3640
Deep Residual Grappa (DeepGrappa): A General Purpose Self-calibrated AI based MR Reconstruction1NHLBI, NIH, Bethesda, MD, United States, 2Barts Heart Centre, Barts Health NHS Trust, London, United Kingdom
Synopsis
In this abstract, we proposed a novel self-calibration AI based MR reconstruction algorithm to utilize the power of a deep neural network. Unlike most deep learning MR reconstruction, this algorithm does not require extra training data and only works on the auto-calibration kspace lines. This algorithm is integrated to run on MR scanner via the Gadgetron InlineAI toolbox. We demonstrated this algorithm on cardiac cine imaging, showing improved image quality without introduced unrealistic anatomical structures.
Purpose
Deep learning based MR reconstruction has attracted intensive research attention during past a few years. While a set of algorithms had been proposed to apply deep neural network (NN) to different MR reconstruction problems [1], it is not ready for general clinical deployment. Deep learning based MR recon may be specific to the anatomy or to the imaging sequences. Although the trained model often gives superior image quality in targeted imaging applications, it may be difficult to transfer to new applications or imaging sequences. Even small changes in imaging protocols, such as acceleration rate or partial Fourier ratio, may require retraining to adapt the models. Another disadvantage is the requirement of many training samples. Questions are raised whether models create unrealistic image features alike anatomical structures. On the other hand, self-calibrated parallel imaging techniques, such as Grappa [2], are very successful and widely accepted for clinical imaging. With self-calibration, the auto-calibration data (ACS) is acquired with the imaging data and used for reconstruction on the per-scan basis. Noise amplification from parallel imaging is well understood due to the g-factor effects. Parallel imaging proves to be robust across imaging sequences and anatomy. Ideally, a successful deep learning algorithm should inherit these strong points from parallel imaging.One effort towards general AI based MR reconstruction is the artificial-neural-networks for k-space interpolation (RAKI) [3]. In this scheme, entire ACS data is used as a single for trainingsample. A shallow neural network with two layers (1st convolution layer: 5x4xCHA; 2nd convolution layer: 1x1xCHA) is trained to interpolate missing kspace data from acquired ones. While RAKI is a self-calibrated technique, it has two disadvantages: 1) Only a shallow NN was used to approximate the Grappa kernel calibration; 2) Since number of training set is N=1, more advanced optimization and normalization techniques, such as Adam optimization or batch normalization, cannot be used.
In this abstract, we proposed a novel self-calibration AI based MR reconstruction algorithm to utilize the power of a deep neural network. Instead of using all ACS data as a single training sample, every Grappa calibration cell is a training sample. The residual neural network design was adopted, together with batch normalization. The Adam optimization can now be used with mini-batch or full batch training data. We demonstrated this algorithm on cardiac cine imaging, showing improved image quality without introduced unrealistic anatomical structures.
Method
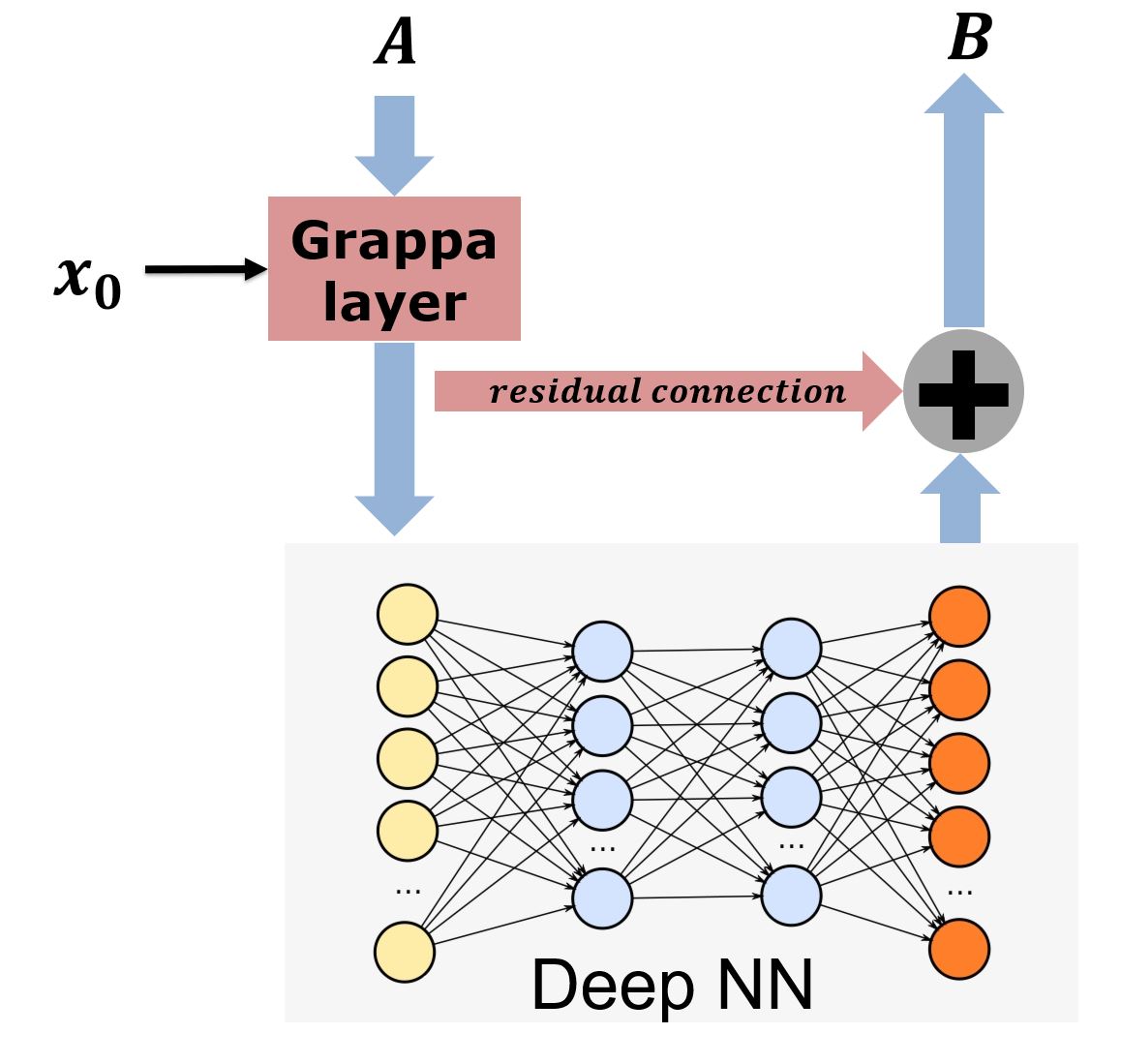
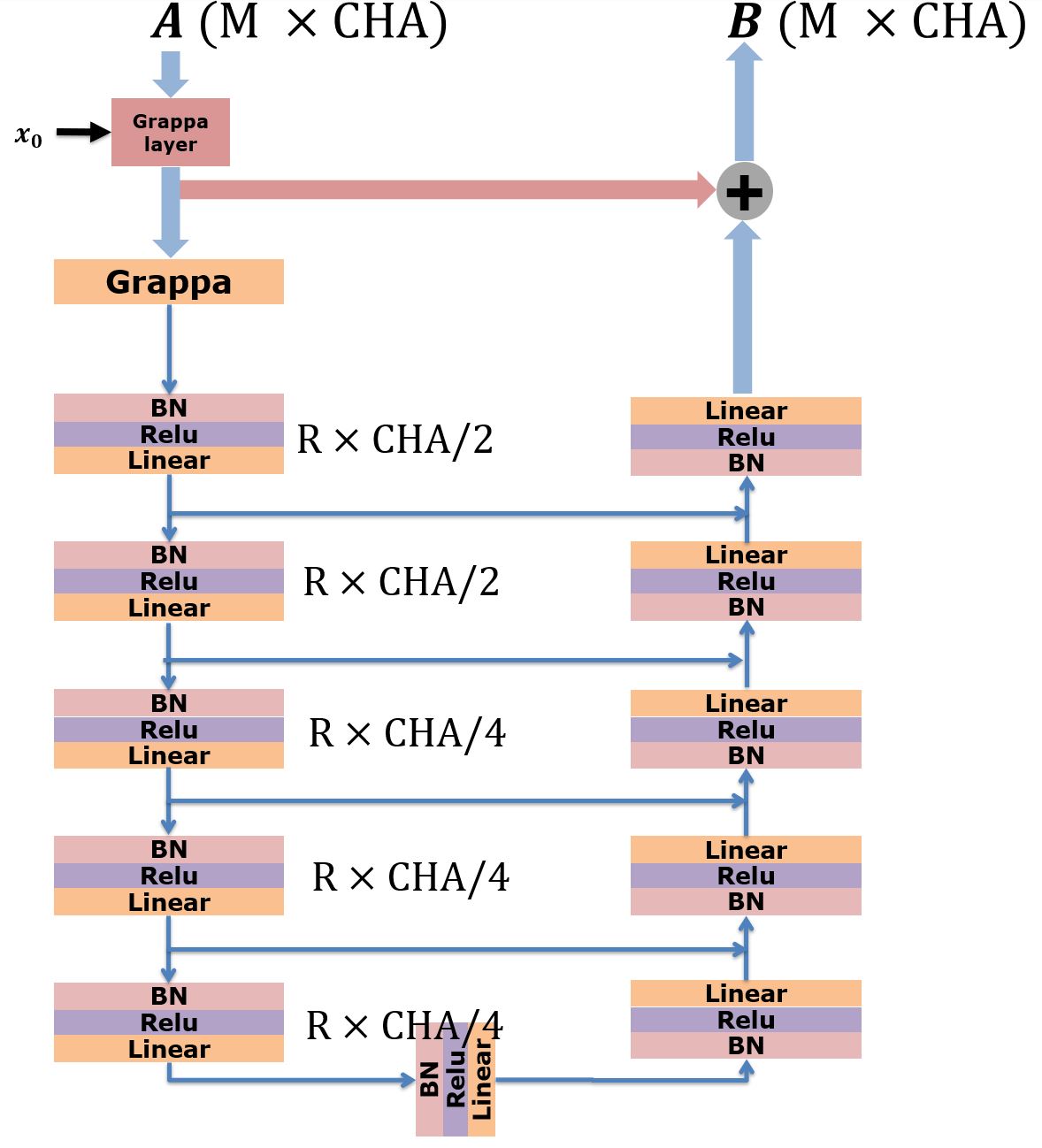
As shown in Figure 1, the DeepGrappa uses a residual NN structure. The Grappa calibration cell was first assembled from ACS data. For example, if CHA=32 channels were used, the calibration kernel along readout was 5 and along phase encoding was 4, every 5x4x32 cell was collected. All these cells are stacked together to assemble the grappa calibration equation Ax=B. In the proposed scheme, however, every calibration cell served as a training sample to NN and corresponding missing data was the output of NN. Assume the total number of calibration cell is M. The grappa calibration is remodeled as a NN layer and serves as input layer for the DeepGrappa. There was a residual connection from grappa layer to output. This would enforce the NN to “fit” on what Grappa calibration cannot learn in its linear functional space. This residual connection allowed faster convergence and gave lower residual errors. A flexible neural network architecture can be used after Grappa layer. In this experiment, a U-net architecture was used, as shown in Figure 2. The ADAM optimization was used with L2 loss between computed and acquired k-space points. Stop criteria was calibration loss is lower than or loss started increase. Here was linear grappa calibration residual.DeepGrappa was integrated on a MR scanner via the Gadgetron InlineAI toolbox [4]. The NN parameters were computed on the fly using the incoming ACS data and applied to imaging data to fill missing k-space points. Resulting images were sent back to the scanner without any user interaction.
In-vivo tests were performed on two patients for real-time cine imaging (FOV: 360x270mm2, matrix size 192x111, interleaved acceleration rate R=4, SSFP readout; for R=5, matrix size 192x105). A Siemens 1.5T scanner was used (Area, Siemens AG, Germany). Patient studies were conducted at the Barts Heart Centre, London, UK. This study was approved by the local Ethics Committee and use of the anonymized data was approved by the NIH Office of Human Subjects Research OHSR (Exemption #13156).
Results
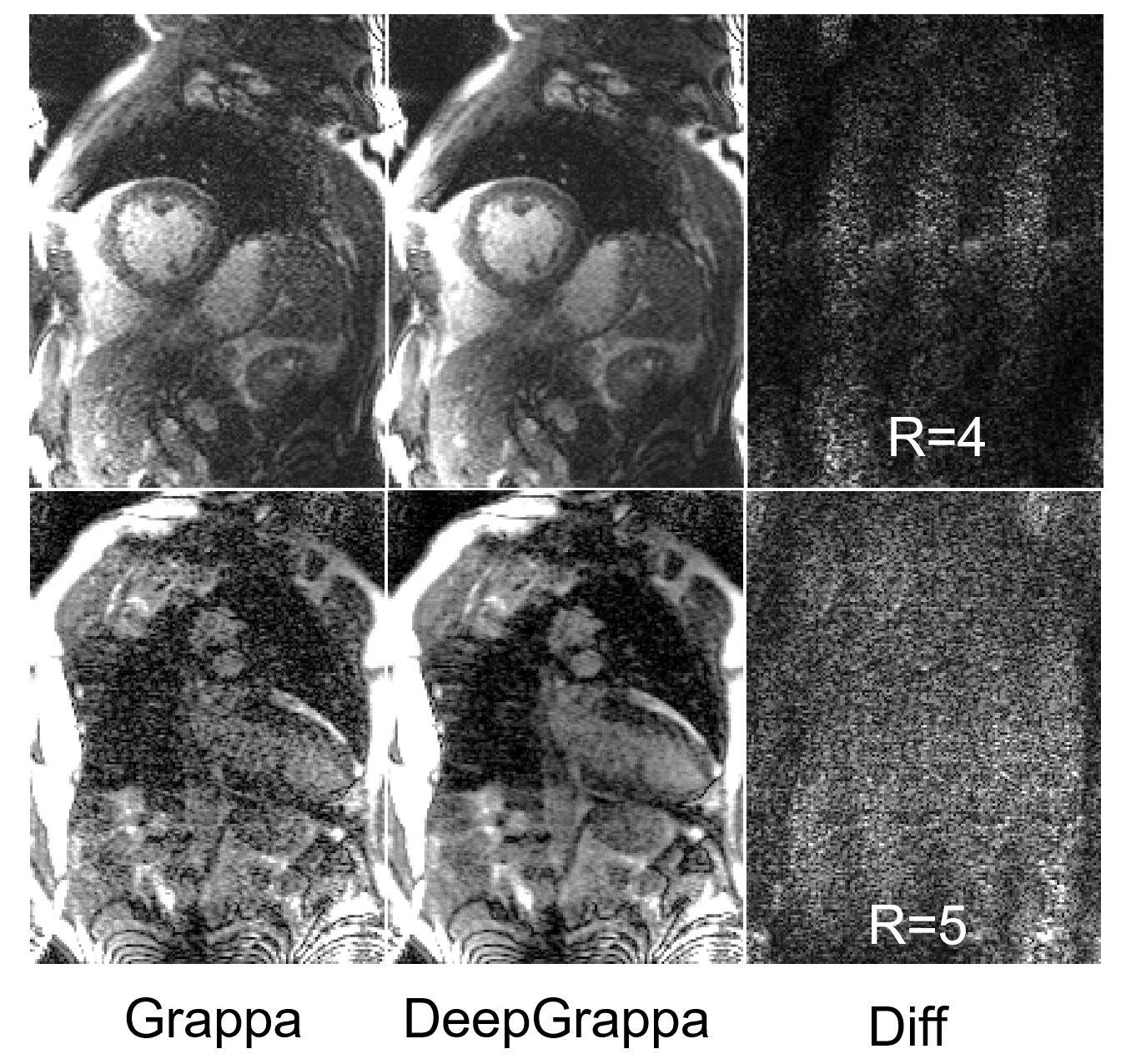
Figure 3 gives example reconstruction for tested real-time cine scans. In both R=4 and 5 cases, proposed method generated improved image quality for noticeably increased SNR. The difference between linear grappa recon and DeepGrappa recon is noise-like with structure reflecting the noise amplification due to inverse (g-factor). The inline reconstruction took ~20s, including training and applying NN to incoming imaging data, on GPU (NVIDIA GTX 2080Ti).Conclusion
A novel AI based MR reconstruction algorithm is proposed. This method is self-calibrated and utilized a design of residual neural network, encouraging to learn over Grappa calibration for beyond linear functional space. Initial validation showed improved image quality can be achieved, without introducing anatomically structured features.Acknowledgements
No acknowledgement found.References
[1] Vahid Ghodrati. MR image reconstruction using deep learning: evaluation of network structure and loss functions. Quantitative Imaging in Medicine and Surgery. 2019;9(9):1516-1527.
[2] Mark A. Griswold, et al. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med. 2002;47:1202–1210.
[3] Mehmet Akçakaya, et al. Scan‐specific robust artificial‐neural‐networks for k‐space interpolation (RAKI) reconstruction: Database‐free deep learning for fast imaging. MRM 81 (1), 2018, 439-453.
[4] Xue H, et al. Gadgetron Inline AI : Effective Model inference on MR scanner. In: ISMRM 2019. p. 4837.
Figures