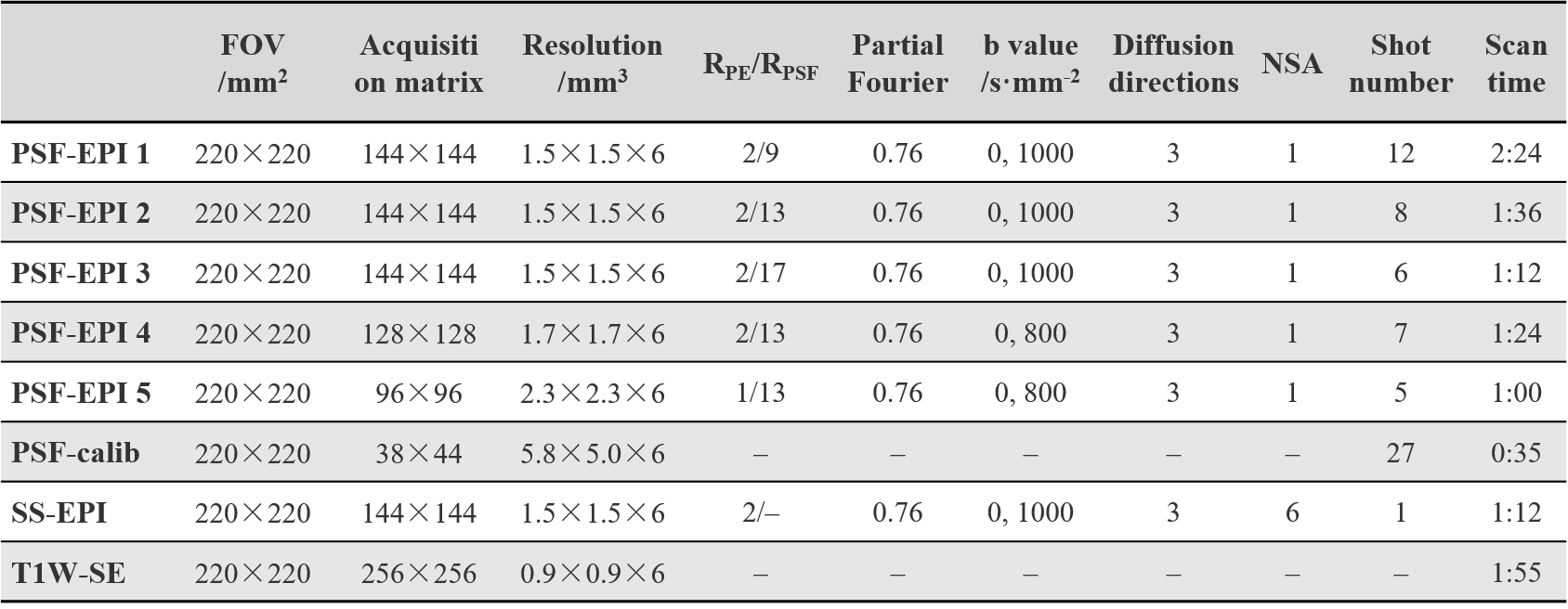
The specific parameters of the PSF-EPI sequence, as well as the SS-EPI and distortion-free T1W-SE sequences, are listed in Table 1. The acceleration rates along PE- and PSF-encoding are denoted by RPE and RPSF, respectively. The 8-channel head coil used here allows a maximum RPE of 2. To achieve the tilted-CAIPI kernel in the ky-ks plane, RPSF was set to odd numbers when RPE = 2. At the end of each EPI readout, 6 extra ky lines were acquired for self-navigated inter-shot phase correction of diffusion data. No ramp sampling was adopted during the EPI readout. The undersampled data were reconstructed by PE-GRAPPA and PSF-GRAPPA with a calibration scan 5.
To test the compatibility of the highly-accelerated PSF-EPI with array coils having fewer elements, four channels were manually selected from the 8-channel coil array, for the sequence PSF-EPI 5 (Table 1). The criteria of channel selection is to ensure that the intensity of images is as uniform across brain as possible after channel combination.
Results and Discussion
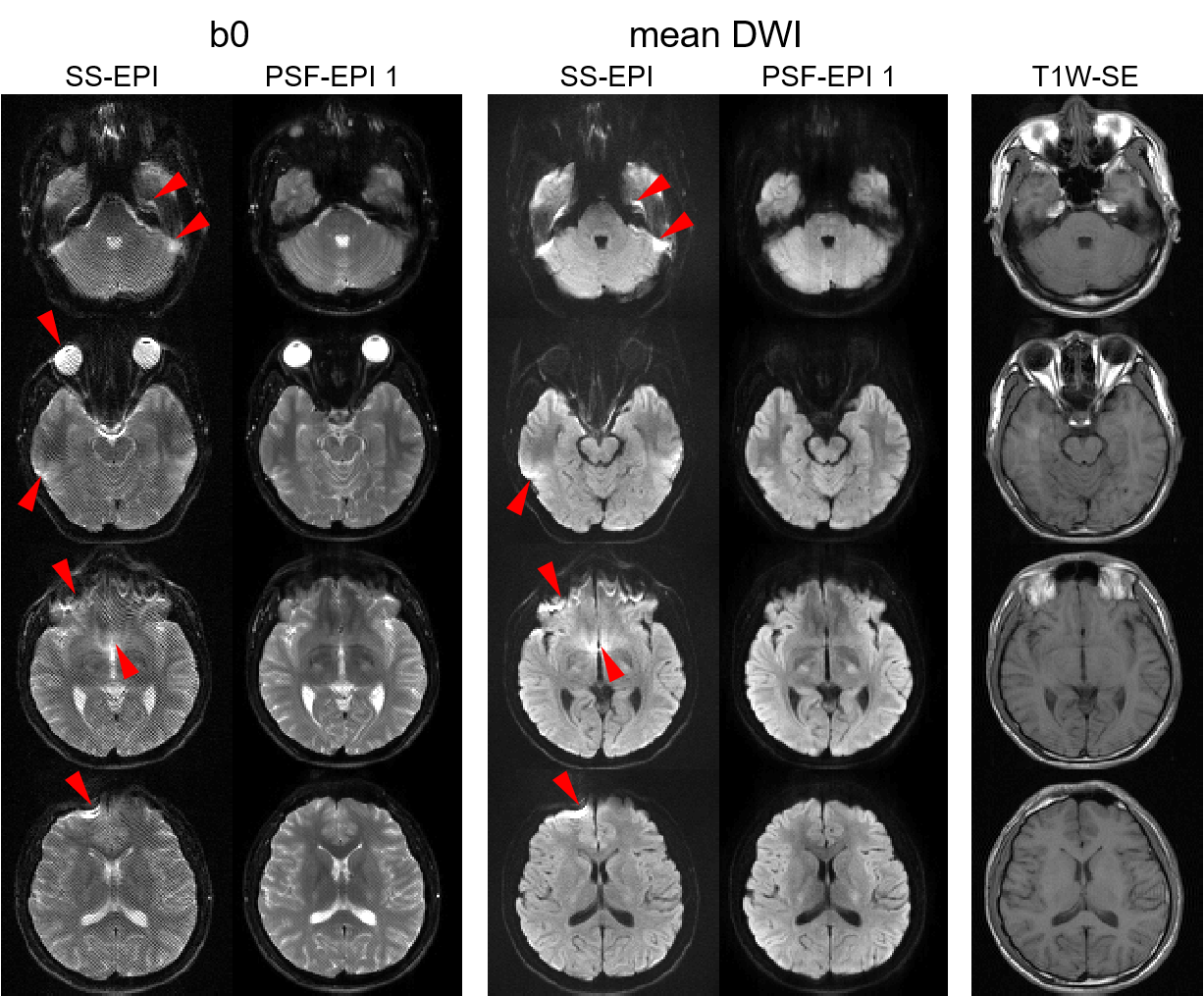
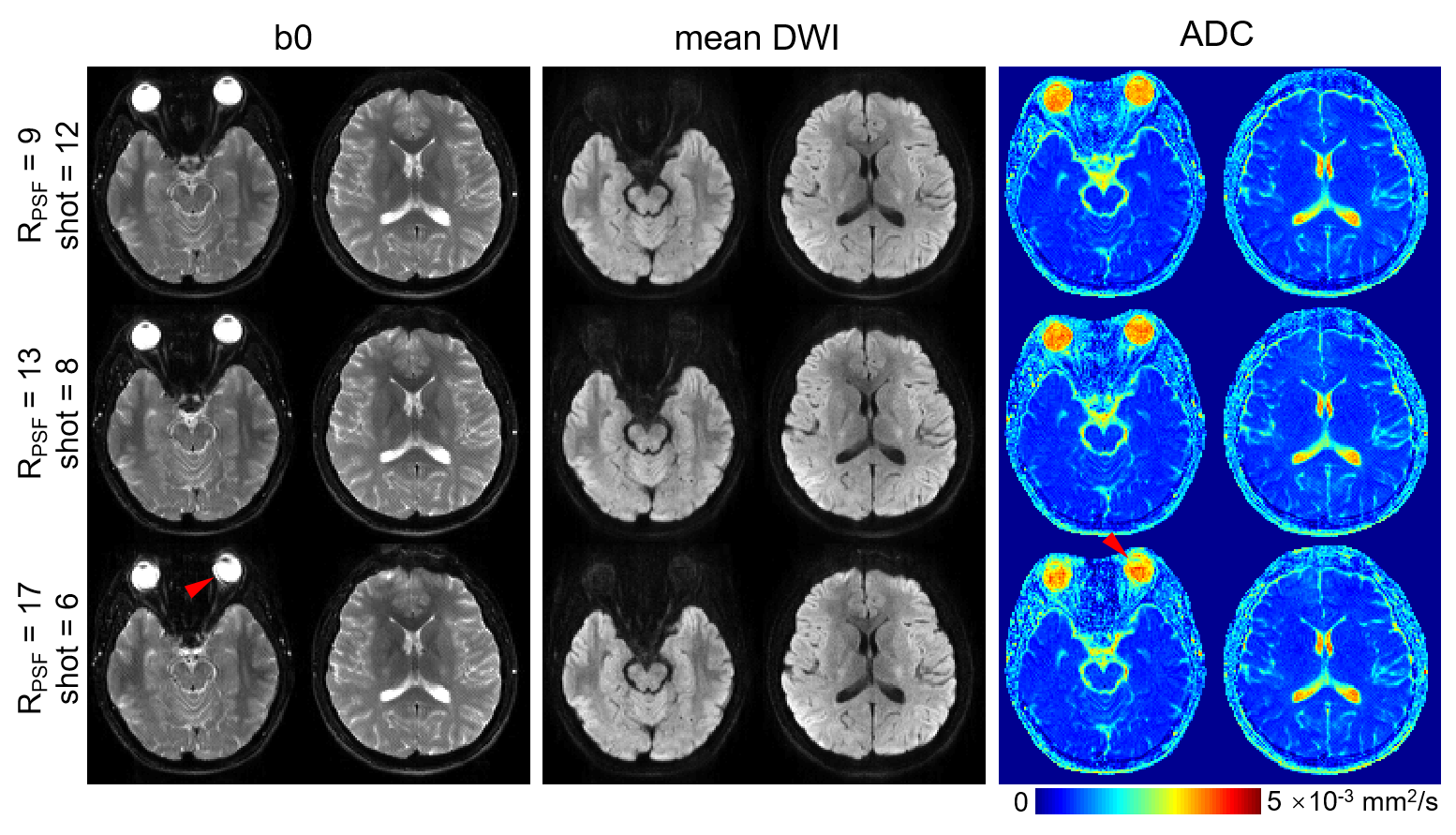
Figure 1 shows the comparison between the 12-shot PSF-EPI (RPSF = 9) and SS-EPI with NSA = 6. SS-EPI suffers from severe distortions (arrows). On the contrary, PSF-EPI maintains high consistency with the distortion-free T1W-SE reference. In addition, the PSF-EPI mean DWI images show satisfactory SNR performance. Note that there are obvious ripple-like artifacts in the SS-EPI b0 images. These artifacts are possibly due to gradient waveform infidelity, which can distort the k-space trajectory 11. These artifacts are greatly reduced in the PSF-EPI b0 images, which might be due to less sensitivity of kx-ks to gradient infidelity than kx-ky.Figure 2 shows the feasibility of PSF-EPI with higher RPSF. The two slices shown here are the same as the 2nd and 4th rows in Figure 1. With RPSF = 13 (shot = 8) or 17 (shot = 6), distortion-free images can still be obtained, while the total number of shots can be reduced compared to RPSF = 9, thus saving the acquisition time. Meanwhile, with RPSF = 13 or 17, the SNRs of mean DWI images are only slightly degraded, and the ADC maps maintain high consistency with RPSF = 9. The 6-shot (RPSF =17) PSF-EPI achieves higher geometric fidelity and comparable SNR, while using the same acquisition time, when compared to the SS-EPI protocol that has a default NSA of 6. Concerning the eyeballs, RPSF = 13 is a safer acceleration factor than RPSF =17 (arrows).
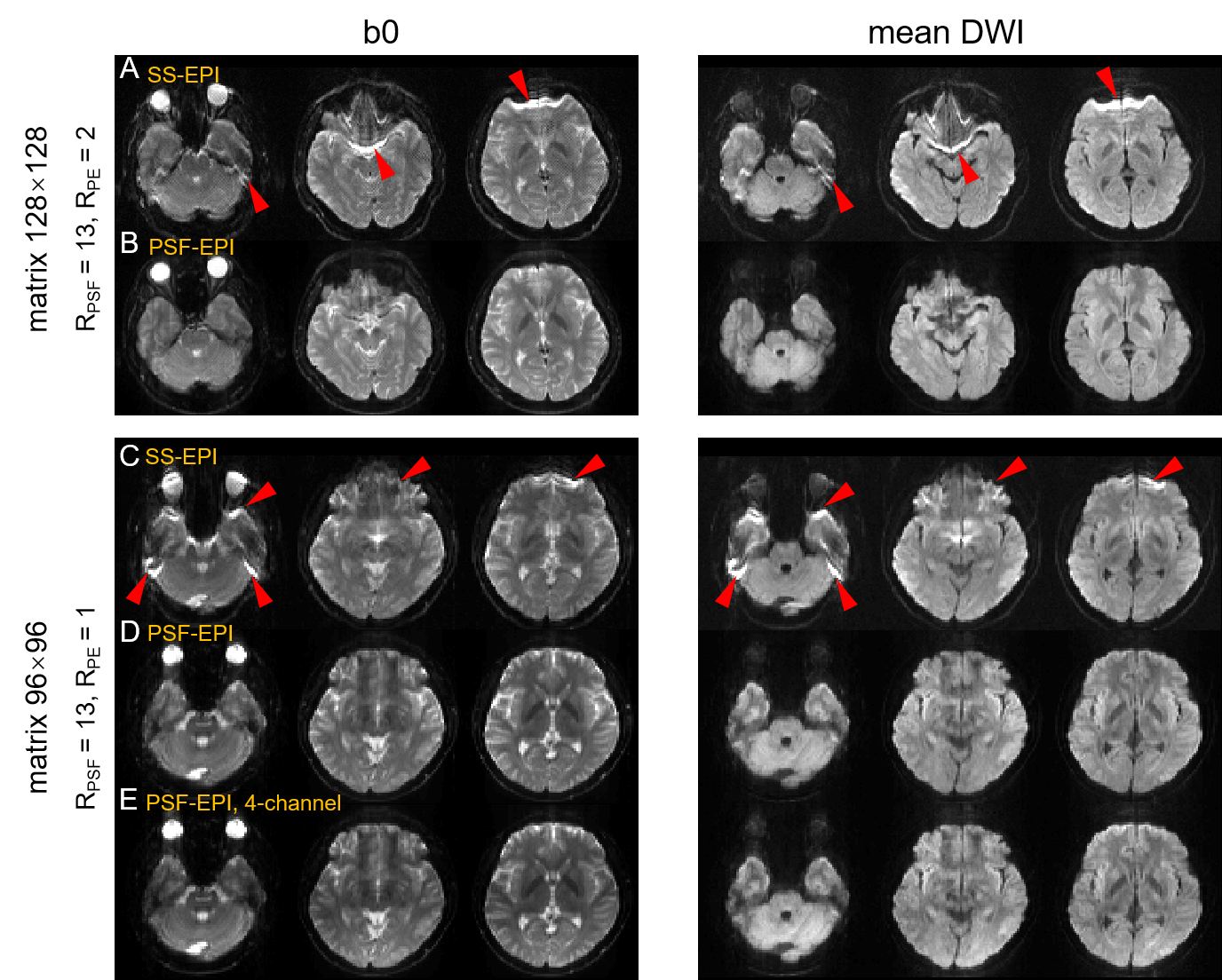
Figure 3 shows the results of PSF-EPI with lower resolution, which requires less shots thus faster acquisition, and less number of coil elements, when RPSF = 13. The severe distortions in SS-EPI (Figure 3A, C) disappear in PSF-EPI (Figure 3B, D, E). When using the undersampled PSF-EPI data from 4 of the 8 coil elements, the distortion-free images can still be reconstructed (Figure 3E). This indicates that PSF-EPI can still be highly accelerated even using array coils with 4 channels.
Conclusion
This study demonstrates the feasibility of fast distortion-free DWI for the brain on a 1.5T clinical MRI scanner with an 8-channel head coil, using tilted-CAIPI accelerated PSF-EPI. With clinically practical acquisition time, i.e., 1~2.5 min, PSF-EPI achieves images with high anatomical fidelity and satisfactory SNR. Highly accelerated PSF-EPI is also potentially compatible with array coils with few elements, e.g., 4.Acknowledgements
No acknowledgement found.References
1. Lovblad KO, Laubach HJ, Baird AE, et al. Clinical experience with diffusion-weighted MR in patients with acute stroke. AJNR Am J Neuroradiol 1998;19(6):1061-1066.
2. Fiebach J, Jansen O, Schellinger P, et al. Comparison of CT with diffusion-weighted MRI in patients with hyperacute stroke. Neuroradiology 2001;43(8):628-632.
3. Kono K, Inoue Y, Nakayama K, et al. The role of diffusion-weighted imaging in patients with brain tumors. AJNR Am J Neuroradiol 2001;22(6):1081-1088.
4. Toyoda K, Kitai S, Ida M, Suga S, Aoyagi Y, Fukuda K. Usefulness of high-b-value diffusion-weighted imaging in acute cerebral infarction. Eur Radiol 2007;17(5):1212-1220.
5. Dong Z, Wang F, Reese TG, et al. Tilted-CAIPI for highly accelerated distortion-free EPI with point spread function (PSF) encoding. Magn Reson Med 2019;81(1):377-392.
6. Hu Z, Wang Y, Dong Z, Guo H. Water/fat separation for distortion-free EPI with point spread function encoding. Magn Reson Med 2019;82(1):251-262.
7. Li G, Wang Y, Shang Y, Qiao Y, Guo H. Cholesteatomas Detection using PSF-encoded EPI DWI. In Proceedings of the 27th Annual Meeting of ISMRM. Montreal, Canada, 2019. p. 0350.
8. Zhang J, Wang Y, Xiong Y, Guo H. Distortion-free diffusion-weighted imaging of the eyeballs and the optic nerves using PSF-EPI. In Proceedings of the 27th Annual Meeting of ISMRM. Montreal, Canada, 2019. p. 0345.
9. Wardlaw JM, Brindle W, Casado AM, et al. A systematic review of the utility of 1.5 versus 3 Tesla magnetic resonance brain imaging in clinical practice and research. Eur Radiol 2012;22(11):2295-2303.
10. Weintraub MI, Khoury A, Cole SP. Biologic effects of 3 Tesla (T) MR imaging comparing traditional 1.5 T and 0.6 T in 1023 consecutive outpatients. J Neuroimaging 2007;17(3):241-245.
11. Bernstein MA, King KF, XJ Z. Handbook of MRI pulse sequences. New York: Elsevier Academic Press; 2004.
Figures