3074
Comparing PET/MRI with PET/CT in detection of lung nodules 4mm or larger using a single-breath hold MR acquisition1Diagnostic radiology, University of Wisconsin School of Medicine and Public health, Madison, WI, United States, 2Medical physics, University of Wisconsin School of Medicine and Public health, Madison, WI, United States
Synopsis
One of the limitations of PET/MRI is poor evaluation of lung parenchyma with free breathing sequences. In this study, 41 patients with gynecological malignancies underwent PET/MRI with rapid single breath hold lung acquisition after PET/CT. The CT and MRI of the lungs were reviewed blindly for detection of pulmonary nodules 4mm or larger. The study showed that there was no significant difference between the CT and single breath hold MRI using Chi square test. Improved detection of small pulmonary nodules using single breath hold sequence would increase the feasibility of stand-alone PET/MR imaging for clinical staging in oncologic patients.
Purpose
To investigate the utility of a single breath hold MR lung sequence using hybrid PET/MRI system to detect lung nodules >= 4mm compared to the free breathing CT portion of PET/CT in patients with gynecological malignancies.Background
Positron emission tomography/magnetic resonance imaging (PET/MRI) as a new hybrid imaging technology has promising applications in oncology.1 PET/MRI leverages the high soft tissue contrast and the functional sequences of MR with the molecular information of PET in single, hybrid imaging technology.2 To date, one of the limitations of PET/MRI is poor evaluation of the lung parenchyma with free breathing sequences.3 Pulmonary imaging with MRI has been limited by the low proton density, rapid signal decay, substantial respiratory and cardiac motion present in lung tissue. The MR imaging detection rate of large pulmonary nodules more than 1 cm is high; however, the detection rate of sub centimeter nodules remains inadequate on routine clinical sequences.3,4Methodology
This retrospective, HIPAA-compliant study was approved by our institutional human subjects review committee. 41 patients with gynecological malignancies underwent rapid, single breath hold MRI imaging of the lungs with short TE in a hybrid PET/MR imaging unit (Signa PET/MR, GE Healthcare) as a part of clinical whole-body PET/MRI immediately after clinical PET/CT. Patients received a dedicated clinical PET/MR examination of the pelvis, for which Gadolinium contrast was administered. Lung imaging occurred approximately 5 minutes after contrast administration. MR sequence parameters included: type=3D gradient echo; FOV = 46 x 46 x 36.4 cm; resolution: 1.4 x 1.6 x 2.6 mm (reconstructed at 1.4 x 1.6 x 1.3 mm); TE = 1 ms; TR = 3.1 ms; flip angle = 4-5 degrees; acceleration = 2 x 2 (phase x slice); scan time = 24 s. Directly identifiable information (e.g. name, MRN, etc.) have been removed. The CT and MRI imaging of the lungs were reviewed blindly by a nuclear radiologist for detection of pulmonary nodules measuring >= 4mm. Statistical significance between CT and MRI exams was compared using Chi square test.Results
A total of 41 patients were included. The total number of pulmonary nodules >= 4mm identified with CT part of PET/CT was 16. The total number of pulmonary nodules >= 4mm identified with breath hold MRI lung sequence of PET/MRI was 13. CT detected nodules in 5 patients and missed one patient. For MRI, nodules were also detected in 5 patients and missed in one patient. Chi square analysis showed prob > chi2 = 1.0000, with p-value 0.999. This suggests that there is no statistical differences between the two modalities for nodules >=4mm.Discussion
In patients with gynecological malignancies, whole body PET/MRI with diagnostic pelvic sequences has superior tissue contrast making it excellent for local staging. Adding the strengths of PET in staging nodal and distant metastatic disease to the strengths of MRI in local staging may make the use of the hybrid PET/MRI powerful tool for comprehensive assessment of disease within a single examination. However, CT has been considered a better modality compared to MRI in evaluation of lung parenchyma including detection of pulmonary nodules. It is used for cancer staging either as a part of PET/CT or as high-resolution chest CT. Therefore, to assure accurate staging of lung metastatic disease, oncologic patients would undergo PET/CT in addition to the PET/MRI which exposes patients to more radiation from the CT and lengthens the time of the exam. Improved detection of small pulmonary nodules using a rapid single breath hold sequence would increase the feasibility of stand-alone PET/MR imaging for clinical staging and surveillance in gynecological malignancy without need for PET/CT. In this study, we have demonstrated that there is no significant difference between the CT and breath hold MRI in detection of lung nodules >=4mm. Incorporating rapid MR lung sequences in staging would shorten the imaging time and decrease the radiation exposure.Conclusion
PET/MRI with a rapid, single breath hold lung sequence has high reliability for detection of sub centimeter lung nodules that are large enough to be clinically significant.Acknowledgements
None.References
1. Drzezga A, Souvatzoglou M, Eiber M, et al. First Clinical Experience with Integrated Whole-Body PET/MR: Comparison to PET/CT in Patients with Oncologic Diagnoses. J Nucl Med. 2012;53:845–855.
2. Sasan Partovi, Andres Kohan, Christian Rubbert, et al. Clinical oncologic applications of PET/MRI: a new horizon. Am J Nucl Med Mol Imaging. 2014; 4(2): 202–212.
3. Quick HH, von Gall C, Zeilinger M, et al. Integrated whole-body PET/MR hybrid imaging: clinical experience. Invest Radiol 2013;48(5):280–289.
4. Burris NS, Johnson KM, Larson PE, et al. Detection of Small Pulmonary Nodules with Ultrashort Echo Time Sequences in Oncology Patients by Using a PET/MR System. Radiology. 2016 Jan;278(1):239-46.
5. Gibiino F, Sacolick L, Menini A, et al. Free-breathing, zero-TE MR lung imaging. MAGMA 2015;28(3):207–215.
6. Stolzmann P, Veit-Haibach P, Chuck N, et al. Detection rate, location, and size of pulmonary nodules in trimodality PET/CT-MR: comparison of low-dose CT and Dixon-based MR imaging. Invest Radiol 2013;48(5): 241–246.
7. Chandarana H, Heacock L, Rakheja R, et al. Pulmonary nodules in patients with primary malignancy: comparison of hybrid PET/MR and PET/CT imaging. Radiology 2013;268(3): 874–881.
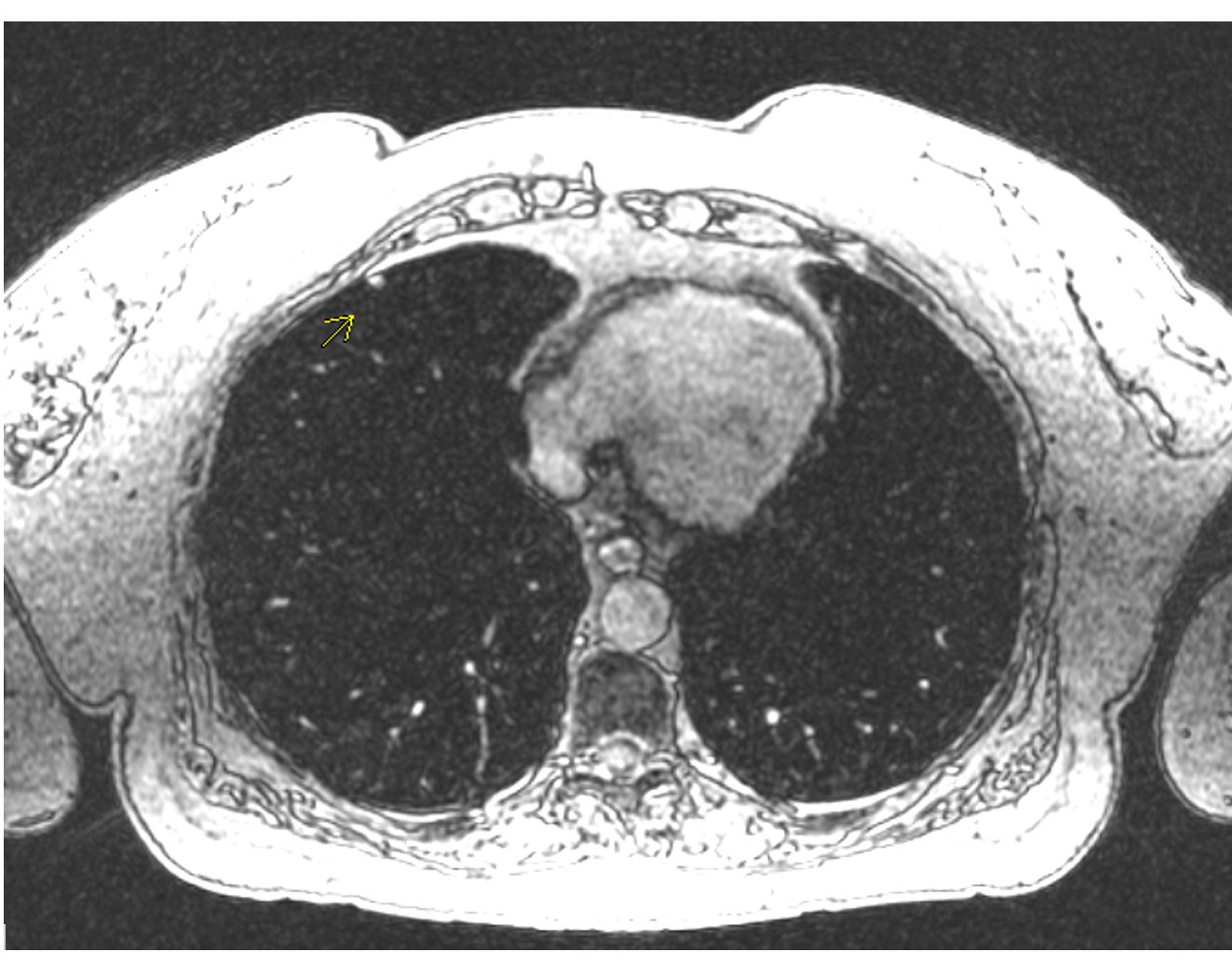
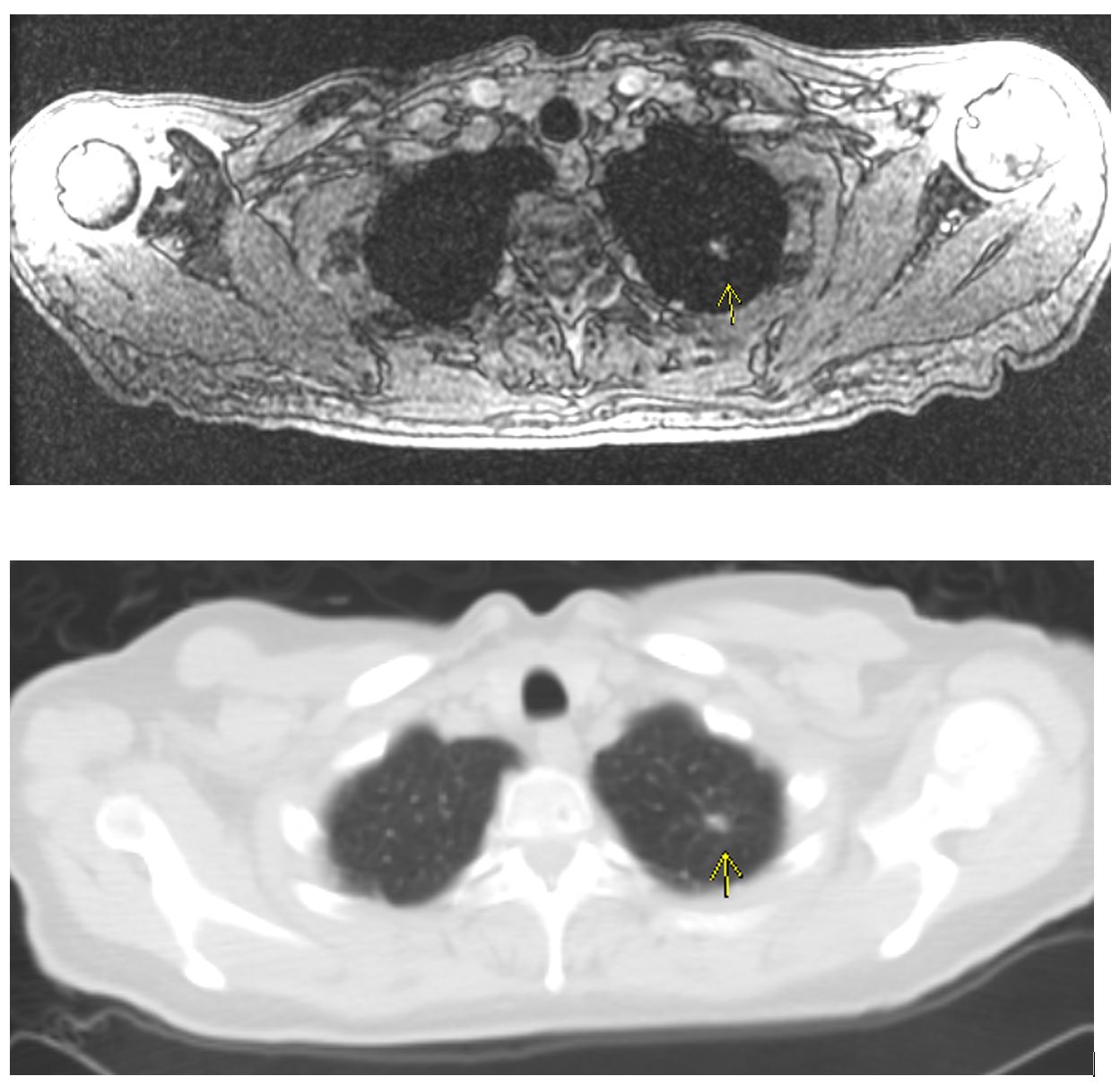
Figures