3562
Intelligent Knee MRI slice placement by adapting a generalized deep learning framework1GE Global Research, Niskayuna, NY, United States, 2GE Healthcare, Bangalore, India, 3GE Healthcare, Rio de Janeiro, Brazil, 4GE Healthcare, Waukesha, WI, United States
Synopsis
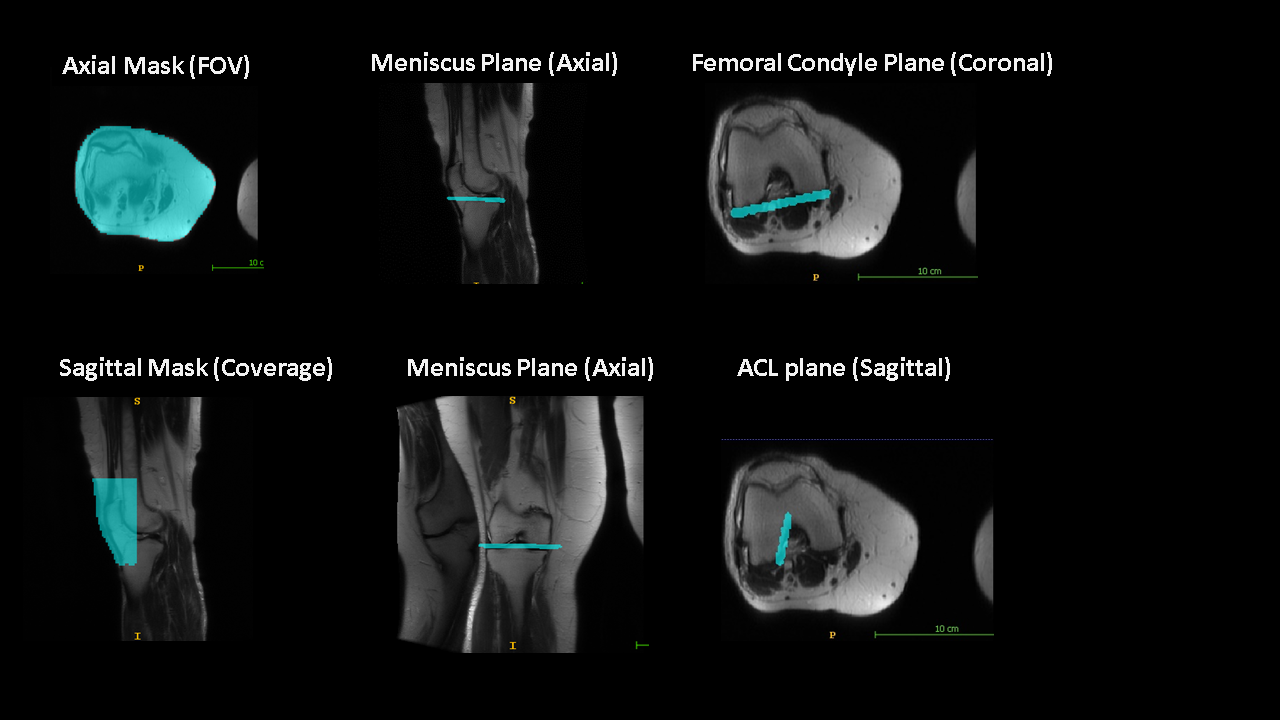
We demonstrate a deep learning-based workflow for intelligent slice placement (ISP) in MR knee imaging: meniscus plane, femoral condyle plane, tibial plane, sagittal plane and ACL plane, based on standard 2D tri-planar localizer images. We leveraged a previously described generalized architecture for ISP planning in brain, with only the training data and plane definitions adapted for knee. The mean absolute distance error between GT plane and predicted plane was < 0.5 mm for all planes except tibial plane (~ 1 mm). The results indicate the generalization of deep-learning ISP framework and its suitability for ISP in any anatomy of interest.
Introduction
Automation of MRI scan plane prescription allows for contiguous visualization of anatomical landmarks; irrespective of changes in patient pose, minor anatomical changes and technologist training. Previous efforts to automate prescription include use of specialized 3D localizers and landmark detection or more recently use of deep based generalized framework for MRI scan plane prescription1,2. In this work, we adapted the workflow described in previous work2 to enable intelligent slice placement (ISP) for knee MRI with multiple knee landmarks: meniscus plane for axial planning, femoral condyle plane for coronal planning, tibial plane for coronal planning , anterior cruciate ligament (ACL) plane for sagittal planning, and default sagittal plane (assumed to be the plane orthogonal to coronal femoral condyle plane). The framework allows all the plane prescription to be done on standard 2D tri-planar localizer images; thereby simplifying the knee imaging workflow. We adapted the DL based framework as is, only making changes for the knee data and the associated landmark planes. Results are presented for the four knee landmark planes.Methods
Subjects: Knee MRI data for study came from multiple sites. A total of 513 knee exams from volunteers as well as patients were included in the study. All the studies were approved by respective IRBs.MRI Scanner and Acquisition: Localizer Data was acquired on multiple MRI scanners (GE 3T Discovery MR 750w, GE Signa HDxt 1.5T, GE 1.5T Optima 450w, GE Signa Premier 3.0T, GE Signa Architect 3.0T and GE Signa Pioneer 3.0T) and with different coil configurations (e.g. 16- and 18-channel TR Knee coil, 16-channel TDI AA coil , GEM Flex coil, 30 channel AIR AA coil, 20 and 21-channel Multipurpose AIR coil etc.). Localizer data had variations in contrast (GRE, SSFSE), image resolution and matrix size across subjects.
Entire Knee ISP workflow was implemented on clinical scanners (1.5T and 3T GE Signa MRI scanners).
DL Methodology: DL-CNN classification and segmentation networks as described in Ref. [2] were adapted with three different sets of DL-CNNs, as described below.
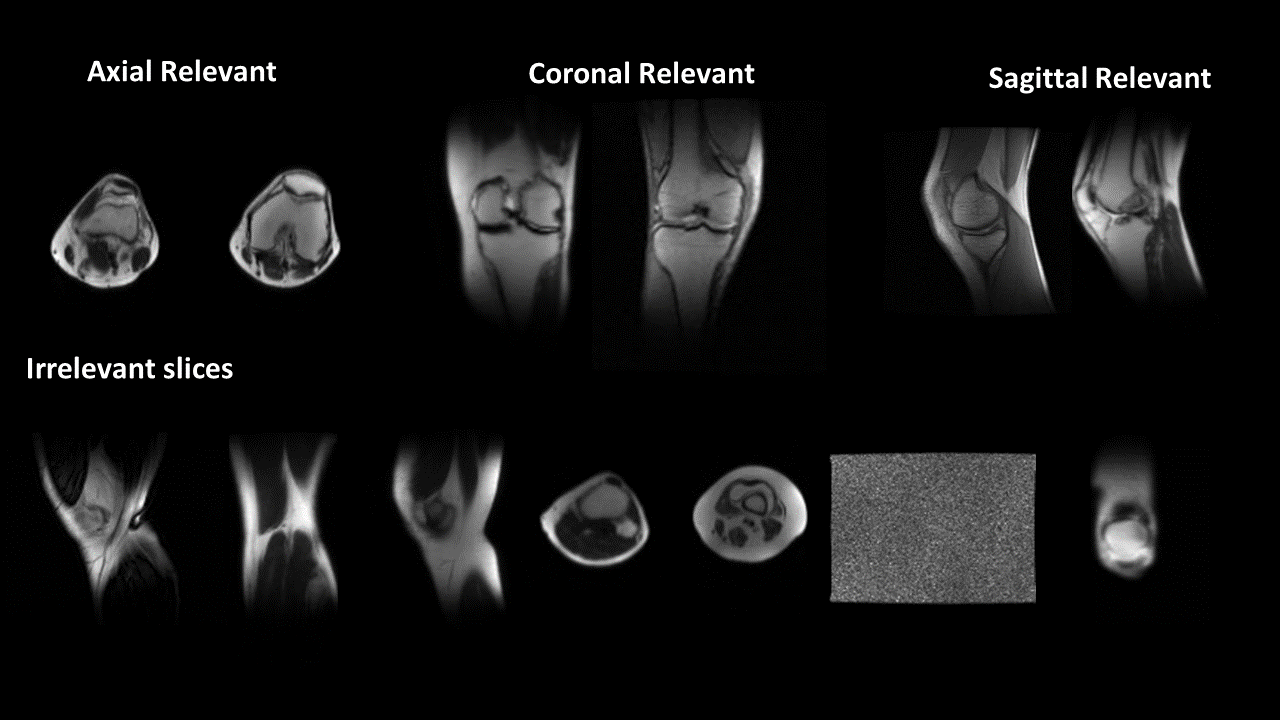
LocalizerIQ Net labels: LocalizerIQ-Net was trained to identify the relevant knee axial, sagittal and coronal images as well as irrelevant images, non-knee and noise data (Fig. 1). A total of 24250 slice images were used for training/validation (augmentation performed) and testing done on 1050 images.
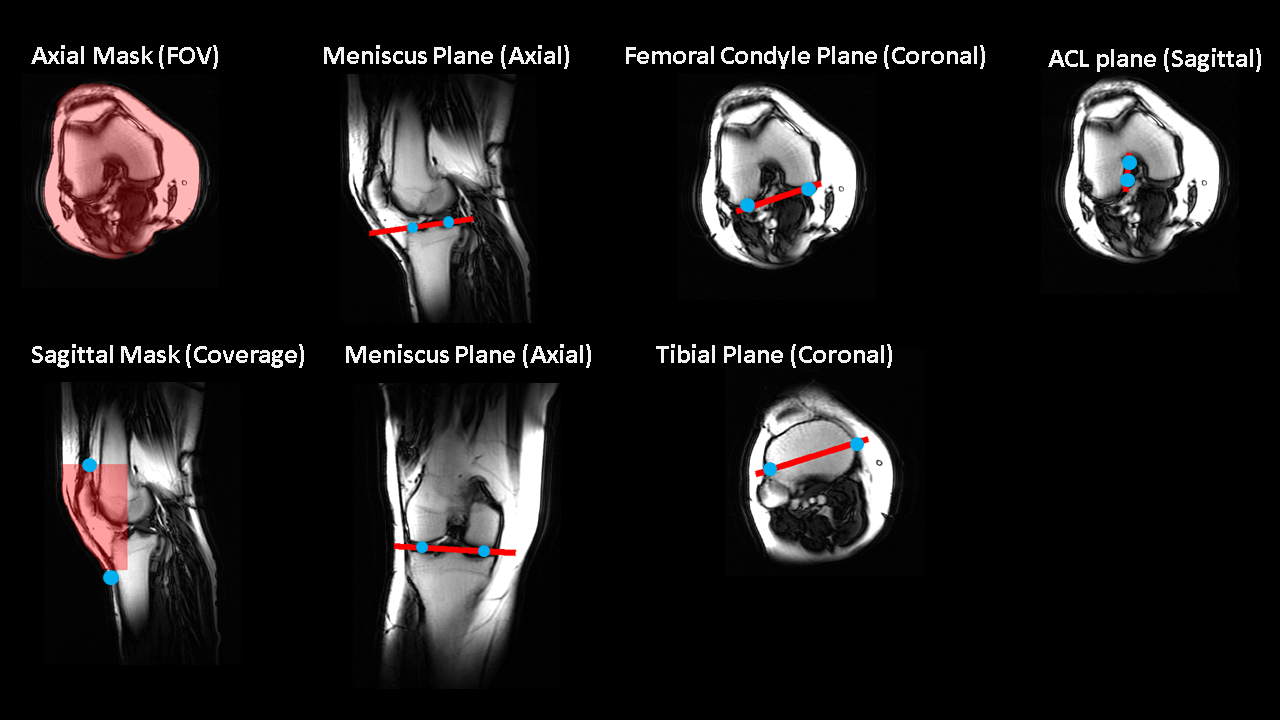
Data for Coverage-Net and Orientation-Net: Ground-truth (GT) landmark points were marked by a trained radiologist and then translated into multiple imaging planes for DL segmentation (Fig.2). A total of 20100 volumes (402 cases and augmented) were used for training/validation and 222 volumes (111 cases) were used for testing.
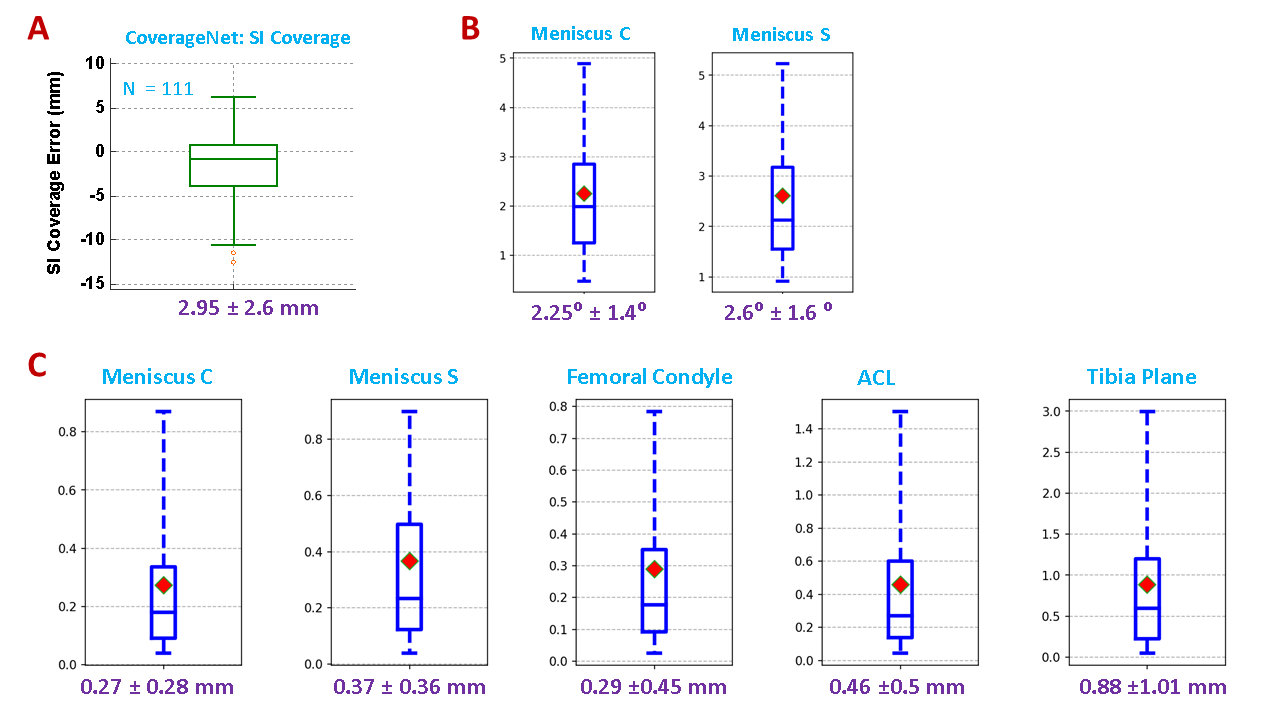
Accuracy Assessment: For LocalizerIQ-Net, label classification accuracy. For Coverage-Net in axial orientation, Dice score was used as accuracy metric and dice > 95% was considered acceptable. For Coverage-Net in sagittal orientation, center error along SI direction was used as accuracy metric (< 3 mm error was considered acceptable). For Orientation-Net, accuracy was assessed by calculating mean absolute distance (MAD) error and angle error between GT and DL-predicted planes for all the landmarks. MAD error < 1 mm and angle-error < 3⁰ was considered as acceptable for ISP.
Results and Discussion
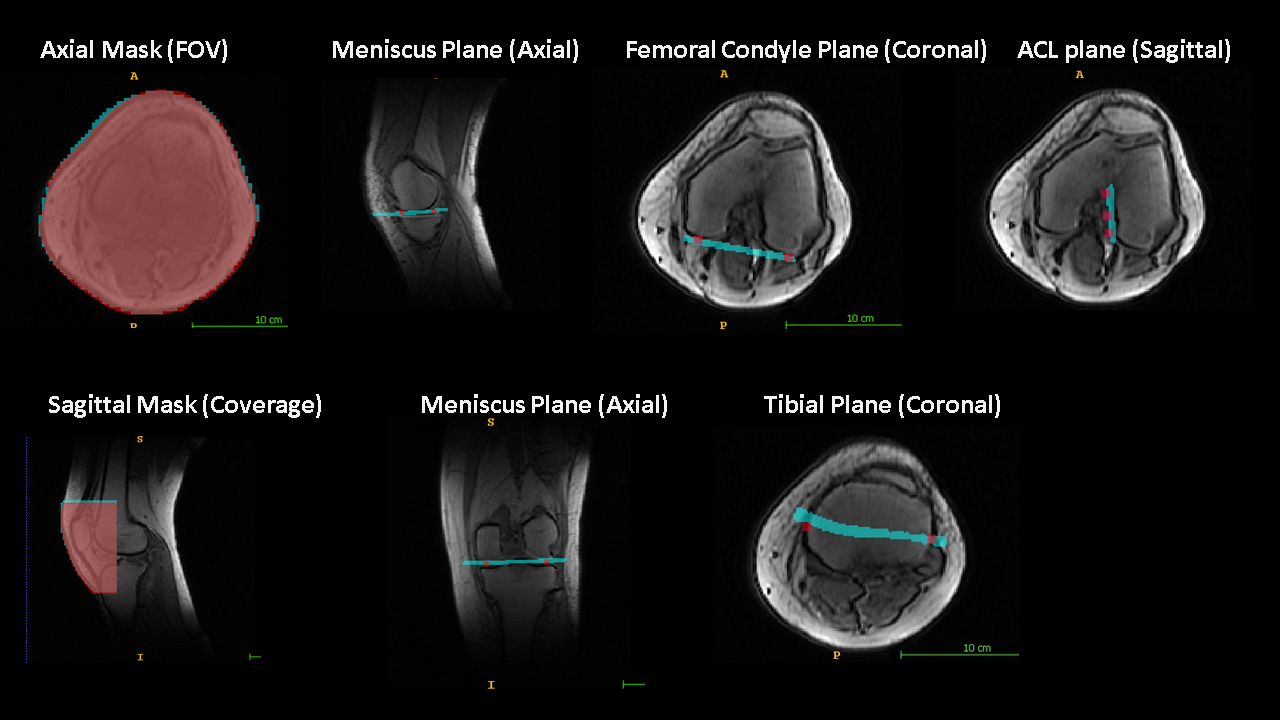
For LocalizerIQ-Net, classification accuracy was 90%. Most of the errors were concentrated in the extreme slices transitioning between anatomically relevant and irrelevant data. Fig.3 shows the results in a sample case. For Coverage-Net, in axial orientation, the dice score was ~ 98% indicating excellent FOV information. For sagittal Coverage-Net, the mean center error along SI direction was 2.95 mm ±2.6 mm (fig. 4A), and ensured that slice coverage always extends between patella and patellar tendon. Angle error for meniscus plane was 2.6⁰ and is within the acceptable range for knee imaging. For Orientation-Net, MAD error was < 0.5 mm for all planes except tibial plane (~ 1 mm) (fig. 4). Tibial plane segmentation is non-trivial due to lack of specific internal features and smother outer surface (See fig. 3). Consequently, the errors were higher; though within acceptable limits. The generalized framework provided robust knee plane prediction; even in presence of wrap-around artifacts in localizers (fig. 5).Conclusion
We adapted a generalized DL-based intelligent slice placement framework for four commonly used knee landmarks. The results indicate that framework allows for successful knee landmark plane prescription, which can be used in clinical practice; even with presence of artifacts in localizer data. Overall, we surmise that the framework can be extended for ISP in terms of additional landmarks in knee or any other anatomy.Acknowledgements
No acknowledgement found.References
1. Lecouvet FE, Claus J, Schmitz P, Denolin V, Bos C, Vande Berg BC. Clinical evaluation of automated scan prescription of knee MR images. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2009 Jan;29(1):141-5.
2. Shanbhag DD et.al. A generalized deep learning framework for multi-landmark intelligent slice placement using standard tri-planar 2D localizers. In Proceedings of ISMRM 2019, Montreal, Canada, p. 670.
Figures