3682
Self-Navigated MEDIC: an improved and reliable technique for cervical spine MRI1Siemens Shenzhen Magnetic Resonance, Ltd, Shen Zhen, China, 2MR Collaborations, Siemens Healthcare Ltd., Shenzhen, China, 3SW, Siemens Shenzhen Magnetic Resonance, Ltd, Shen Zhen, China
Synopsis
In this work, we developed a navigated Multi-Echo Data Imaging Combination (MEDIC) sequence for robust cervical spine (c-spine) imaging. In this sequence, a navigator echo is acquired in each repetition period to monitor the phase instability caused by respiration-induced field variations, and such instability among multiple echoes is subsequently compensated with a linear-phase evolution model. In vivo experimental results showed that the developed navigated MEDIC sequence outperformed the conventional MEDIC sequence and might be a potential technique for the diagnosis of cervical spine on 3T
Introduction
Currently, theT2*-weighted Multi-Echo Data Imaging Combination (MEDIC) sequence is the most commonly used sequence for cervical spine imaging because of the monopolar readout gradients and the multiple-echo combination used, which are beneficial to avoid off resonance effects and generate a high signal-to-noise ratio [1]. However, during scanning, respiration-induced field variations may produce phase errors among the echoes, which decrease the signal-to-noise ratio and potentially induce severe image artifacts. To address these issues, we developed a navigated MEDIC sequence to monitor the phase instability caused by the field variation, and a segmented linear phase correction model was used to reduce the phase errors.Method
Sequence: In the developed prototype navigated MEDIC sequence, image echoes are followed by an additional navigator echo in each repetition period [Fig1]. By comparing the phase variation between the navigator echo and its predecessor navigator reference echo, the phase variation between the two navigators was calculated, then echoes acquired between these two moments were respectively calibrated with a compensation phase calculated with a segmented linear phase correction model [Fig2]. The idea of using predecessor navigator echo as correction reference is to ensure the accuracy of phase correction and reduce possible phase wrapping effect.Experiments: The IRB-approved c-spine imaging was performed in healthy volunteers on a 3T scanner (MAGNETOM Spectra, Siemens Healthcare, Shenzhen, China) with a 16-channel head/neck coil. The optimized parameters for the developed navigated MEDIC sequence included: FOV = 180 x 180 mm2, flip angle = 30o; slice number = 30; distance factor = 10%; slice thickness = 3 mm; TE/TR = 15/545 ms; BW/pixel = 260 Hz; combined echoes = 4; and scan time = 4:58 minutes. A conventional MEDIC sequence was also conducted for comparison, with similar parameters: FOV = 180 x 180mm2, flip angle = 30o; slice number = 30; distance factor = 10%; slice thickness = 3 mm; TE/TR = 15/550 ms; BW/pixel = 260 Hz; combined echoes = 4; and scan time = 4:38 minutes.
Result
Compared to the conventional MEDIC sequence, the developed navigated MEDIC sequence can effectively improve the image quality. In contrast to conventional MEDIC, the images obtained by the newly developed sequence showed less artifact and clearer tissue interfaces [Fig3]. Furthermore, the images obtained from the developed sequence looked much sharper [Fig4]. Respiratory motion during MR scans results in strong blurring and ghosting, and these negative effects may not only be directly caused by motion, but also by motion-induced field variations, and the latter are particularly more common at 3T or higher magnetic field. The segmented linear phase correction model used in this work can compensate for the phase variations.Conclusion
We developed and evaluated a new navigated MEDIC sequence for cervical spine imaging. The preliminary study has demonstrated that the technique may outperform the conventional MEDIC sequence, and might be a potential technique for the diagnosis of the cervical spine. Clinical studies are currently underway to validate the clinical value of the technique.Acknowledgements
No acknowledgement found.References
[1]Bhawan K Paunipagar et,al. Imaging of articular cartilage. Indian J Radiol Imaging. 2014 Jul-Sep; 24(3): 237–248.Figures
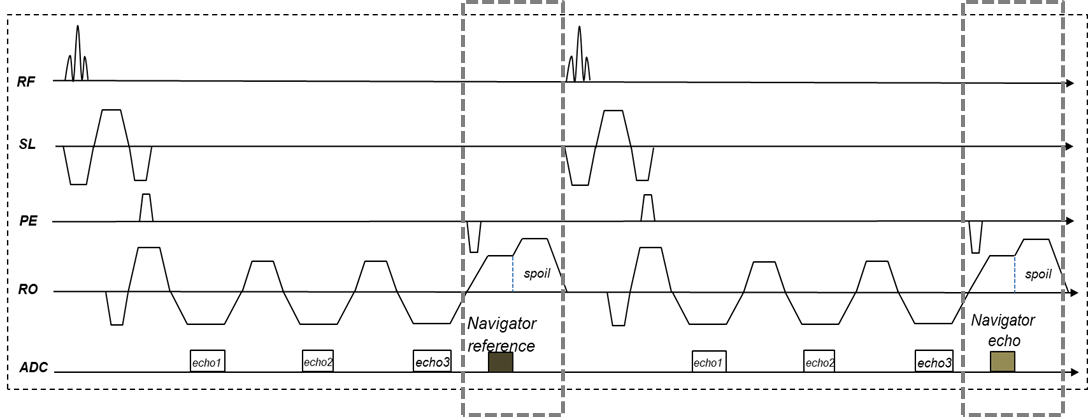
Fig 1. Diagram of the proposed MEDIC sequence with navigator
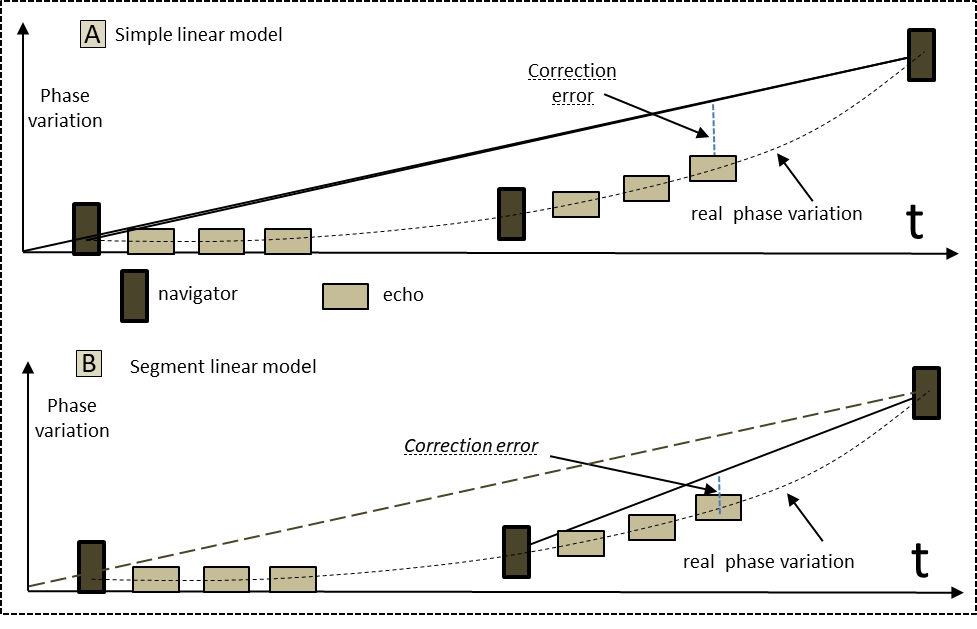
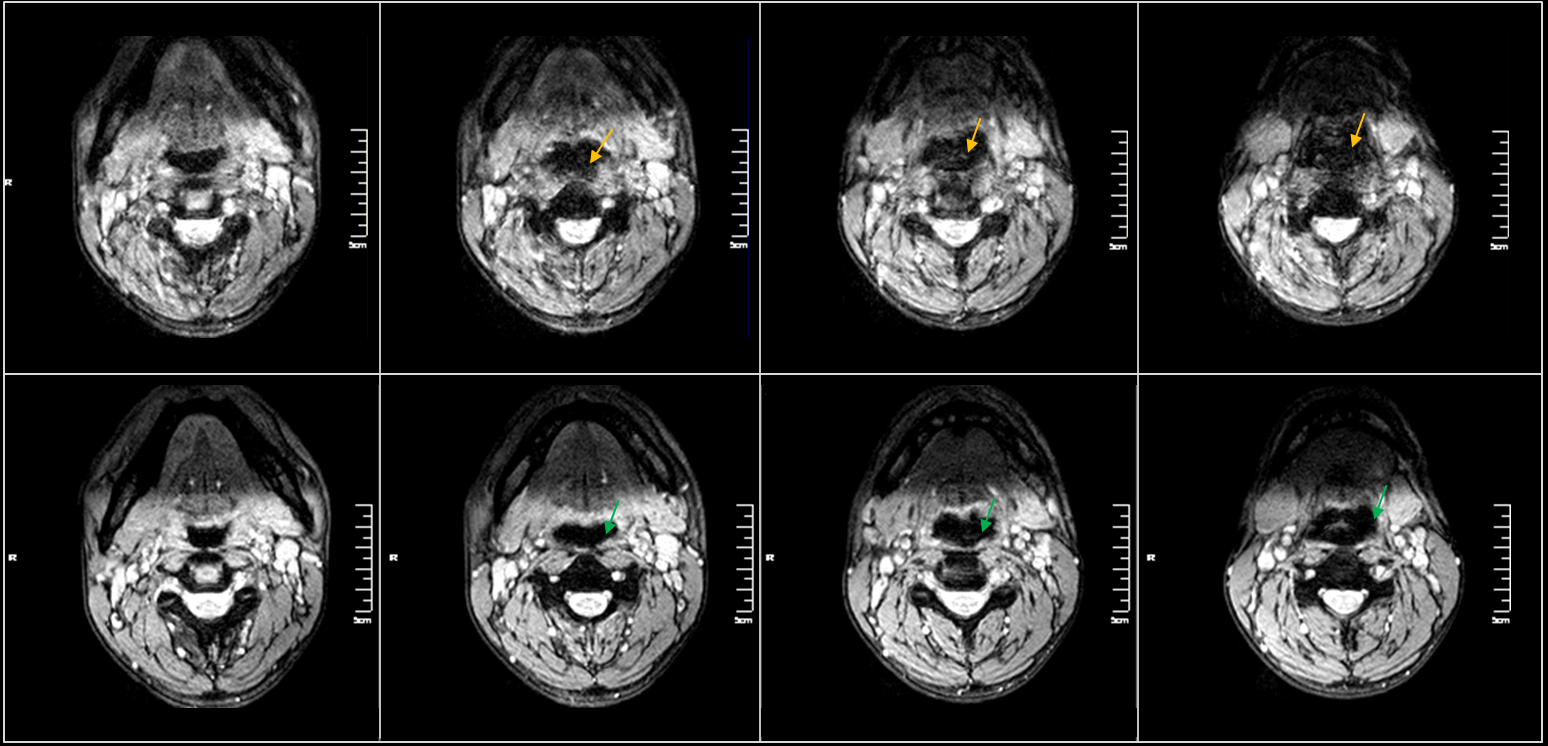
Fig3 Representative Images obtained with the developed Navigated MEDIC sequence (second row) and against those with conventional MEDIC sequence (first row). The image sharpness was obviously improved on navigated MEDIC case(green arrow). It is noticed that TR was increased to 550ms in Navigated MEDIC, so that the scan time was increased by 20 s.
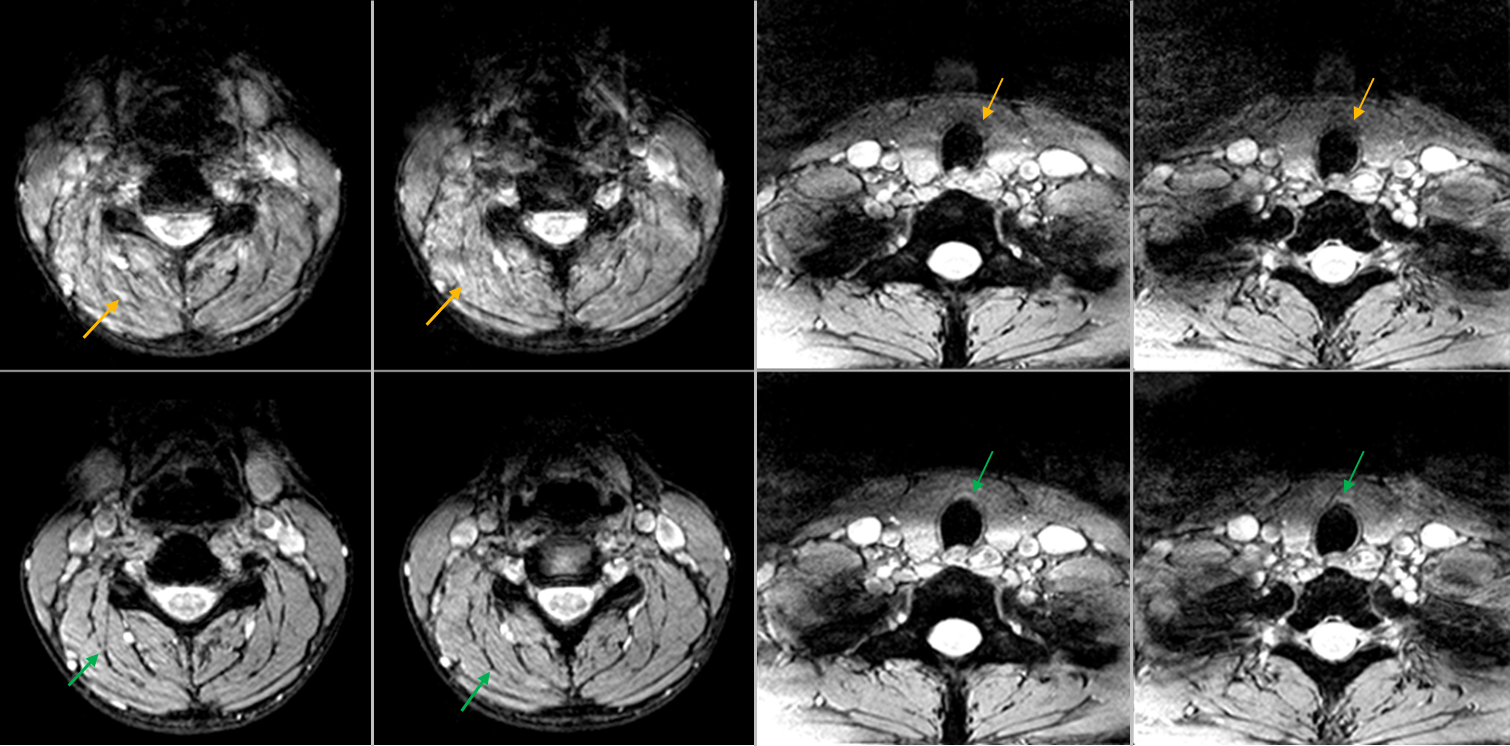
Fig4 Representative Images obtained on other volunteers(b and c) experiments also show very good consistency. Images acquired with Navigated MEDIC(first row) show more details and edge structure are more clear, while images acquired by conventional MEDIC is blurred(second row).