3485
Rapid 3D Navigator-Triggered MRCP With SPACE Sequence at 3T: Only One-third Acquisition Time of Conventional 3D Navigator-Triggered MRCP.1Radiology, Union Hospital, Fujian Medical University, Fuzhou, China, 2Diagnostic imaging, Siemens Healthcare, Shanghai, China., shanghai, China, 3MR application, Siemens Healthineers Ltd,Guangzhou,China, guangzhou, China
Synopsis
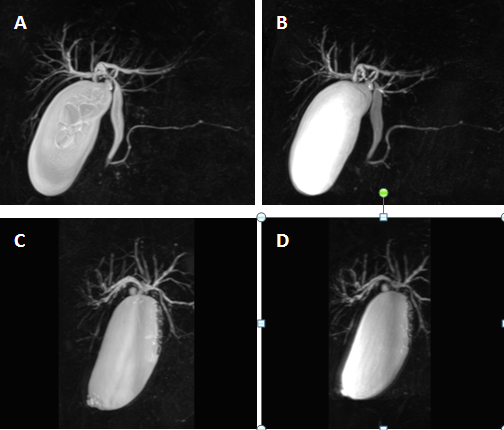
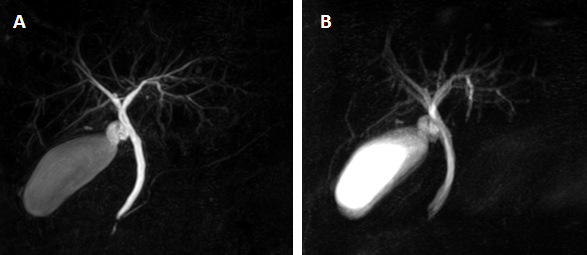
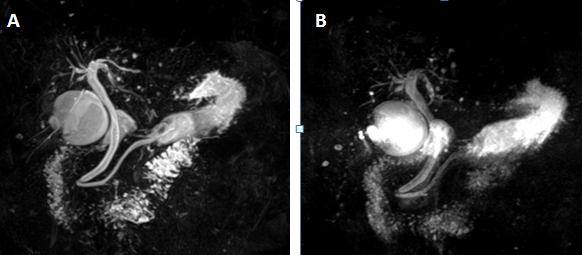
The SPACE sequence based rapid MRCP protocol proposed in this study, which reduced acquisition time without deteriorating the image quality, yielded significantly higher overall image quality and better visualization of the pancreaticobiliary tree compared with the conventional MRCP. On the basis of our findings, we suggest that the rapid 3D SPACE technique could improve the clinical throughput of MRCP and show a trend toward wider clinical availability for MRCP studies.
Purpose
The purpose of this study was to compare the image quality and acquisition time between a 3D respiratory-triggered MRCP sequence with fast imaging techniques and the conventional 3D heavily T2-weighted sequences.Materials and methods
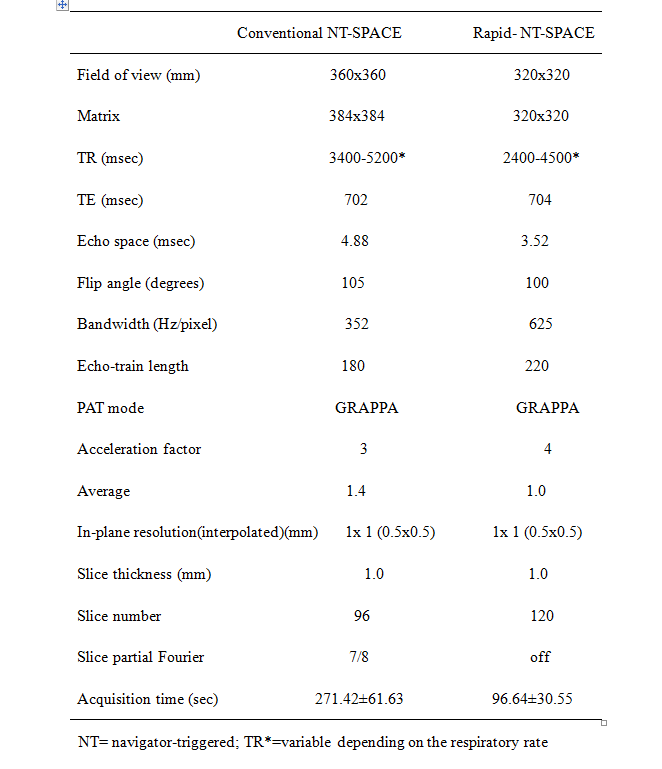
Materials and methods: Between January 2019 and May 2019, a total number of 67 consecutive patients with suspected pancreaticobiliary diseases were included in this prospective study. All MRCP patients were performed on a whole-body 3T MR system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) in the supine position using an 18-channel body matrix coil combined with 12-channal spin matrix coil. Conventional 3D MRCP in an oblique coronal orientation was acquired using SPACE sequence with a navigator-triggered manner, followed by the proposed rapid-MRCP scheme. Both sequences were performed before contrast media administration. Patients fasted for at least 4 hours before MR imaging. The application of a negative oral contrast agent was performed to suppress fluid signal in the stomach and duodenum prior to the examination unless a contraindication. The parameters for MRCP imaging are summarized in Table 1. The acquisition time for both sequences was recorded. Two blinded radiologists performed qualitative analyses with respect to overall image quality, motion artifacts and CBD visibility using a 4-point scale. Quantitative evaluation included the contrast, signal-to-noise-ratio (SNR), and contrast-noise-ratio (CNR) between the common bile duct (CBD) and periductal tissues. A paired t-test was used to assess differences in the qualitative and quantitative evaluations between two acquisition methods.Results
All MRCP studies were completed successfully. The mean acquisition time of rapid-NT-MRCP (96.64±30.55s) was significantly lower than that of the conventional NT--MRCP (271.42 ± 61.63 s; P < 0.001).The contrast ratio, SNR and CNR of the CBD were significantly higher for conventional NT-MRCP than with rapid NT-MRCP images (0.95±0.02 vs 0.93±0.03, P<0.001; 10.36±4.63 vs 8.90±4.71, P=0.011; 14.01±6.02 vs 12.22±6.36, P=0.020, respectively). The rapid MRCP depicted the overall image quality, artifacts, CBD visibility, right and left hepatic duct, segment 2 branch, main pancreatic duct and cystic duct significantly better compared with conventional MRCP (P<0.05). There were no statistically significant differences between the two methods regarding visibility of anterior and posterior and segment 3 branches (P>0.05).Conclusions
In conclusion, the proposed rapid MRCP protocol yielded significantly higher overall image quality and better visualization of the pancreaticobiliary tree with a significantly reduced imaging time without deterioration of image quality compared with the conventional MRCP at 3T.Acknowledgements
We thank Guijin Li and Zhongshuai Zhang of MR application Siemens Healthineers Ltd China for the technical support.References
1. Mazziotti S, Costa C, Ascenti G, GaetaM, Pandolfo A, Blandino A. MR cholangiopancreatography diagnosis of juxtapapillary duodenal diverticulum simulating a cystic lesion of the pancreas: usefulness of an oral negative contrast agent. AJR Am J Roentgenol 2005;185:432–435
2.Nakaura T, Kidoh M, Maruyama N, et al. Usefulness of the SPACE pulse sequence at 1.5 T MR cholangiography: comparison of image quality and image acquisition time with conventional 3D-TSE sequence. J Magn Reson Imaging.2013;38:1014–1019.
3.Sodickson A, Mortele KJ, Barish MA, et al. Three-dimensional fast-recovery fast spin-echo MRCP: comparison with two-dimensional single-shot fast spin-echo techniques. Radiology. 2006;238:549–559.
4. Nandalur KR, Hussain HK, Weadock WJ, et al. Possible biliary disease: diagnostic performance of high-spatial-resolution isotropic 3D T2-weighted MRCP. Radiology 2008;249:883–890.
Figures