3337
Evaluation of precision of the psoas major muscle MR elastography1Department of Radiological Sciences, Tokyo Metropolitan University, Tokyo, Japan, 2Office of Radiation Technology, Keio University Hospital, Tokyo, Japan, 3Human Technology Research Institute, National Institute of Advanced Industrial Science and Technology (AIST), Ibaraki, Japan, 4Department of Mechanical Engineering, Tokyo Denki University, Tokyo, Japan, 5Department of Sport and Health Sciences, University of Ease Asia, Yamaguchi, Japan, 6Department of System Emotional Science, Toyama University, Toyama, Japan
Synopsis
We developed psoas major muscle (PM) MR elastography (MRE) technique and reported shear modulus of the PM for the first time in the world. However, measurement precision (repeatability and reproducibility) of this technique was not assessed. In this study, repeatability with three repetitions and reproducibility with different three operators were evaluated. Repeatability of this technique was about the same as required for clinical liver MRE and reproducibility was almost perfect. The original vibration pad was focused on generating shear wave in the PM efficiently. The development of the vibration pad specialized for PM MRE resulted in acceptable repeatability and reproducibility.
Introduction
According to the 2010 Global Burden of Disease Study, low back pain (LBP) is ranked highest in terms of years of living with a certain disability1. The specific causes for the 15% of LBP can be identified through diagnostic imaging or clinical examination (specific LBP). However, unfortunately, specific causes cannot be identified in about 85% of LBP cases (non-specific LBP). Ingber2 suggested that the increase of psoas major muscle (PM) stiffness due to myofascial dysfunction could be one of the causes for non-specific LBP. There are some methods for assessing tissue stiffness such as palpation and ultrasound elastography. However, these methods are seemed difficult to be applied to deep-lying tissues with a high degree of confidence. Magnetic resonance elastography (MRE) is a phase-contrast technique that allows measurement of the shear modulus of tissues, noninvasively and quantitatively even in deep lying tissues3,4. Thus, the PM MRE technique has been developed using a gradient-echo type multi-echo MRE sequence5,6.The Quantitative Imaging Biomarker Alliance (QIBA), which was organized by the Radiological Society of North America7 indicated that it is important to check precision of measurements for liver MRE. “Precision” means comparable data in repeated MRE examination in the same or similar conditions (same subject, same or different operator, same device, and same parameter).
Therefore, in the present study, measurement "precision" using "repeatability" with the same operator and "reproducibility" with different operators has been assessed.
Materials and Methods
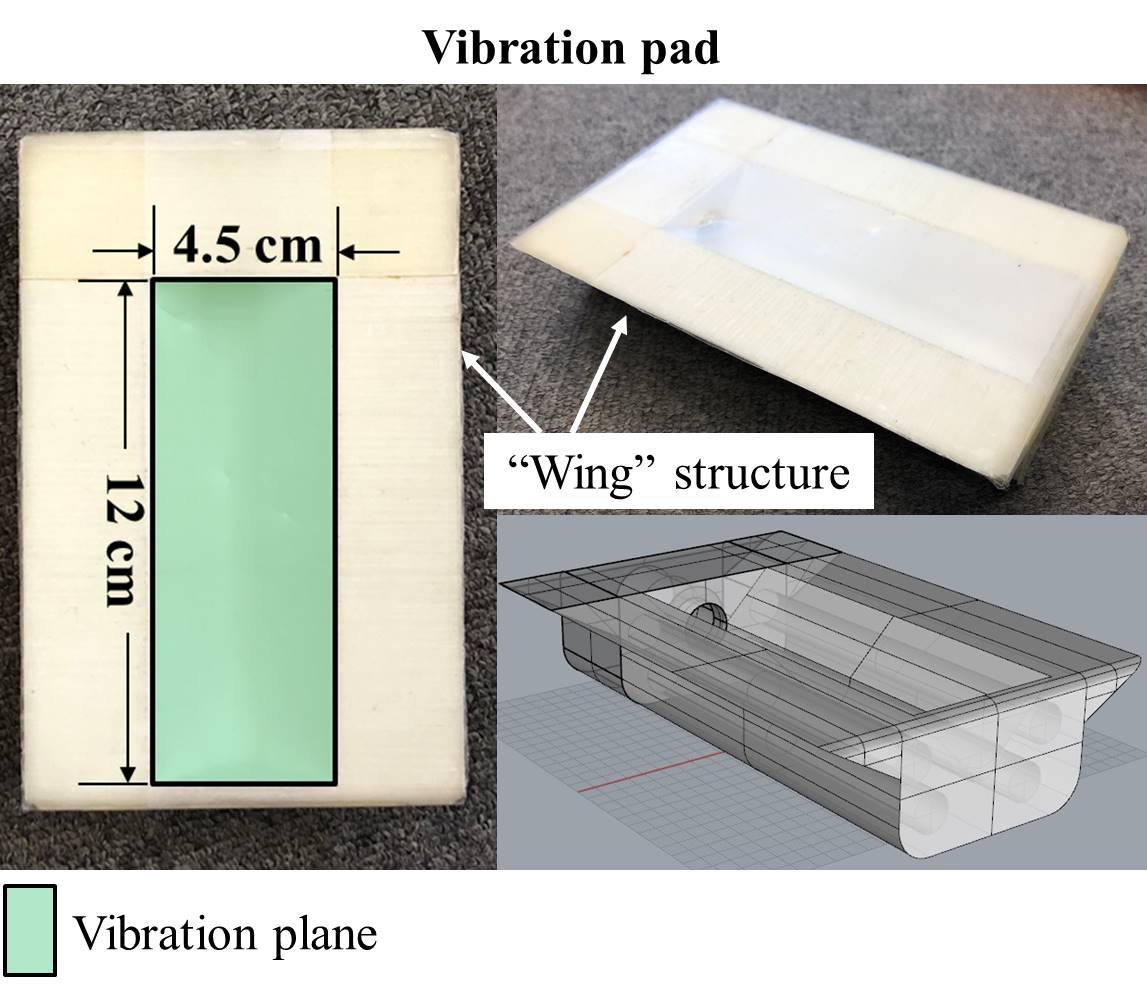
Volunteers with no history of specific LBP were enrolled in this MRE study. Nine volunteers participated in the repeatability study and three participated in the reproducibility study (all men, age range; 20-38).Pneumatic vibration pad for PM MRE (Fig.1) was made using a three-dimensional (3D) printer (3D touch, 3D Systems, Inc., Rock Hill, SC, USA). The setup of vibration pad was shown in Fig.2 and concrete pad position was shown in Fig.3. MRE experiments were performed on a clinical MR imager (Achieva 3.0T, Philips Healthcare, Best, The Netherlands) using a SENSE Torso coil (Philips Healthcare, Best, The Netherlands). An external vibration waveform was generated by a self-built waveform generation system (LabVIEW and USB-6221, National Instruments Corporation, Austin, TX, USA). MRE was performed with a gradient-echo type multi-echo MRE sequence. PM MRE was performed at 50 Hz vibration frequency. Acquisition parameters were as follows: 512×512 acquisition matrix, 50% scan percentage, two numbers of averages, 20° flip angle, 250-350 mm field of view, 10 mm slice thickness, 2.5 ms 1st TE, 12.5 ms 2nd TE, 40 ms TR, and 80 s total acquisition time (20 s for one scan, 4 vibration phase offsets). Imaging was performed in the oblique axial plane in which the oblique angle was parallel to the lumbar vertebral disc at the level of L3/L4.
Repeatability with three repetitions was evaluated by the repeatability coefficient expressed as percentage (%RC). Reproducibility with different three operators was evaluated by the interclass correlation coefficient (ICC). Concordance was evaluated as follows: poor if < 0, slight if it was between 0–0.20, fair if it was between 0.21–0.40, moderate if it was between 0.41–0.60, substantial if it was between 0.61–0.80, and almost perfect if it was between 0.81–1.
Results
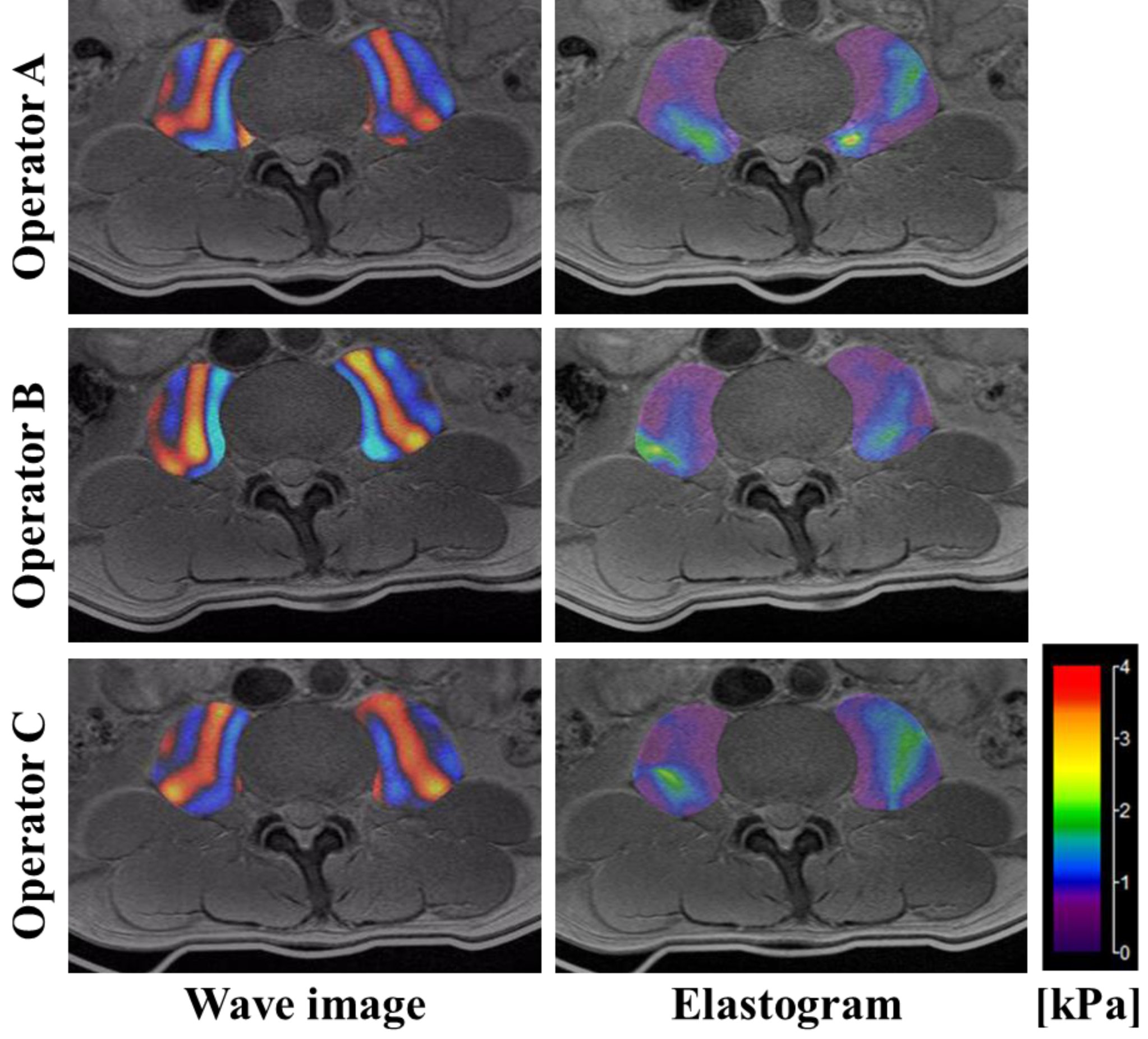
Fig.4 shows representative MRE images of the PM (three repetitions) in the repeatability study. The %RCs were 20.7% (95% confidence interval (CI): 3.27-23.0) in the right PM and 18.9% (95% CI: 2.98-21.0) in the left PM, respectively. QIBA consensus profile required the %RC in the liver MRE to be lower than 19%. It was found that %RC of PM MRE technique was comparable to that required for liver MRE, which was about 19%, suggesting that the PM MRE technique used in this study had the repeatability same as the liver MRE.Fig.5 shows representative MRE images of the PM performed by three different operators in the reproducibility study. ICCs were 0.93 (95% CI: 0.46-0.99) in the right PM and 0.97 (95% CI: 0.76-0.99) in the left PM, which showed almost perfect reproducibility.
Discussion
The development of the vibration pad suitable for PM MRE resulted in good repeatability and reproducibility. The vibration pad was focused on vibrating lumber vertebra (vibration plane) and to perform PM MRE in supine position (“wing” structure). Numano et al.6 reported that an efficient method to propagate the shear wave to the PM was to vibrate the lumbar spine. Fig.4 and Fig.5 showed symmetric wave propagation from the lumber spine with good repeatability and reproducibility. MRE was generally more dependent on the operator's skills than conventional imaging techniques, such as MRI or CT, because the results of MRE varied depending on the location or fixation strength of the vibration pad. In the present study, the vibration pad was fixed by the subject’s own weight in a supine position, and it was not dependent on operators' skills. It seemed that the vibration pad pushed deeply into the volunteer's lower back, however, “wing” structure of the vibration pad (Fig.1) reduced pain and permit subjects to perform PM MRE in supine position.Conclusion
Our PM MRE technique had repeatability same as required for the liver MRE and had almost perfect reproducibility. The original vibration pad seemed to suitable for performing PM MRE with acceptable repeatability and reproducibility.Acknowledgements
This work was supported by JSPS KAKENHI Grant NumberJP19K09579, Japan.References
1. Hoy D, March L, Brooks P, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis 2014;73(6):968-74.
2. Ingber RS. Iliopsoas myofascial dysfunction: a treatable cause of "failed" low back syndrome. Arch Phys Med Rehabil 1989;70(5):382-6.
3. Muthupillai R, Lomas DJ, Rossman PJ, et al. Magnetic resonance elastography by direct visualization of propagating acoustic strain waves. Science (New York, NY) 1995;269(5232):1854-7.
4. Muthupillai R, Ehman RL. Magnetic resonance elastography. Nature Medicine 1996;2(5):601-3.
5. Numano T, Mizuhara K, Hata J, et al. A simple method for MR elastography: a gradient-echo type multi-echo sequence. Magn Reson Imaging 2015;33(1):31-7.
6. Numano T, Habe T, Ito D, et al. A new technique for motion encoding gradient-less MR elastography of the psoas major muscle: A gradient-echo type multi-echo sequence. Magn Reson Imaging 2019;63:85-92 .
7. MR Elastography Biomarker Committee. Magnetic Resonance Elastography of the Liver, Quantitative Imaging Biomarker Alliance. Profile Stage: Consensus. QIBA, August 20, 2019. Available from: https://qibawiki.rsna.org/index.php/Profiles
Figures