3353
Reduced Motion Artifact in Super Resolution T2 FSE Multislice MRI: Application to Prostate1Mayo Graduate School, Rochester, MN, United States, 2Mayo Clinic, Rochester, MN, United States, 3Mayo Clinic, Scottsdale, AZ, United States
Synopsis
T2-weighted fast spin echo is acquired in virtually all clinical MRI exams; however, it has coarse through-plane vs. in-plane resolution and is thus often acquired in multiple orientations. This extends the exam time. We have shown improved through-plane resolution in T2 FSE prostate MRI by acquiring overlapped slices and accounting for the slice profile in the reconstruction. Due to acquisition of overlapped slices in several passes, an artifact was observed in the reformatted images, due to subtle peristaltic motion. We propose acquiring the phase encoding lines in several segments to suppress the motion artifact observed in the reformatted images.
Introduction
Use of overlapped slices for super resolution has previously been proposed in 2D T2-weighted spin-echo (T2SE) multislice acquisition [1, 2]. To avoid slice-to-slice interference effects the acquisition is typically subdivided into several multislice “passes” in which consecutive slices sampled within a pass are adequately separated to avoid slice-to-slice interference. Combination of the slices from all passes gives the desired overlapped sampling.For imaging of relatively motion-free regions such as the brain this appears to be adequate [1, 3]. In our own work for prostate MRI [2] we acquired 3 mm thick axial slices with 1 mm slice-to-slice increment using six passes. In vivo results showed improved sharpness in the resultant thin 1 mm axial slices compared to abutting 3 mm thick slices. However, the level of peristalsis-related motion artifact, manifest as discrete steps or scalloping in sagittal or coronal reformats, was higher.
The purpose of this work is to describe how the overlapped slices required for super resolution can be acquired using a modified, segmented, multislice acquisition. We hypothesize that the modified approach substantially reduces the scalloping artifact seen in reformats while retaining overall image quality in the acquired orientation.
Methods
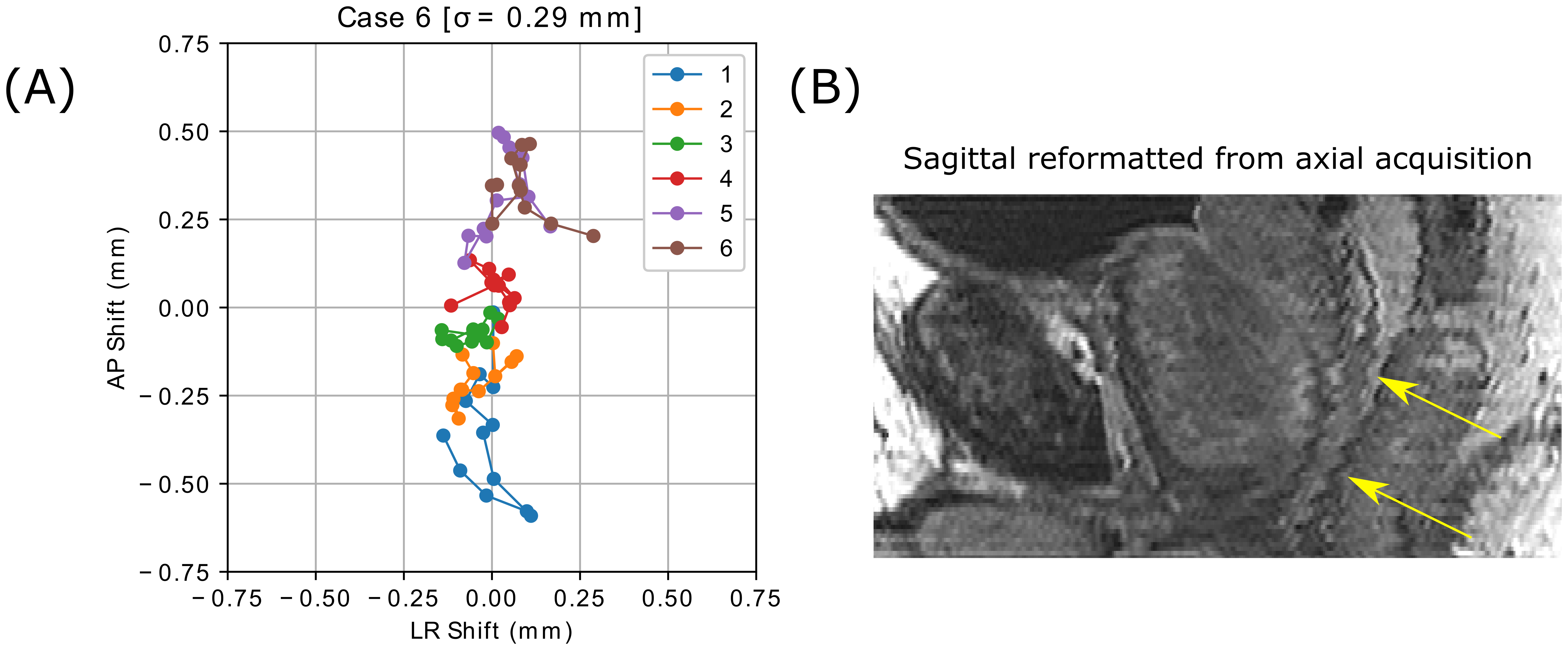
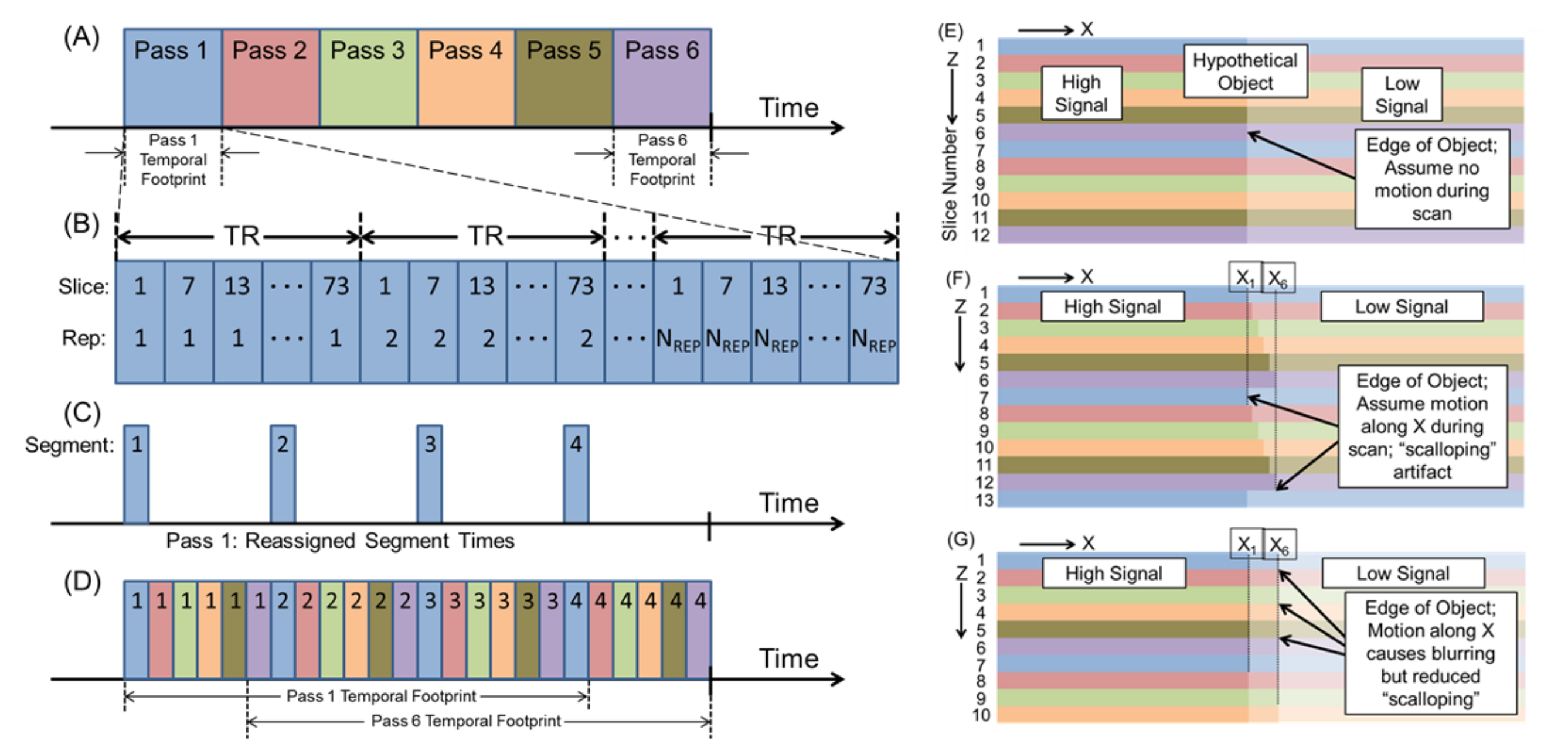
Subtle transverse motion of the prostate during a four-to-six minute long T2 FSE scan is observed to be primarily driven by peristaltic motion in the rectum. This was analyzed by reviewing the 16 prostate exams of Ref. [2] each of which acquired 78 3 mm thick axial slices with 2 mm overlap. Slice-to-slice displacement in the transverse plane was determined by cross correlation of adjacent, overlapped slices. Results for a typical case are shown in Figure 1A, with the displacements for slices within a specific pass shown in an individual color. Also shown is the sagittal (B) reformat formed from the set of overlapped axial images with super resolution applied along the slice (superior/inferior, S/I) direction. The scalloping is clearly evident and objectionable.The artifact can be explained by considering the multi-pass acquisition (Fig.2A). With no motion the slices accurately portray an edge within a presumed object (E) where the slices are color-coded to match their pass of acquisition. However, slight motion along X leads to step-wise scalloping (F) owing to the temporal footprints of Passes 1 and 6 being widely separated in time (A) where the temporal footprint is defined as the time over which data collection for a pass is performed.
In the proposed method the acquisition of the kY-lines in each pass is divided into multiple segments (four as shown for Pass 1 in Fig.2C). Each segment comprises the acquisition of some subset of the NREP repetitions required for full sampling (B). In Fig.2D the segments of all six passes are shown with their color showing the pass, and the number showing the segment number. The new acquisition causes the temporal footprints of all passes to have substantial overlap, leading to improved pass-to-pass consistency of object position but at the possible expense of blurring (G).
The new segmented sequence was evaluated using a motion-controlled resolution phantom to assess possible loss of in-plane resolution vs. the original sequence. To assess performance in vivo, the new segmented and original multislice sequences were compared to 14 male patients under an IRB-approved protocol. Super-resolution axial images and sagittal reformats were evaluated by three experienced uroradiologists.
Results
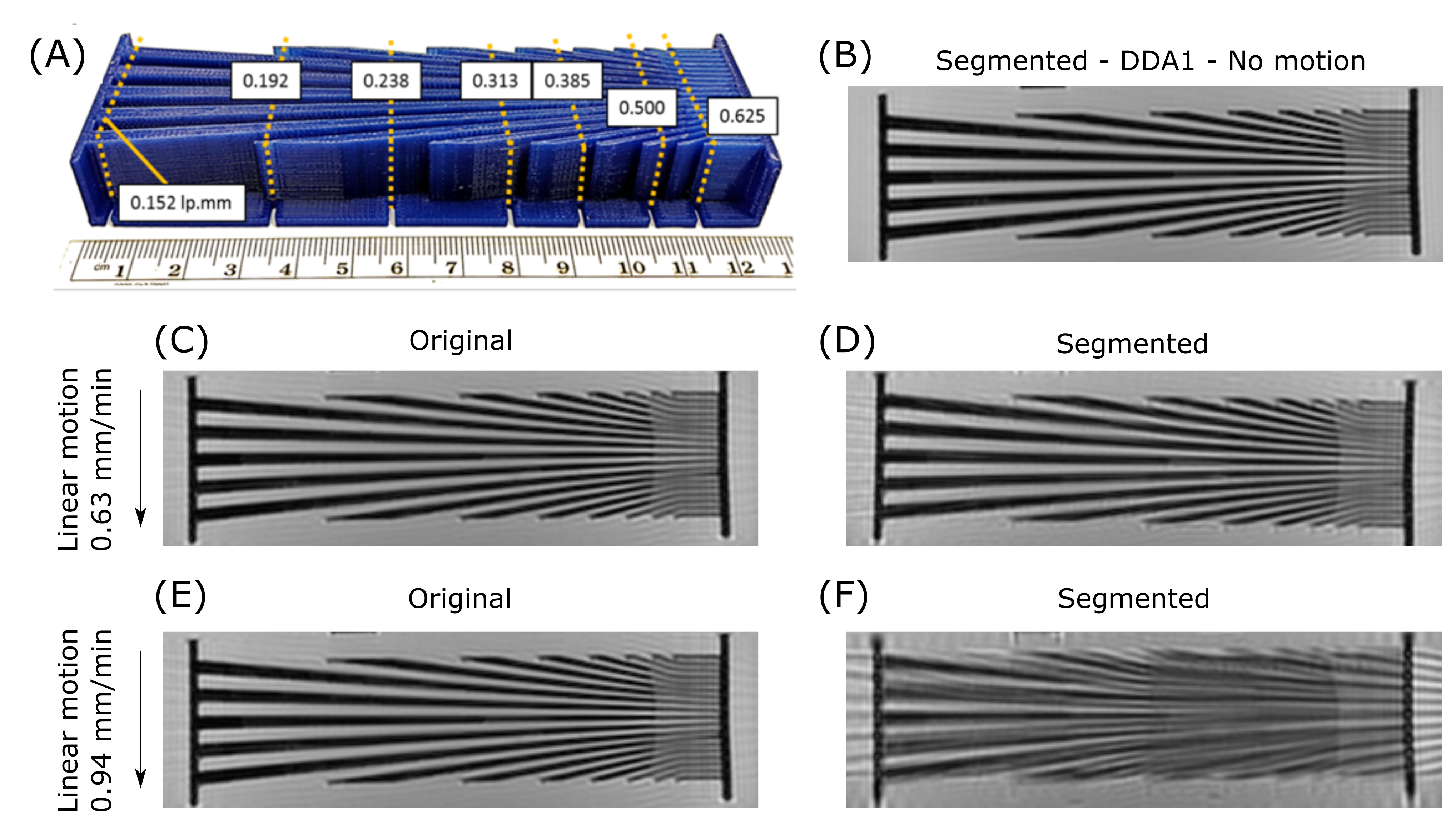
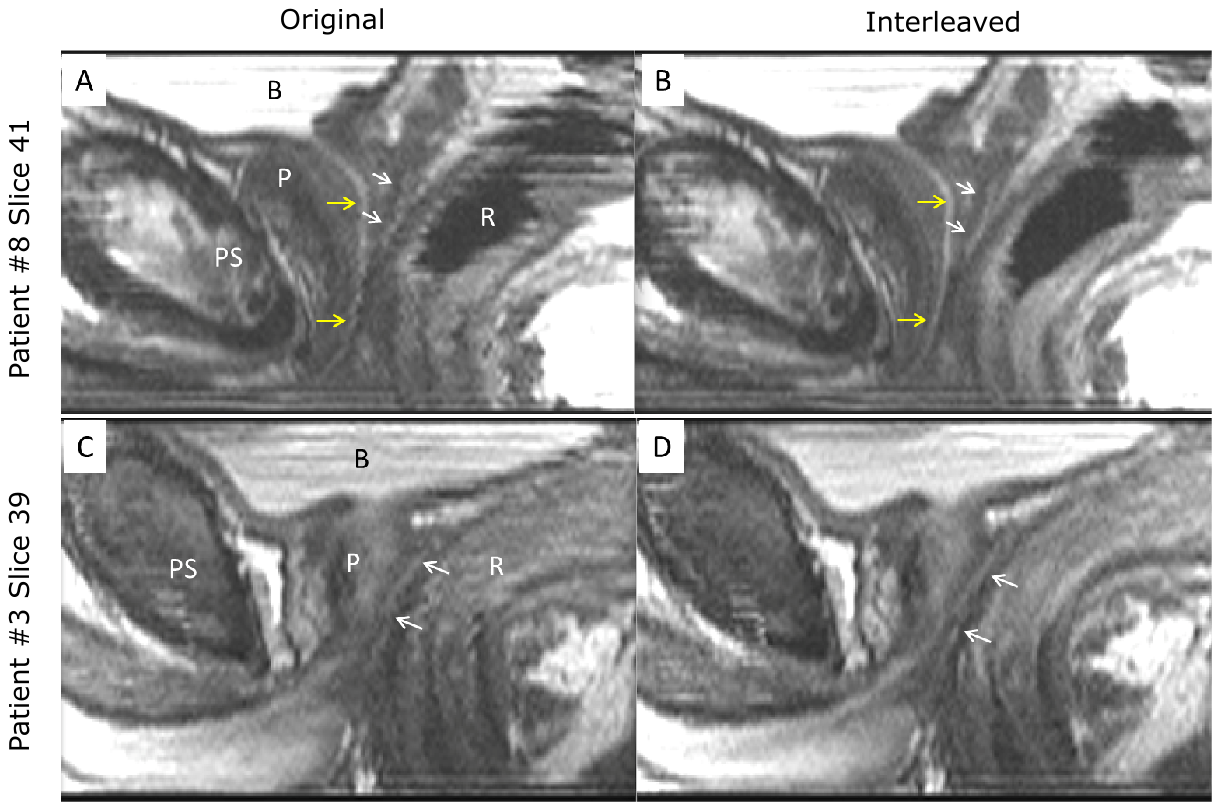
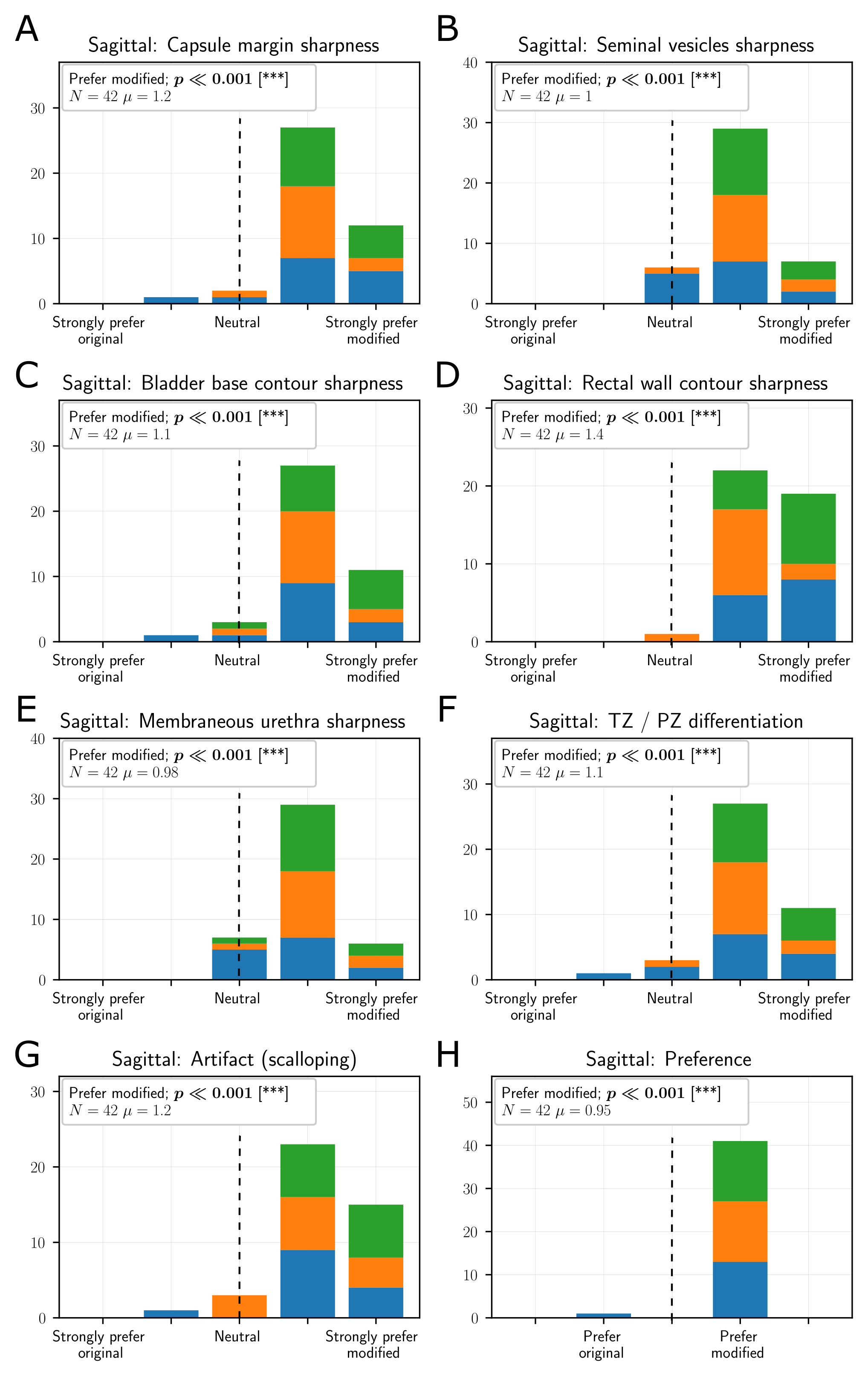
Fig.3 shows a photograph of the resolution phantom (A), an image acquired with the segmented sequence with no motion (B), and images made with the original and segmented sequences for 0.63 mm/min (C, D) and 0.94 mm/min (E, F) motion within the axial plane of acquisition. The temporal footprints for a pass of the original and segmented sequences are approximately 1 min and 7 min for a TR of 3000 msec.Fig.4 compares sagittal reformats from Patient #8 for the original (A) vs. segmented (B) and Patient #3 original (C) vs. segmented (D) acquisitions. For all criteria the sagittal reformats were significantly superior to those from the original (Fig.5), while for the axial images the performance was not statistically different. We thus consider the hypothesis to have been proven true.
Discussion
Fig.3D vs. C shows that in spite of the increased temporal footprint there is negligible loss of in-plane resolution in the segmented vs. the original sequence at the level of motion encountered clinically (approximately 1 mm over 6 min per Fig.1A). At larger motions degradation is observed (Fig.3 F vs. E) as might be expected. In vivo, both visual (Fig.4) and radiological assessment (Fig.5) showed that the new segmented sequence significantly reduces the scalloping artifact and improves image quality in sagittal reformats.Conclusions
For prostate MRI the new segmented acquisition significantly reduces the motion artifact that can be present in sagittal and coronal reformats due to long time lags between the acquisitions of adjacent or overlapped slices. The new method trades off the potential increased sensitivity to in-plane motion manifest as the increased temporal footprint for any one pass, with reduced sensitivity to the objectionable scalloping artifact. The method might be applicable to other applications requiring acquisition of many overlapped or contiguous slices.Acknowledgements
We would like to acknowledge Kathy Brown and Diane Sauter for assistance in the patient studies, Phil Rossman and Thomas Hulshizer for constructing the prostate phantom and motion assembly.References
[1] Greenspan H, Oz G, Kiryati N, Peled S. MRI inter-slice reconstruction using super-resolution. Magnetic Resonance Imaging 2002 Jun;20(5):437–446.
[2] Kargar S, Borisch EA, Froemming AT, Grimm RC, Kawashima A, King BF, et al. Use of k Z -space for high through-plane resolution in multislice MRI: Application to prostate. Magnetic Resonance in Medicine 2019 Jun;81(6):3691–3704.
[3] Barth M, Breuer F, Koopmans PJ, Norris DG, Poser BA. Simultaneous multislice (SMS) imaging techniques. Magnetic Resonance in Medicine 2016 Jan;75(1):63–81.
Figures