3306
Implementation of Liver MR Elastography Tutorial Module to Improve Exam Quality and Reduce Patient Callback Rate1Radiology, Mayo Clinic Arizona, PHOENIX, AZ, United States
Synopsis
In this age of specialized imaging sequences such as liver MR elastography, inexperience with the technical image acquisition and unawareness of artifacts and pitfalls confound diagnostic accuracy due to poor image quality. We feel there is a knowledge gap in those at the front line involved with image acquisition, and that by defining and filling in this knowledge gap with an educational tutorial module, MR elastography image quality can be optimized and callback rates can be decreased. In turn, decreased callbacks will translate into reduced cost for unnecessary repeated scans; reduced patient time and frustration; and increased MR scheduling access.
Introduction
Liver magnetic resonance elastography (MRE) is a highly useful adjunct tool for the evaluation of liver pathology and fibrosis1-4. In order for the radiologist to render an accurate diagnosis, the overall quality of a study must be diagnostic. At our institution, a radiologist may request a patient call back if they believe the study is not diagnostic at time of dictation. We previously evaluated our body MR callback cases over a 9 year period (2010-2018) and discovered 154 body MR callbacks of 44811 total body MR cases performed. Of these, 22 (of 154) of the callbacks were secondary to technical issues with the MRE acquisition. We identified the key checkpoints of the MRE acquisition process to be the MR technologists and their interaction with the patient, as well the readers of the MR elastography studies. We believed there was a knowledge gap in understanding how to troubleshoot the MRE exam, and therefore designed a self-paced quality control tutorial that was distributed to those involved in MRE image acquisition and interpretation. With the implementation of the tutorial, we believe there will be an overall improvement in image quality and decrease in number of MRE callbacks.Methods
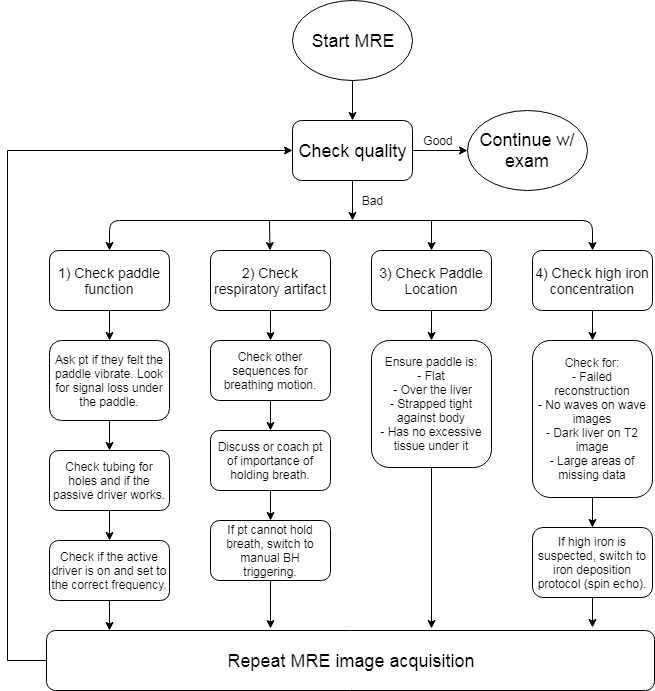
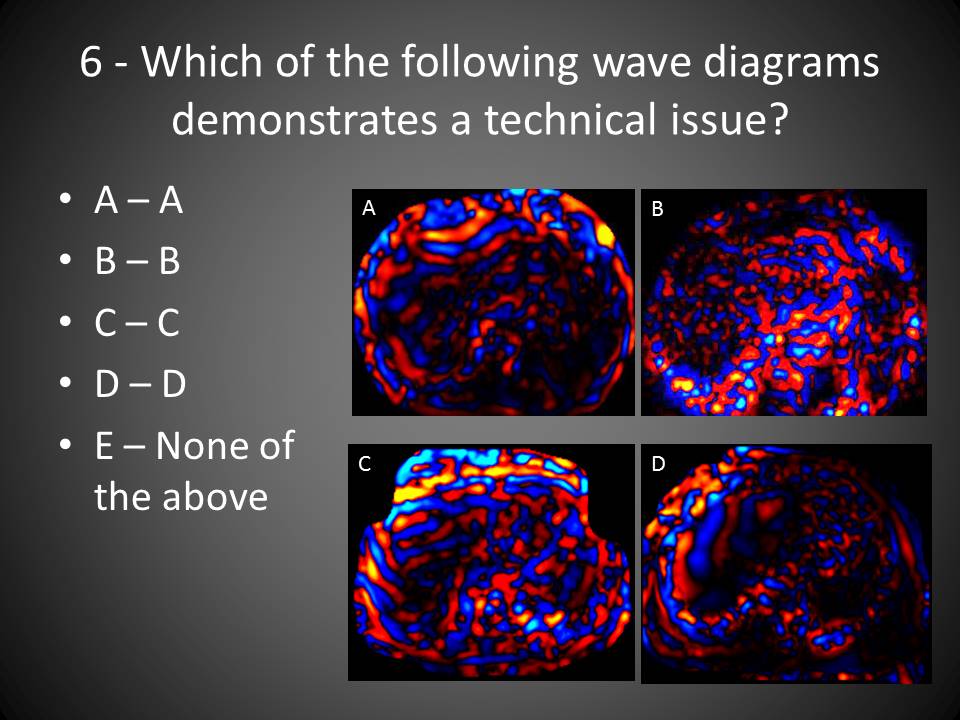
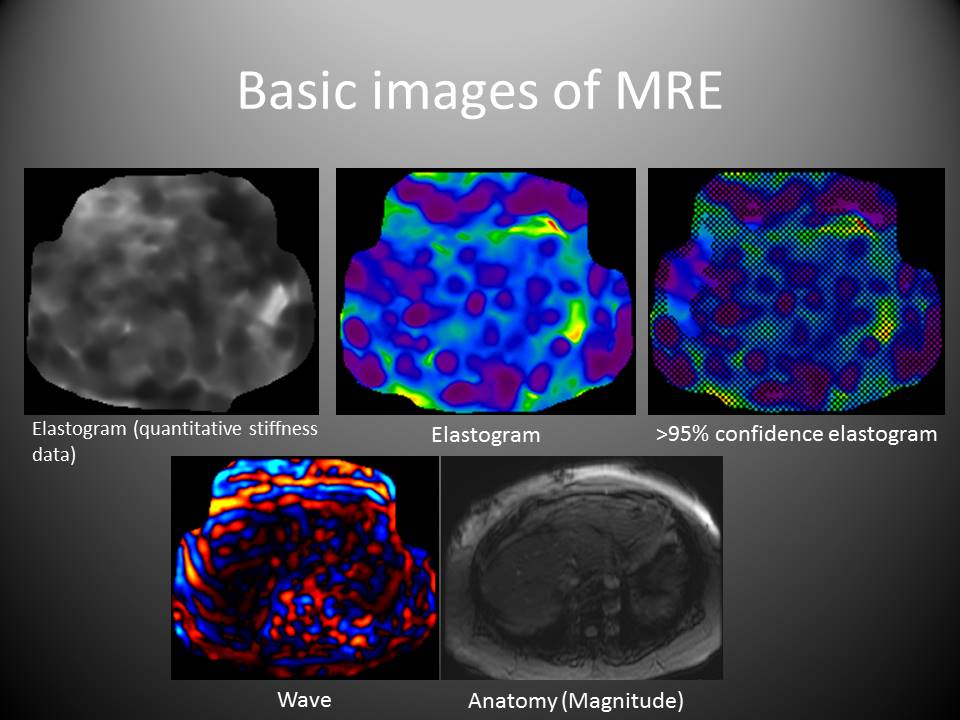
We created an educational packet that included the basics of MR elastography, common artifacts, and a decision-tree algorithm to troubleshoot and resolve poor image quality (Figure 1). Our test group included all MR technologists and MR abdomen readers including faculty, fellows, and residents. After completing an initial 21 question pretest, the group was given 2 weeks to learn from a self-paced tutorial module on the basics of MR elastography (Figures 2 and 3). This was followed by a 21 question posttest. We had a total of 18 participants who completed the study in March 2019. The number of MRE callbacks April 2019 to the present was compared to historical values.Results
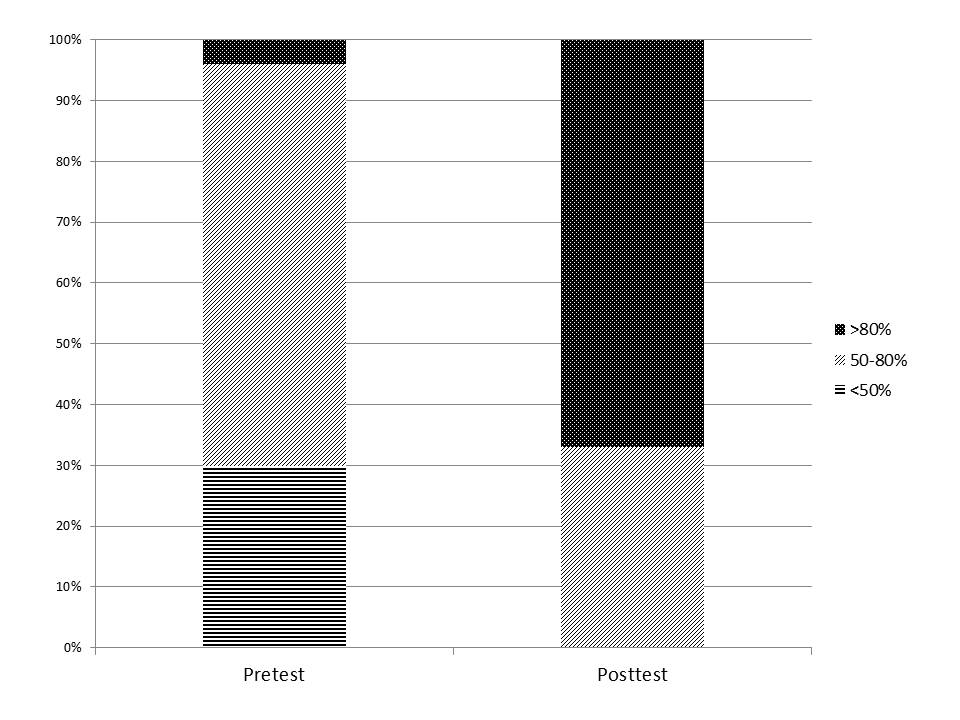
Prior to the aforementioned intervention, the baseline MR elastography callback rate was 22 (of 1734 total MRE studies performed) for 2010-2018. In the 18 participants, 30% scored <50% correct; 66% scored 50-80%; and 4% scored >80% on the pretest. Following administration of the liver MR elastography quality control learning module, the study group scores increased with 0% scoring <50% correct; 33% scoring 50-80%; and 67% scoring >80% (Figure 4). Scores improved by a mean of 21 points (standard deviation (SD) of 17, 95% confidence interval of 13 to 29, p<0.0001 by two-tailed paired t-test) from a baseline mean of 63 points (SD 13) to a post-intervention mean of 84 points (SD 14). Post intervention, the MR elastography callback rate was 0 (of 208 total MRE studies performed) from April-July 2019.Discussion
With introduction of a self-paced Liver MR elastography quality control learning module, we were able to increase the study group’s basic knowledge in troubleshooting MRE image quality as evidenced by improved posttest scores. This has translated to a decrease in the MR elastography callback rate since the intervention from 14% to 0%. Furthermore, patient throughput has been improved as we have defined specific steps for identifying and resolving poor image quality, with resultant decrease in the number of unnecessary repeated series. We understand that only a short time has passed since intervention and the overall callback rate can be affected by personnel change, but the results are promising that our liver elastography tutorial module can optimize MRE image quality/acquisition, with resultant decrease in frequency of patient callbacks.Conclusion
Familiarity and understanding of optimal MRE acquisition options as well as recognition of MRE artifacts and pitfalls via incorporation of a quality control learning module can help optimize MRE exams and decrease unnecessary patient callbacks.Acknowledgements
Lead MR technologists - Vicki Place, Cathy Gustafson
Radiology manager - Chris Tollefson
Statistics - Joseph G. Hentz
References
1. Hoodeshenas, S., Yin, M., & Venkatesh, S. K. (2018). Magnetic Resonance Elastography of Liver. Topics in Magnetic Resonance Imaging, 27(5), 319–333.
2. Batheja M, Vargas H, Silva AM, Walker F, Chang YH, De Petris G, Silva AC. Magnetic resonance elastography (MRE) in assessing hepatic fibrosis: performance in a cohort of patients with histological data. Abdom Imaging. 2015 40(4):760-5.
3. Gallegos-Orozco JF, Silva AC, Batheja MJ, Chang YH, Hansen KL, Lam-Himlin D, De Petris G, Aqel BA, Byrne TJ, Carey EJ, Douglas DD, Mulligan DC, Silva AM, Rakela J, Vargas HE. (2015). Magnetic resonance elastography can discriminate normal vs. abnormal liver biopsy in candidates for live liver donation. Abdom Imaging. 40(4):795-802.
4. Venkatesh, S. K., Yin, M., & Ehman, R. L. (2013). Magnetic resonance elastography of liver: Technique, analysis, and clinical applications. Journal of Magnetic Resonance Imaging, 37(3).
Figures