3355
Head motion estimation and correction using slab-selective FIDnavs1Department of Radiology and CIBM, University of Geneva, Geneva, Switzerland, 2Department of Radiology, Boston Children's Hospital and Harvard Medical School, Boston, MA, United States, 3Advanced Clinical Imaging Technology, Siemens Healthcare, Lausanne, Switzerland, 4Department of Radiology, UNIL and CHUV, Laussanne, Switzerland, 5LTS5, EPFL, Lausanne, Switzerland
Synopsis
In this work, we propose to measure and correct rigid body head motion using slab-selective FID navigators. It is possible to estimate motion without relying on any
Purpose/Introduction
The localized sensitivity profiles of multi-channel coil arrays provide spatial encoding information that enables quantitative estimation of rigid body head motion using FID-navigators (FIDnavs)1,2. Previous work demonstrated that it is possible to estimate motion without relying on patient-specific choreographic training by using simulated motion data and a forward model of FIDnav signal generation3. This calibration procedure provides a more practical solution, particularly for pediatric applications where subjects are unable to cooperate with specific instructions. As the FIDnav measures signal from the entire excited volume, a limitation of measuring non-selective FIDnavs, is that the FIDnav is sensitive to signals from the neck and jaw region, which do not move rigidly with the head. In this work, we propose using slab-selective FIDnav excitation to estimate rigid body head motion by extending the forward model to include an accurate model of the slab excitation profile.Methods
Data acquisitionThree volunteers were scanned at 3T (MAGNETOM Trio a Tim System, Siemens Healthcare, Erlangen, Germany) using a 32-channel head coil, after providing written informed consent. Three low-resolution reference images were acquired including a large slab-selective (64 partition encodes) image with both surface and body coils, and a small slab-selective (32 partition encodes, with 100% oversampling) image with the body coil using a 3D FLASH sequence (TR=12ms, TE=2.25ms, 4-mm isotropic resolution axial images). A prototype 3D FLASH sequence was modified to include an FIDnav readout (TNAV=2.25ms) every TR after the slab-selective RF pulse.
Three FID-navigated high-resolution 3D FLASH images were acquired for each volunteer with i) no motion (reference); ii) abrupt head motion every minute; iii) slow head-shaking motion every minute. Images were acquired with the following parameters: 1-mm isotropic axial images with TR=12ms, TE=5.53 ms, FA=30°, RBW=400 Hz/pixel, FOV=256x256x128mm. The center of the FIDnav ADC and the TE of the low-resolution reference images were matched for calibration purposes. Motion measurements were also recorded using electromagnetic (EM) tracker4 (Robin Medical, Baltimore, MD) comprising four sensors placed on the volunteer’s forehead for comparison.
Data processing
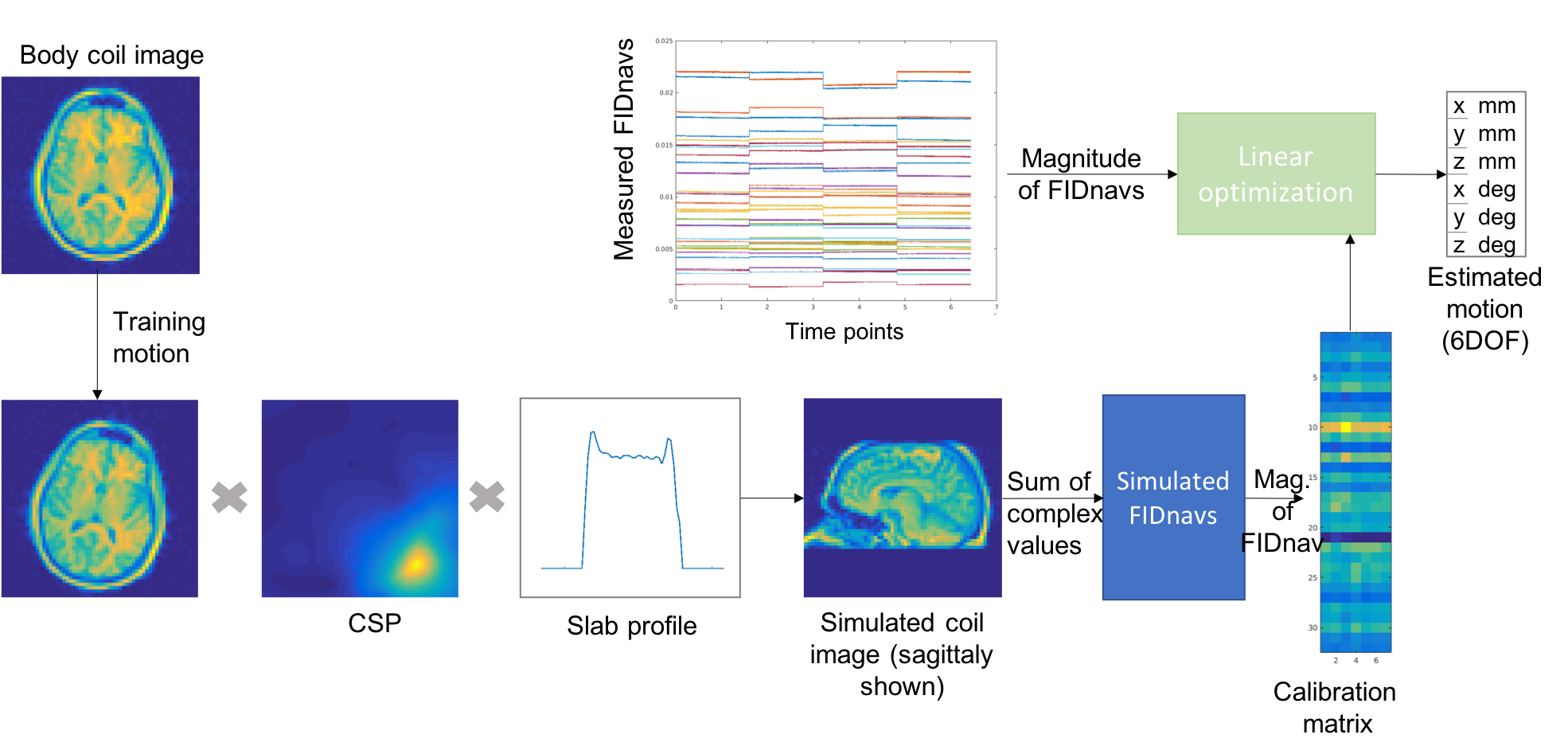
Coil sensitivity profiles (CSP) were computed by taking the ratio of large slab-selective surface and body coil images. Thin-plate spline extrapolation was applied to create a model of the CSPs. The slab profile was computed from the ratio of the small- and large-slab body coil images. FIDnavs were simulated by taking the complex sum of an image simulated by point-wise multiplication of the large-slab body coil image, the extrapolated CSPs and the slab profile (Figure 1). A calibration matrix was created by simulating 1mm/1° motion in 6 degrees-of-freedom applied to the reference body coil image and computing the absolute FIDnav in each position. The resulting inverse problem was solved using least squares fitting to estimate rigid body head motion at each time point. The flowchart of the algorithm can be seen in Figure 1.
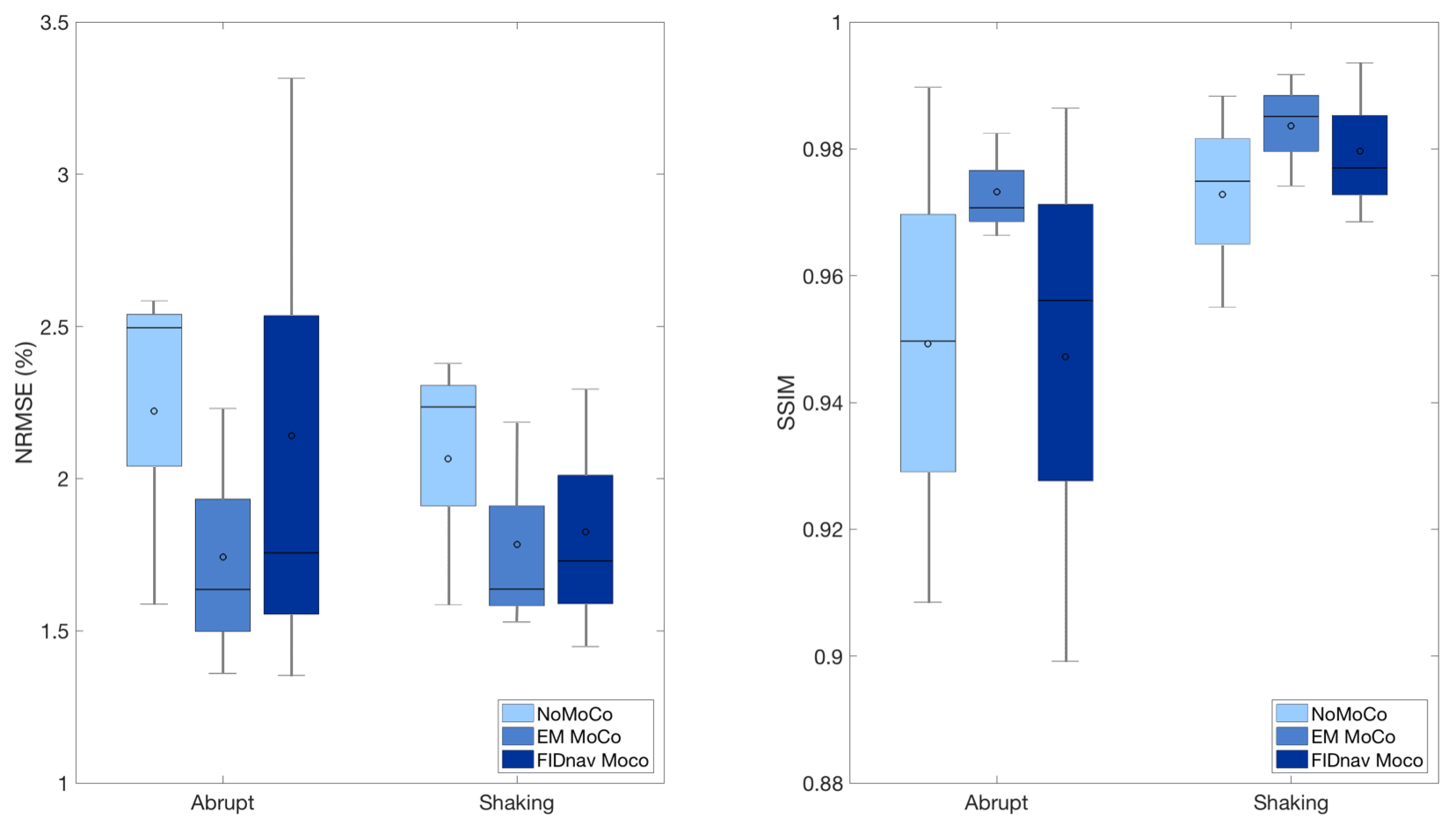
The estimated rigid-body motion from both EM tracking and FIDnavs was used to retrospectively correct the acquired k-space data5. Each image was registered to the corresponding no motion image and normalized root mean square error (NRMSE) and structural similarity index (SSIM) were computed relative to the no motion image to evaluate the improvement in image quality achieved by retrospective correction.
Results
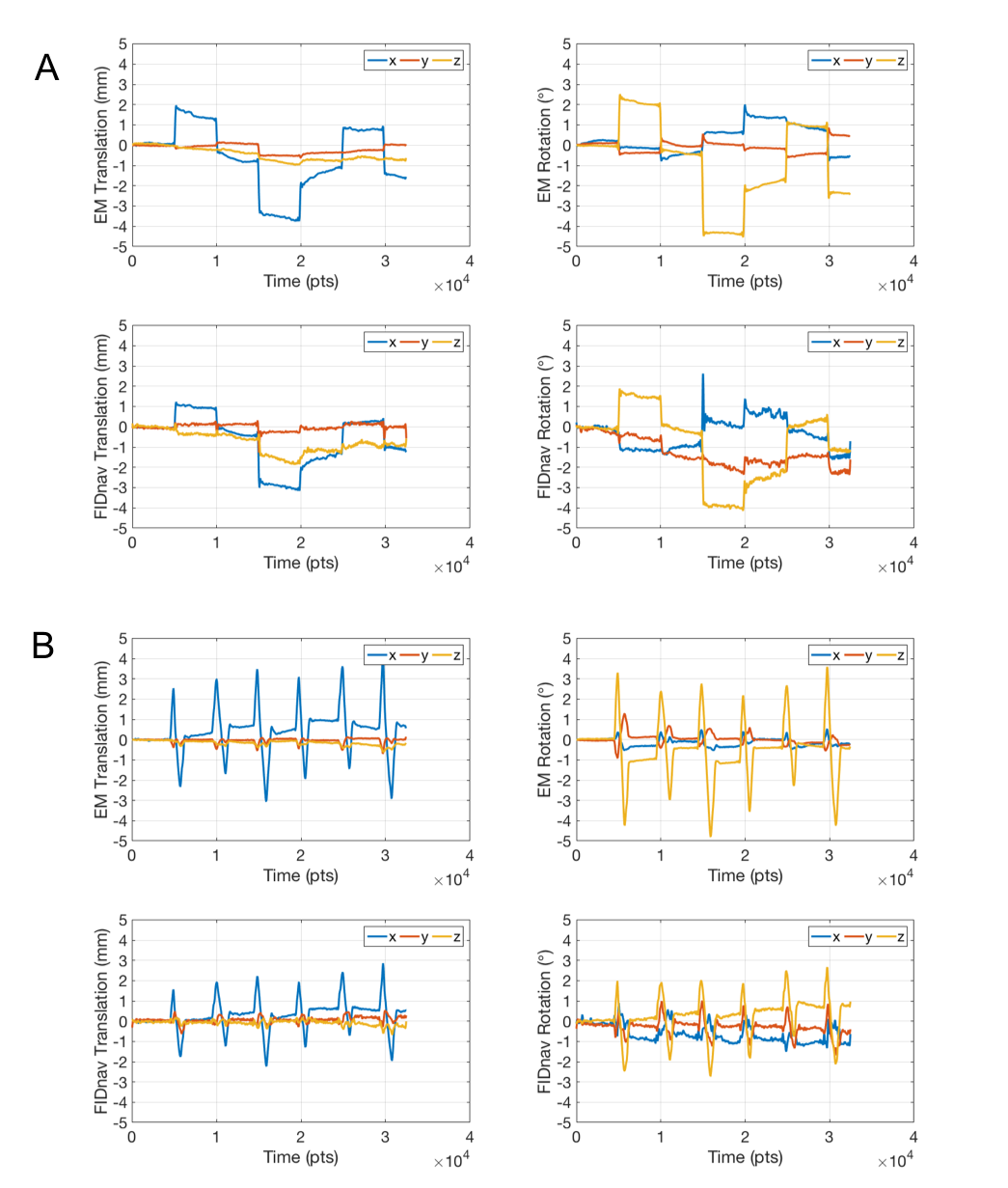
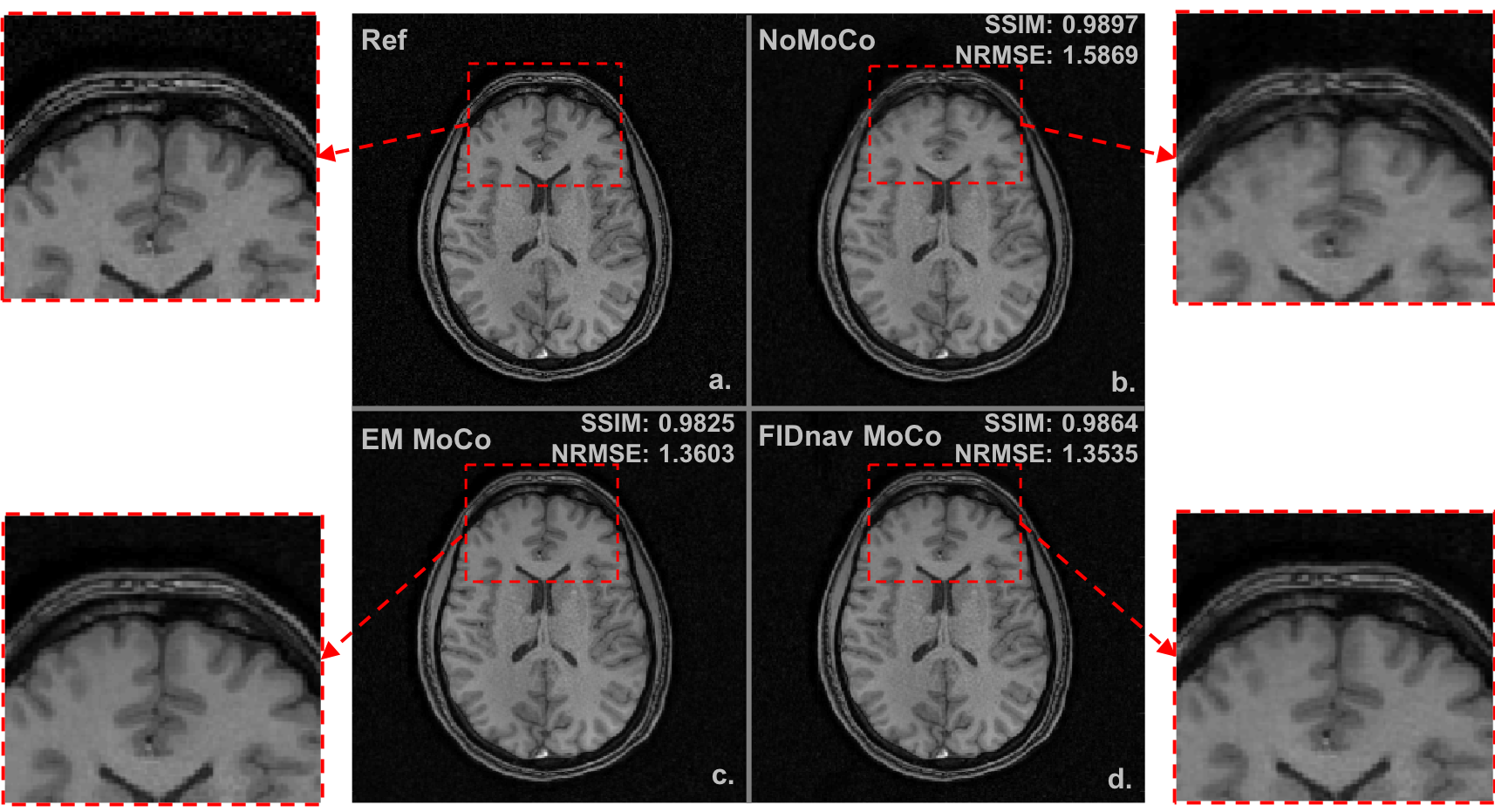
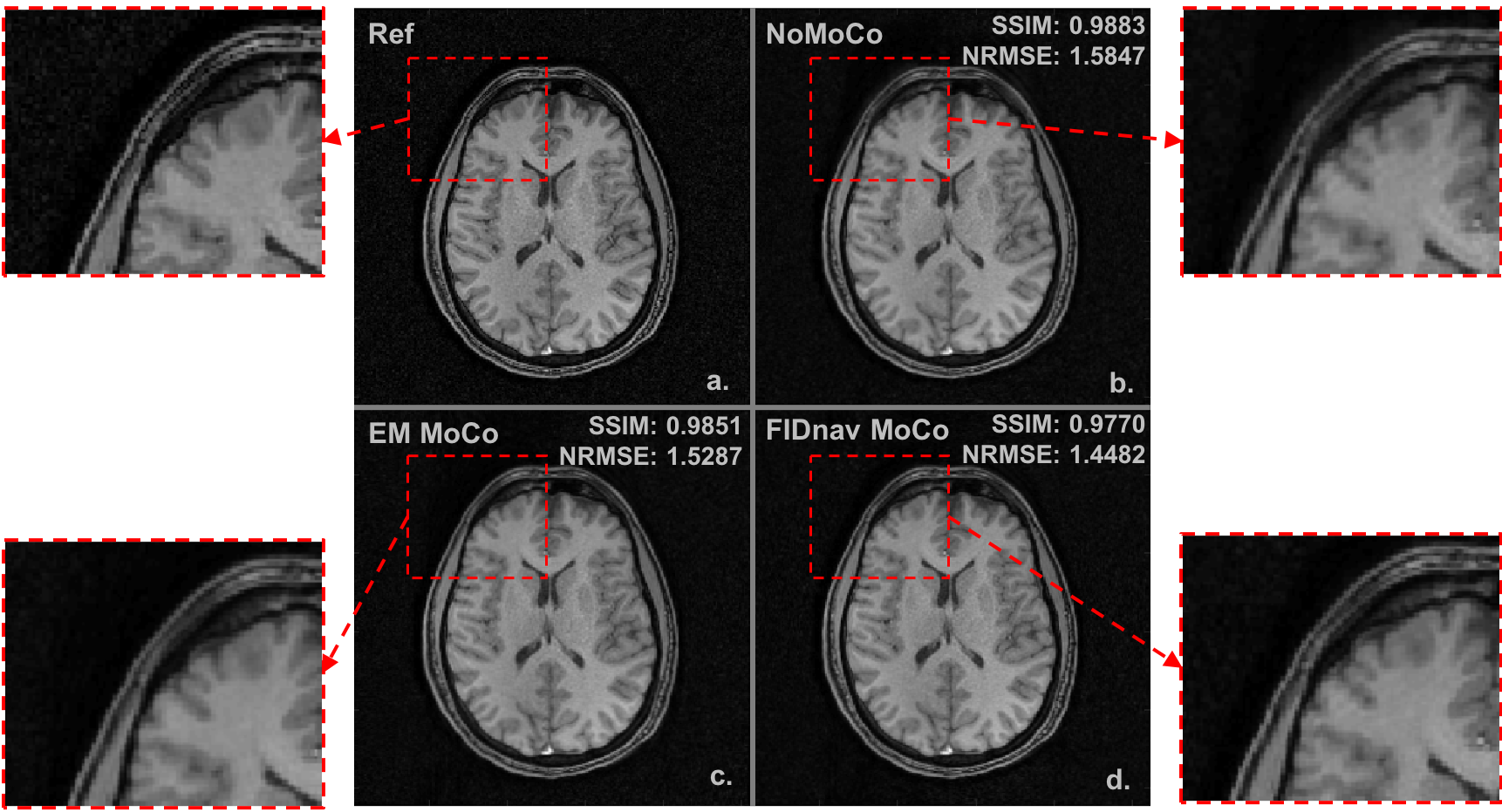
Figure 2 shows a comparison of translational and rotational motion estimations from FIDnavs and EM tracking of a volunteer performing (A) abrupt head motion every minute with accuracy and precision for translation and rotation 0.3±0.2mm 0.9±0.6° and (B) slow head-shaking motion once every minute with accuracy and precision for translation and rotation 0.2±0.2mm 0.6±0.4°. For head-shaking motion, FIDnav estimates are in good agreement with external tracking.Figures 3 and 4 show retrospective motion correction for one volunteer performing abrupt head motion and slow head-shaking motion, respectively. In both figures (a) no motion reference image, (b) uncorrected head motion (c) retrospectively corrected image using EM tracker and (d) retrospectively corrected image using FIDnav.
Figure 5 shows quantitative image metrics of NRMSE and SSIM for abrupt head motion and slow head-shaking motion. For head-shaking motion, FIDnav-based correction substantially reduced NRMSE and improved SSIM, with results comparable to EM tracking. Correction for abrupt head motion was more variable.
Discussion
This study demonstrates the ability of slab-selective FIDnavs to provide rigid-body motion estimates without the need for patient-specific choreographed training by extending the forward model to include slab excitation profile. Retrospective correction with FIDnav motion estimates improved structural image quality in the presence of continuous head-shaking motion. The reasons for the variability in abrupt motion could be breakdown of the model assumptions in the presence of large amplitude motion. Shaking motion is largely within the slab which could be a reason why the estimations are more accurate. Through-slab motion may introduce small artifacts due to changing signal intensities at the edge of the slab profile. FIDnavs are an attractive approach for imaging babies as they do not require any external hardware. Navigators can be acquired rapidly with a minimal impact to the overall scan time. Slab-selective FIDnavs can be suitable for neonatal imaging due to ability of exciting only head region which can be assumed to move rigidly.Acknowledgements
This research was supported by Swiss National Foundation Doc.Mobility grant. Project number: P1GEP2_184160References
1. Kober T, Marques JP, Gruetter R, Krueger G. Head motion detection using FID navigators. Magn Reson Med. 2011;66:135- 143.
2. Babayeva M, Kober T, Knowles B, Herbst M, Meuli R, Zaitsev M, Krueger G. Accuracy and precision of head motion information in multi-channel free induction decay navigators for magnetic resonance imaging. IEEE Trans Med Imaging. 2015;34:1879-1889.
3. Wallace TE, Afacan O, Waszak M, Kober T, Warfield SK. Head motion measurement and correction using FID navigators. Magn Reson Med. 2018;00:1–17. https://doi.org/10.1002/mrm.
4. Afacan, O, Wallace, TE and Warfield, SK (2019). Retrospective correction of head motion using measurements from an electromagnetic tracker. Magnetic Resonance in Medicine.
5. Fessler JA. Michigan Image Reconstruction Toolbox.
Figures