3335
Tomoelastography for Quantification of Heterogeneity in Primary Sclerosing Cholangitis-related Hepatic Fibrosis1Radiology, Charité - Universitätsmedizin Berlin, Berlin, Germany, 2Bioengineering, University of Illinois at Chicago, Chicago, IL, United States, 3Hepatology, Charité - Universitätsmedizin Berlin, Berlin, Germany, 4Medical Informatics, Charité - Universitätsmedizin Berlin, Berlin, Germany
Synopsis
Primary sclerosing cholangitis (PSC) is a rare chronic liver disease that leads to stricturing of bile ducts and a heterogeneous distribution of hepatic fibrosis. Despite the success of MR cholangiopancreaticogram and liver biopsy for the detection of PSC, they do not correlate with the severity of disease. Currently, there is no accurate diagnostic reference standard for monitoring the disease activity in PSC which limits patient management. Tomoelastography has the potential to quantify heterogeneity in PSC-related hepatic fibrosis using a normalized standard deviation index as a new biomarker besides overall stiffness.
Introduction
Primary sclerosing cholangitis (PSC) is a rare chronic liver disease that leads to stricturing of intra- and extrahepatic bile ducts, hepatic tissue damage and a heterogeneous distribution of fibrosis.1,2 In contrast, other chronic liver diseases such as viral hepatitis show a homogeneous distribution of fibrosis. Although MR cholangiopancreaticogram (MRCP) and liver biopsy are successful in the detection of PSC, they do not correlate with the severity of disease.1,3 Currently, there is no accurate diagnostic reference standard for monitoring the disease activity in PSC. The aim of this study was to quantify the heterogeneity of PSC-related fibrosis as a potential new biomarker in comparison to viral hepatitis as a control group using tomoelastography.Methods
Forty-six subjects were prospectively enrolled in this monocenter study: 20 patients with PSC (mean age of 41 ± 14 years, 5 female subjects) and 26 patients with viral hepatitis (mean age of 50 ± 14 years, 8 female subjects). The study was approved by the institutional review board, and written informed consent was obtained from all subjects. Tomoelastography by multifrequency MR elastography was performed at 1.5 Tesla (Magnetom Aera, Siemens Healthineers, Erlangen, Germany) using a custom-designed piezoelectric driver, six mechanical drive frequencies from 35 to 60 Hz with 5 Hz increments, and compound multifrequency processing.4 Shear wave speed (SWS, in m/s) was measured as a surrogate of stiffness. Inclusion criteria were biliary stricturing on MRCP or typical histopathological features on biopsy for PSC, blood testing for viral hepatitis, and age ≥ 18 years.5 Exclusion criteria were acute cholangitis, history of other liver diseases, and malignancies. Fibrosis staging was based on SWS cut-off values as follows: F1, 1.52 m/s; F2, 1.55 m/s; F3, 1.67 m/s; F4, 1.72 m/s.6 A normalized standard deviation index (NSDI) was introduced for quantifying fibrosis heterogeneity, which accounts for differences in fibrosis severity. Groups were compared using a two-sided t-test with a level of significance of P ≤ 0.05.Results
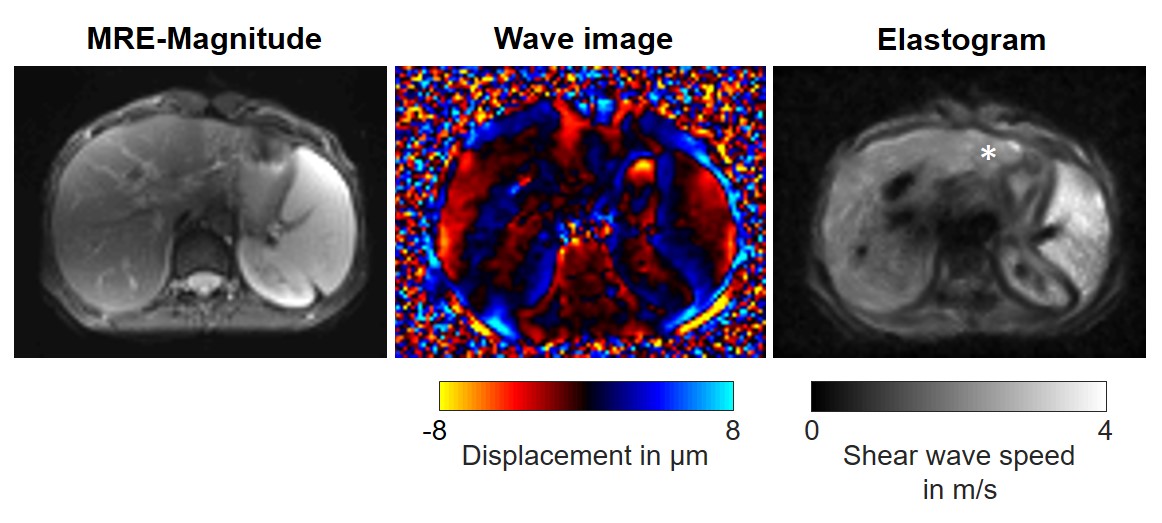
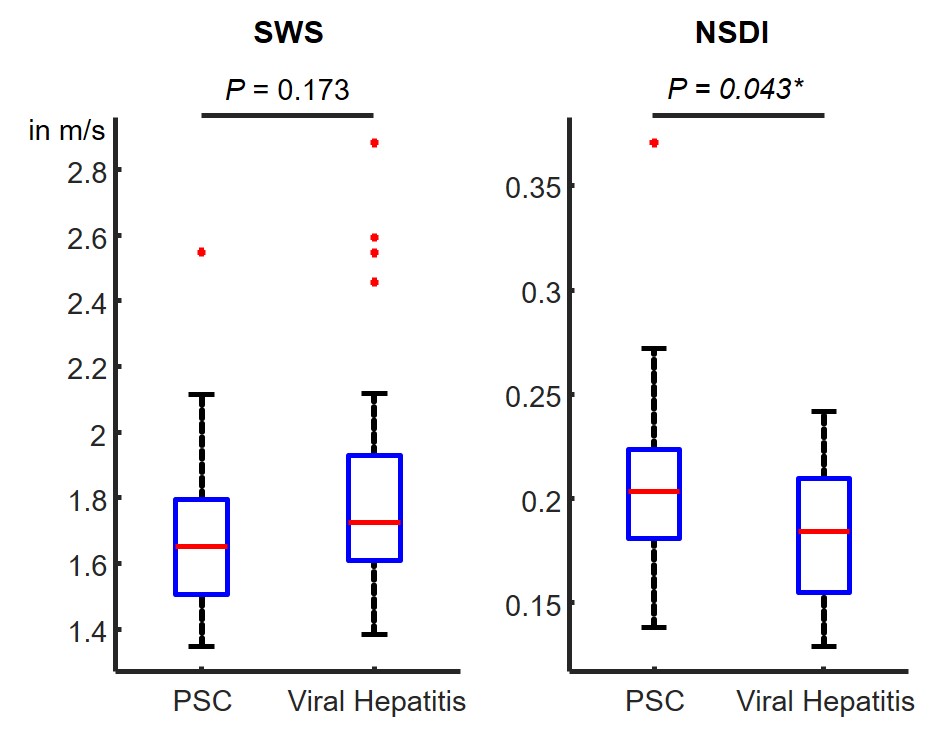
Figure 1 shows an exemplary case of a PSC patient with pronounced fibrosis in the left liver lobe. The following distribution of fibrosis stages were found based on tomoelastography for PSC: F0, n = 6; F1, n = 2; F2, n = 2; F3, n = 1; and F4, n = 9; and for viral hepatitis: F0, n = 4; F1, n = 2; F2, n = 4; F3, n = 3; and F4, n = 13. Mean group values of SWS and NSDI for all fibrosis stages combined were 1.70 m/s (0.21) for PSC and 1.84 m/s (0.18) for viral hepatitis. A statistically significant increase of NSDI in PSC (P = 0.043) was evident as shown in figure 2. No significant difference was found for SWS (P = 0.173) and SD without normalization (PSC, 0.36 m/s and viral hepatitis, 0.35 m/s; P = 0.655).Discussion and Conclusion
This preliminary study is a first step towards relating fibrosis heterogeneity to the severity of PSC. It is a stimulating result that a significant increased fibrosis heterogeneity – quantified through NSDI – was evident in the PSC group. These results encourage further investigation of the quantification of heterogeneity as a potential new biomarker besides overall stiffness for the assessment of PSC-related hepatic fibrosis.Acknowledgements
Funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation): RE 4161/1-1 (Rolf Reiter), RE 4161/1-2 (Rolf Reiter), RE 4161/2-1 (Rolf Reiter); Project Number 372486779 - SFB 1340 Matrix-in-Vision (Christian Bayerl, Bernd Hamm, Jürgen Braun, Ingolf Sack and Patrick Asbach)
References
1. Burak KW, Angulo P, Lindor KD, et al. Is there a role for liver biopsy in primary sclerosing cholangitis? Am J Gastroenterol. 2003:98(5);1155–1158.
2. Zenouzi Z, Welle C, Venkatesh S, et al. Magnetic Resonance Imaging in Primary Sclerosing Cholangitis—Current State and Future Directions. Semin Liver Dis. 2019;39(3):369-380.
3. Bader TR, Beavers KL, Semelka RC. MR Imaging Features of Primary Sclerosing Cholangitis: Patterns of Cirrhosis in Relationship to Clinical Severity of Disease. Radiology. 2003;226(3):675-685.
4. Tzschätzsch H, Guo J, Dittmann F, et al. Tomoelastography by multifrequency wave number recovery from time-harmonic propagating shear waves. Med Image Anal. 2016;30(5):1-10.
5. Eaton JE, Talwalkar JA, Lazaridis KN, et al. Pathogenesis of Primary Sclerosing Cholangitis and Advances in Diagnosis and Management. Gastroenterology. 2013;145(3):521-536.
6. Reiter R, Tzschätzsch H, Dittmann F, et al. Diagnostic Performance of Tomoelastography by Multifrequency Magnetic Resonance Elastography for Staging Hepatic Fibrosis. In Proceedings of the 104th Scientific Assembly and Annual Meeting of the Radiological Society of North America 2018;SSC06-02.
Figures