3680
Real Time MRI at 70 frames per second: Establishing protocols for maxillofacial surgery applications.
Aneurin J Kennerley1, Isaac J Watson2, Lloyd A.E Bollans1, David A Mitchell3, and Angelika J Sebald1,3
1Chemistry, University of York, York, United Kingdom, 2Electronic Engineering, University of York, York, United Kingdom, 3York Cross Disciplinary Centre for Systems Analysis, University of York, York, United Kingdom
1Chemistry, University of York, York, United Kingdom, 2Electronic Engineering, University of York, York, United Kingdom, 3York Cross Disciplinary Centre for Systems Analysis, University of York, York, United Kingdom
Synopsis
We showcase a 70+ frame per second Real Time MRI protocol that is robust and flexible for a number of different applications in maxillofacial surgery (including multi-plane monitoring speech and swallowing mechanisms) and associated follow up/long term monitoring for reducing depression and improving post-operative quality of life for patients. We explore the use of different food types to act as MR contrast agents to highlight changes in oral function. The project is co-created with a consulting Oral & Maxillofacial and Head & Neck Surgeon (Mr D Mitchell).
Introduction
The fast switching gradients on modern MRI scanners, alongside iterative image reconstruction1, now permit deployment of real time imaging methodologies2. Alongside important cardiac applications, real time (RT) MRI offers new opportunities for the non-invasive functional monitoring of the mechanics of speech, swallowing and breathing. Quantitative monitoring of such mechanics finds relevance before and after major ablative/reconstructive maxillofacial surgery. Many patients, in particular those with head/neck cancer or major trauma, have serious enduring post-operative problems; e.g. difficulty in swallowing and speech3. These long-term problems lead to malnutrition, isolation and depression4,5. RT MRI methods in this context can improve surgical planning, post-operative short and long term rehabilitation and monitoring. Furthermore RT-MRI can provide insight into adaption following major surgery in this region. Here we assess the safety/feasibility of RT-MRI establishing protocols for the evaluation of swallowing and speech. Data from this unique monitoring methodology will help improve the current less than optimum post-treatment support and patient management; ultimately improving the quality of life of maxillofacial patients.Methods
RT-MRI was conducted on a 3T scanner (Siemens, Magnetom Prisma) using a 64 channel head/neck Rx array coil. Image acquisition utilised an RF‐spoiled radially encoded FLASH MRI sequence (Figure 1A). Base resolution was 144 points per read direction (oversampling factor = 2) with TR = 12.5ms; TE= 1.21ms and flip angle = 5o. We employed a strongly under-sampled encoding scheme of 19 segments/interleaves. Each shot/single turn corresponded to a full image containing only 5 spokes. Data were acquired for 20 repetitions ~5.1s allowing for dynamic imaging (Figure 1B). This interleaved scheme allowed retrospective reconstruction combining successive single‐turn acquisitions to achieve real time imaging up to 70 frames per second (fps). Residual streaking artefacts were reduced by non-uniform Fourier transform (Figure 1C) and iterative image reconstruction (Figure 1D).In addition we explore the added value of imaging the swallowing mechanisms for different food-types/textures applicable for this patient group. Participants were asked to swallow a 5ml sample delivered via a pre-positioned straw during acquisition of real time data. The different homogeneous and heterogeneous T1 times of the food types tested offer potential routes to improve contrast within the oral cavity.
Results
Example real time MRI images (figure 1) following standard Cartesian re-gridding reconstruction for (A) the first repetition and (B) the final repetition where our participant is sticking their tongue out. We see longitudinal changes in CSF contrast as the water pool is RF saturated. Image artefacts can be reduced with cylindrical space non-uniform FT (C) and iterative image reconstruction (D)1 with the readout direction oversampling of the Prisma exploited at the cost of analysis time. We compare slow (4 fps) vs fast frame rate (70+ fps) reconstruction strategies. We implement a selective coil element approach to alter local contrast in the region of interest (primarily mouth). We showcase multi-plane imaging for 3D reconstruction of swallowing, vowel formation and speaking. We investigate the possibility of using real time MRI to track ventricular volume changes during functional brain imaging. The T1 benefits of different foodstuffs during this RF saturated radial FLASH sequence were tested for improved signal contrast of swallowing function. All images and resultant 'real time' videos were assessed for applicability by our project co-creator D Mitchell - a consulting Oral & Maxillofacial and Head & Neck Surgeon.Conclusion & Discussion
We showcase a RT-MRI protocol that is robust and flexible for a number of different applications in maxillofacial surgery and associated follow-up/long term monitoring for improving post-operative quality of life. We demonstrate 70 fps real time MR images of swallowing different food-types/textures, speech/vowel formation in 2D and 3D. We have identified key points needed for establishing RT MRI methodologies in maxillofacial surgery applications. Our protocols are designed such that they will augment more traditional diagnostic imaging approaches, MRI or other. Next steps include: clinical exploration and evaluation as a longitudinal study; inclusion of k-space time dependent weighting functions.Acknowledgements
Part funded by the Wellcome Trust [ref: 204829] through the Centre for Future Health (CFH) at the University of York. We thank all our willing volunteers and staff at the York Neuro-Imaging Centre for their patience with our imaging demands.References
- Block KT et.al. (2007) Magn Res Med. 57(6):1086-98
- Uecker M et al. (2010) NMR in BioMed 23(8): 986-94.
- Moore KA et.al. (2014) Int J Den Hyg 12: 36-47
- Acrher J et.al. (2008) J Oral Path Med 37: 255-70
- Bradbury E (2012) BJMOS 50: 19306
Figures
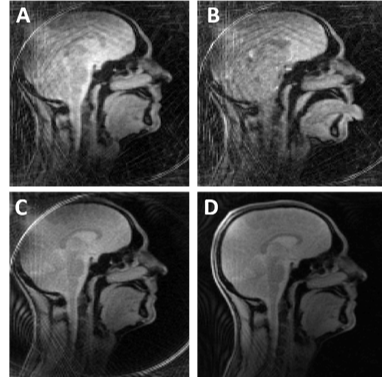
RT-MRI (A) Cartesian re-gridded reconstruction (frame 1). (B)
End frame where participant is sticking their tongue out. Image artefacts can
be reduced with non-uniform FT (C) and iterative image reconstruction
(D).
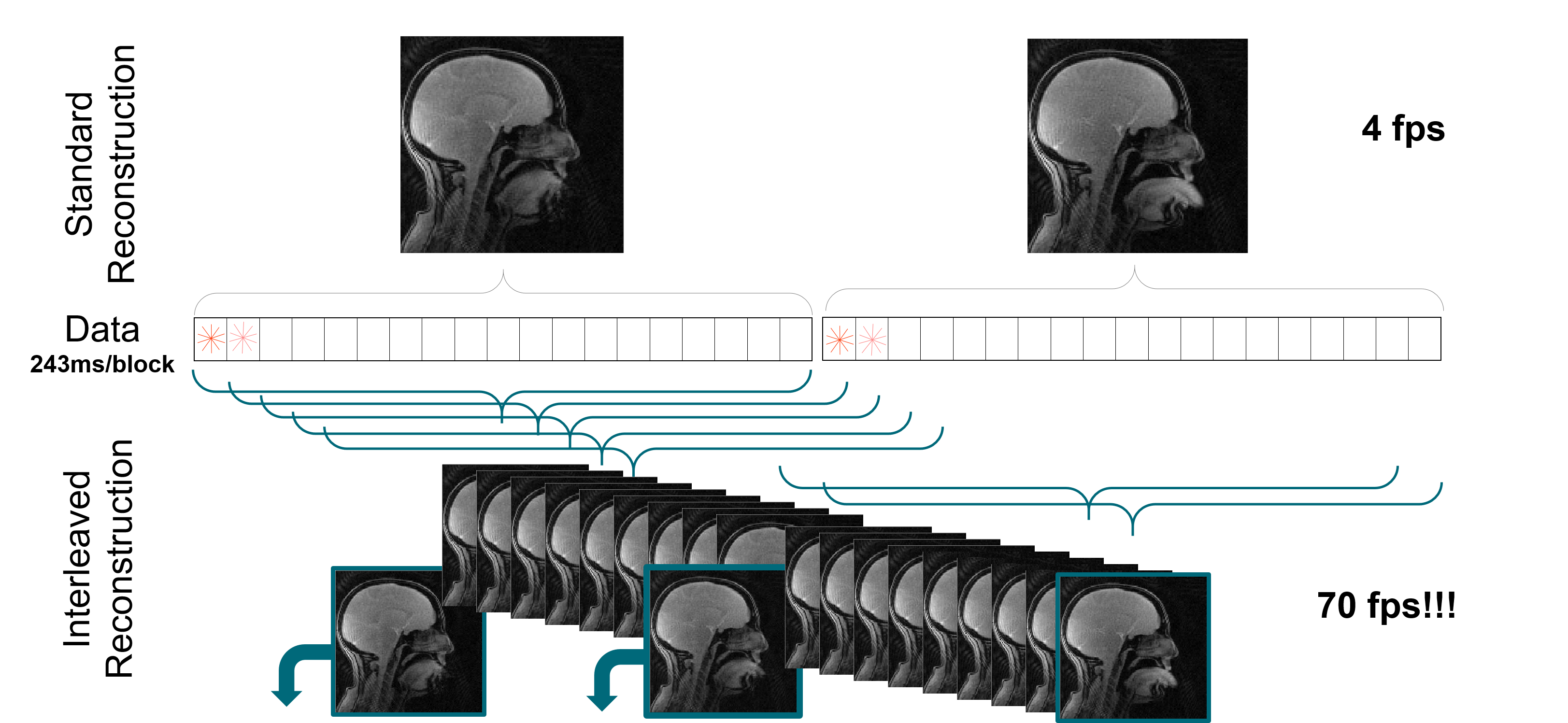
Off-line reconstruction to increase the frame rate relies on an sliding average window over sequential segments within the radial FLASH acquisition. The central weighting of k-space is compensated for. Different temporal weightings are also considered.