3207
Simultaneous T1-weighted imaging, R2* mapping, and QSM from a multi-echo MPRAGE sequence using a radial fan-beam sampling scheme at 3 Tesla1University of Queensland, Brisbane, Australia, 2University of Calgary, Calgary, AB, Canada, 3General Electric Healthcare, Calgary, AB, Canada
Synopsis
A multi-echo MPRAGE sequence with radial fan-beam segments is demonstrated at 3 T. The radial fan-beam sampling scheme permits any number of encoding steps by adjusting the fan size for each inversion segment, which allows longer echo time for magnetic susceptibility contrast. Simultaneous T1-weighted image, R2* map, and QSM were successfully extracted from the single acquisition and were compared with images reconstructed from standard single-echo MPRAGE and multi-echo GRE acquisitions.
Introduction
Recent papers have demonstrated the derivation of T1-weighted, T1 map, R2* map, SWI, and QSM simultaneously from the multi-echo version of MP2RAGE sequence at 7 T [1,2,3]. We aimed to implement this using an MPRAGE sequence, which is widely available and routinely acquired, at the clinical field strength of 3 T. For robust QSM at 3 T the TE needs to be at least 15 ms, as adopted in most QSM studies. However, this long TE makes it challenging to accommodate all the slice encoding steps in a single MPRAGE inversion segment. In this study, we use a radial fan-beam sampling scheme, as proposed in a previous study [4], which permits any number of encoding steps by adjusting the fan size for each inversion segment. This work demonstrates the feasibility of simultaneous T1-weighted imaging, R2* mapping, and QSM using this sequence at 3 T.Methods
Multi-echo MPRAGE with radial fan-beam (RFB) samplingA conventional single-echo MPRAGE sequence was extended into a multi-echo version to enable longer TEs for R2* mapping and QSM. As demonstrated in Figure 1a, each slice encoding step (‘view’) acquired 4 bipolar echoes. Instead of traversing all slice encoding lines for a single inversion step, we segment the ky-kz sampling trajectory into multiple RFBs, as shown on the right. Each RFB sampling starts with an inversion pulse and begins from the center of k-space. In this way, we can control the size of the fan to set the number of views and thus maximum TE for each fixed sequence TR, according to TRseq = TEmax*Nviews.
In vivo experiments at 3 T
Five healthy subjects (22 to 36 years, 4-M,1-F) were scanned using three sequences: (i) sagittal MPRAGE (256*256*192 matrix, 1 mm3, 2.9 ms TE, 650 ms TI, R=2 GRAPPA, 5 mins), (ii) axial multi-echo GRE (256*256*128 matrix, 1 mm3, 8 echoes, 3.4 ms first TE, 3.5 ms echo spacing, 29.8 ms TR, R=2 SENSE, 6 mins), (iii) sagittal multi-echo MPRAGE with RFB (256*256*192 matrix, 1 mm3, 1000 ms TI, 2250 ms sequence TR, 2.7/7.1/11.5/15.9 ms TEs, 70 views per RFB segment, R=2*2 GRAPPA, 8 mins). For one subject, another two ME-MPRAGE RFB scans were acquired in axial FOVs (match ME-GRE coverage), with 4 TEs (longest 15.9 ms) and 6 TEs (longest TE 24.6 ms). Acquisition time for these two axial scans was long (10 and 13 mins) due to a lack of two-dimensional accelerations in the 12 channel receiver head coil used.
T1-weighted, R2* and QSM reconstruction
Magnitude and phase images from multiple echoes were produced from the sequence, as shown in Figure 1b. Phase images were unwrapped and fitted with echo times to generate a total field map. The background field was removed using the RESHARP method and susceptibility inversion was performed using the iLSQR method. R2* mapping was carried out using a mono-exponential fit. Magnitude images withT1-weighted contrast from individual echoes were combined using sum-of-squares to increase SNR.
Results
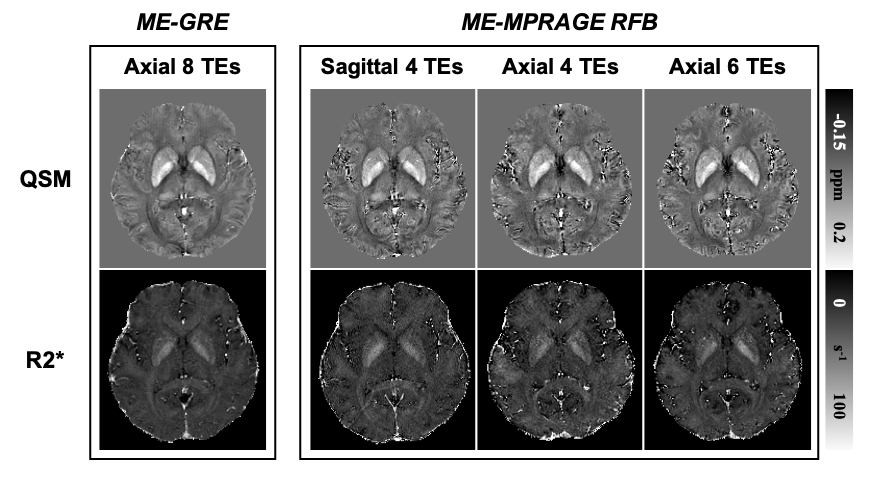
Figure 2 shows T1-weighted, R2*, and QSM results of a healthy subject reconstructed from the sagittal ME-MPRAGE RFB sequence. T1-weighted images showed excellent contrasts between white matter, grey matter, and CSF, while R2* and particularly QSM showed high signal intensities in iron-rich deep grey matter regions.R2* and QSM from the proposed ME-MPRAGE RFB sequence with different parameters (i.e., sagittal vs. axial FOV and 16 ms vs. 25 ms TE) are compared with those from a standard multi-echo GRE sequence (axial and 30 ms TE) in Figure 3. Overall, these quantitative maps appeared similar among these different sequences and acquisition parameters. CSF appeared noisy in all ME-MPRAGE RFB results, due to the suppressed signal intensity in the T1-weighted magnitude images and low SNR in the phase measurements.
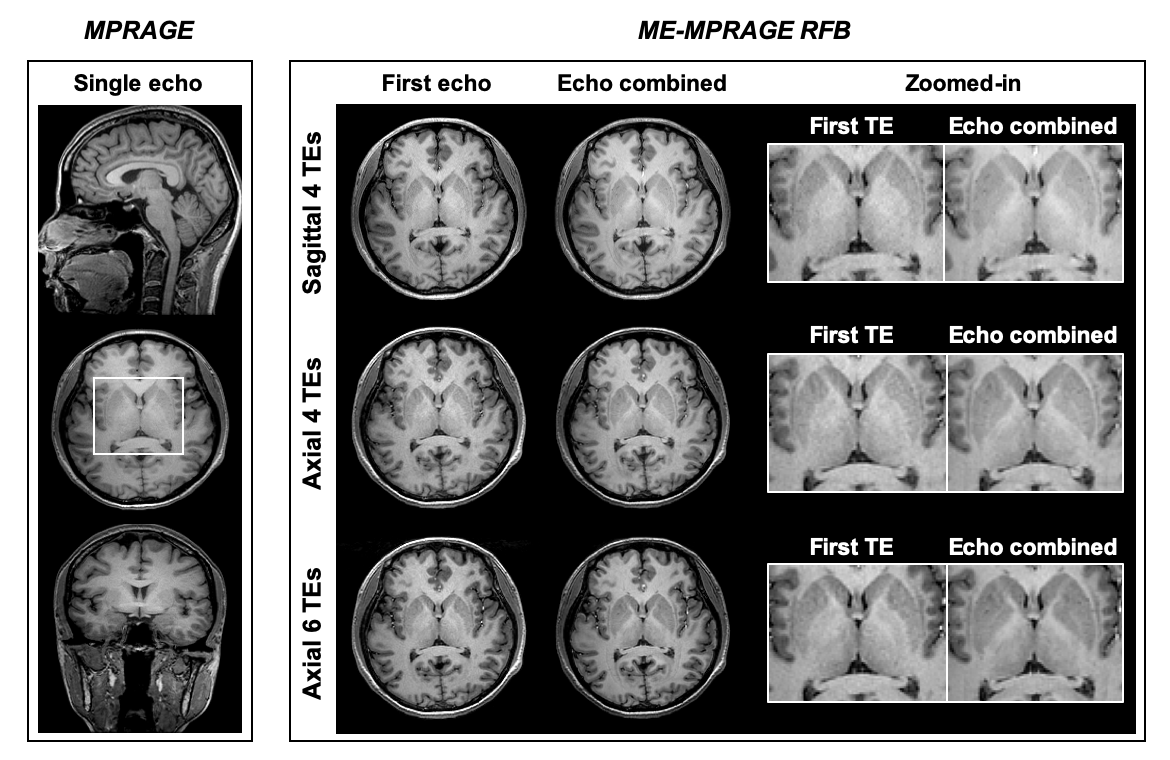
T1-weighted images from ME-MPRAGE RFB are compared with the regular single-echo MPRAGE in Figure 4. Echo combined T1-weighted images showed improved SNR over the first echo. Also, basal ganglia and thalamus gained T2* contrast in the echo combined images due to more T2* weighting from the longer TEs.
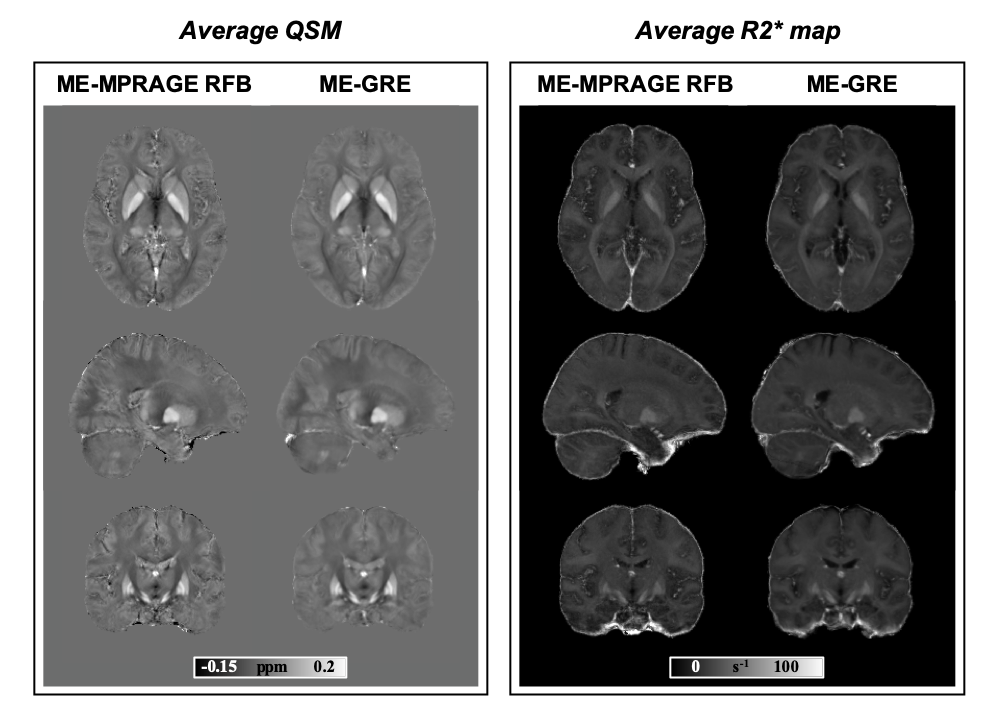
Group average maps of QSM and R2* from the 5 subjects are compared between ME-MPRAGE RFB and ME-GRE in Figure 5. All images were registered to the MNI template using ANTs software. Images from both sequences appear very similar, showing excellent deep grey matter, white matter, and cortical grey matter contrast. CSF was noticeably noisier in ME-MPRAGE RFB than ME-GRE. Preliminary analysis of deep grey matter QSM and R2* measurements from the 5 subjects found no significant difference between the two sequences.
Discussion
The proposed sagittal ME-MPRAGE RFB sequence takes 8 mins, which saves about 25% scan time over individual MPRAGE (5 mins) and ME-GRE (6 mins) combined. Future work will test a 32-channel head coil with 2*2 GRAPPA acceleration in the axial acquisition with a smaller FOV coverage, which should reduce the scan time to 5-6 mins. CSF phase signal is unreliable due to low SNR, and future work will investigate the benefit of masking out CSF for QSM reconstruction from the ME-MPRAGE RFB sequence.Conclusion
A multi-echo MPRAGE with radial fan-beam segments is demonstrated at 3 T. Simultaneous T1-weighted image, R2* map, and QSM were successfully extracted from the single acquisition.Acknowledgements
No acknowledgement found.References
[1] Metere R, Kober T, Möller HE, Schäfer A. Simultaneous Quantitative MRI Mapping of T1, T2* and Magnetic Susceptibility with Multi-Echo MP2RAGE. PLoS One. 2017.
[2] Caan MWA, Bazin PL, Marques JP, de Hollander G, Dumoulin SO, van der Zwaag W. MP2RAGEME: T1, T2*, and QSM mapping in one sequence at 7 tesla. Hum Brain Mapp. 2019.
[3] Sun H, Cleary JO, Glarin R, Kolbe SC, Ordidge RJ, Moffat BA, Pike GB. Extracting more for less: multi-echo MP2RAGE for simultaneous T1-weighted imaging, T1 mapping, R2* mapping, SWI, and QSM from a single acquisition. Magn Reson Med. 2019.
[4] Saranathan M, Tourdias T, Bayram E, Ghanouni P, Rutt BK. Optimization of white-matter-nulled magnetization prepared rapid gradient echo MP-RAGE imaging. Magn Reson Med. 2015.
Figures