3061
Hybrid C11 Choline PET/MRI in staging untreated high risk and very high risk prostate cancer patients at single institution: preliminary results1Radiology, Mayo Clinic Arizona, PHOENIX, AZ, United States, 2Radiology, Mayo Clinic Arizona, Phoenix, AZ, United States, 3Urology, Mayo Clinic Arizona, PHOENIX, AZ, United States, 4Urology, Mayo Clinic Arizona, Phoenix, AZ, United States
Synopsis
The most prevalent malignancy in US men is prostate cancer. Appropriate treatment regimen is dependent on accurate tumor staging. Pelvic multiparametric MR (mpMRI) is the established modality for tumor and nodal staging. C-11 choline is FDA approved in diagnosis of recurrent prostate cancer. Introduction of a hybrid time-of-flight PET/MR system affords the opportunity to perform a combined C-11 choline PET + mpMRI for prostate cancer staging. We feel this system would be beneficial in staging of treatment naïve high risk prostate cancer.
Introduction
Prostate cancer is the most commonly diagnosed malignancy and the second most common cause of cancer related mortality in American men. Accurate diagnosis and staging is crucial for determining appropriate treatment regimens. Currently, pelvic multiparametric MRI (mpMRI) is the established imaging modality for lesion detection and nodal staging. C-11 Choline PET is under FDA approval in diagnosis of recurrent prostate cancer by targeting robust cell membrane synthesis in prostate cancer.1-4 Comparison of pelvic mpMRI and C-11 Choline PET has previously demonstrated the role for both in restaging of recurrence in prostatectomy patients. The opportunity to combine C-11 Choline PET with pelvic mpMRI in a single study has presented itself with the introduction hybrid time-of-flight PET/MR system. We believe hybrid prostate C-11 Choline PET/MR has an improved diagnostic and staging benefit in prostate cancer, particularly in high risk types.Methods
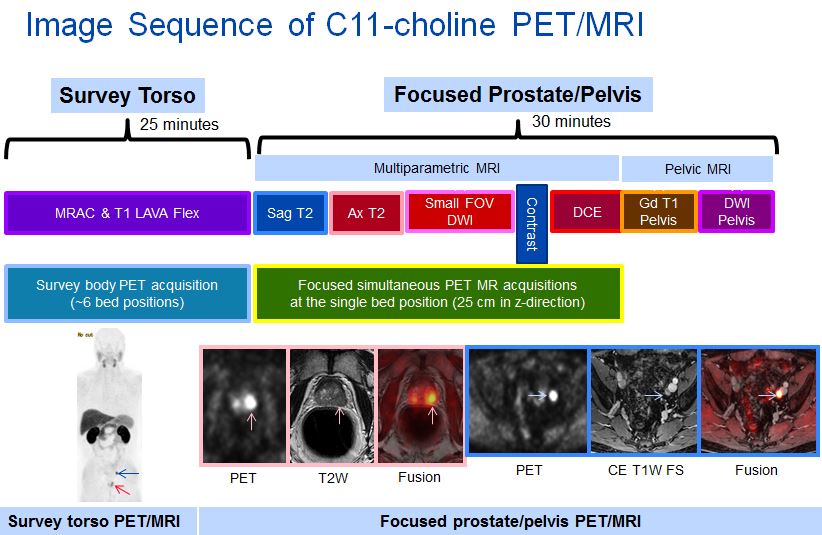
Twenty men diagnosed with prostate cancer, risk stratified as high risk or very high risk by National Comprehensive Cancer Network (NCCN) criteria were prospectively chosen to participate in this study. Exclusion criteria included any patient who had distant metastases, additional malignancies, or who did not achieve preoperative clearance. Eighteen patients have currently been recruited for this ongoing study. This HIPAA-compliant prospective study was approved by the Institutional Review Board (IRB). After informed consent was obtained, each patient underwent 7-bed position, pelvis-to-head torso PET/MR immediately after intravenous C-11 choline injection (12-14 mCi), followed by focused hybrid prostate mpMRI. The mpMRI protocol consists of large field-of-view T1 LAVA-FLEX pre- and post-contrast and diffusion weighted images (DWI), as well as high resolution sequences include T2 fast relaxation fast spin echo in all planes, DWI, and dynamic contrast enhanced sequences were obtained. Contemporaneous PSA level was documented. Uroradiologist review of the abdominopelvic CT and pelvis mpMRI with minimum 2 week memory extinction period. Dual-board certified nuclear radiologist review of the focused C-11 choline PET was performed. A consensus review of focused PET and MR with fusion images was also performed. The number of primary tumors and their maximal standard uptake value (SUVmax) were documented. Reviewer’s overall perceived confidence level for TNM staging was assessed. Surgical pathology from radical prostatectomy and pelvic lymph node dissection was considered as standard of reference. Tumor staging was compared amongst pelvic mpMRI, focused C-11 choline PET, and combined pelvic mpMRI and focused C-11 choline PET. TNM staging was compared to the surgical pathology staging. Evaluation of lymph nodes were evaluated by region and compared with CT, pelvic MRI, and combined pelvic mpMRI and focused C-11 choline PET. Evaluation of bone lesions was compared among bone scan, CT, MRI, and combined pelvic MRI and focused C-11 choline PET where available. Descriptive statistics were used.Results
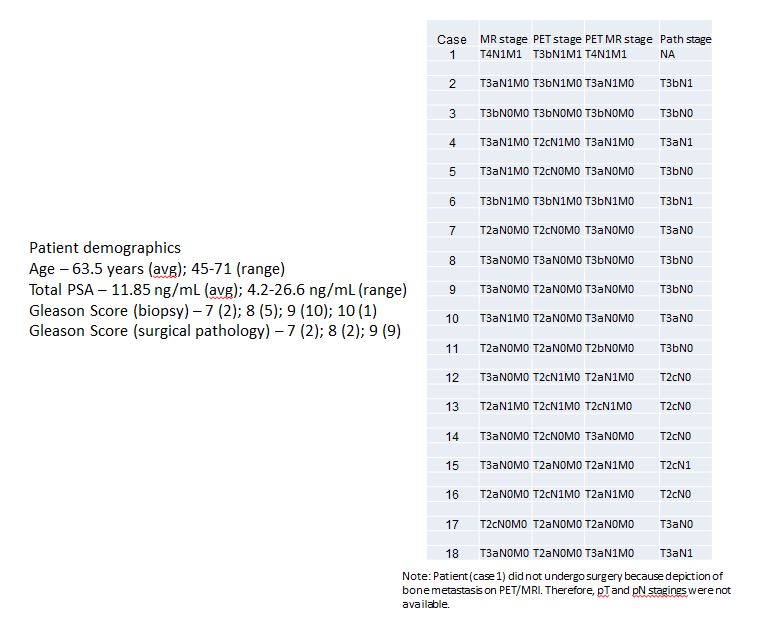
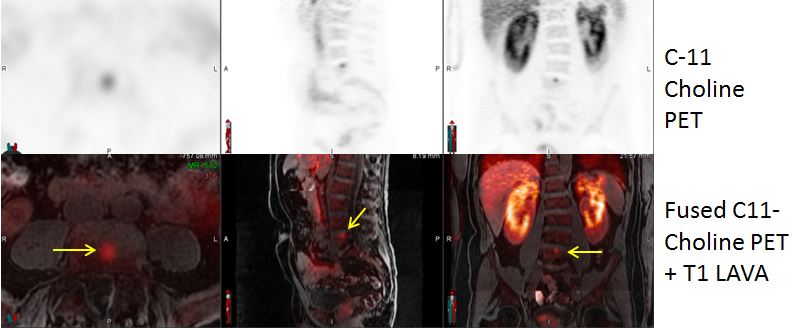
To date, 18 patients were enrolled and the patient’s characteristics were shown in Figure 1. Mean age was 63.5 years and ranged from 45-71 years. Total PSA averaged 11.85 ng/mL. Gleason score from biopsy was 7 in 2, 8 in 5, 9 in 10, and 10 in 1 patient. Gleason score from surgical pathology was 7 in 2, 8 in 2, and 9 in 9 patients. One of the 18 patients was shown to have unexpected bone metastasis at L5 on PET/MR with false negative bone scan and CT. Seventeen patients underwent surgery. TNM staging per modality was shown in Table 2. Bone marrow metastasis was present in one of 18 patients. The reviewers’ perceived confidence level was increased at the consensus review of MRI and focused PET/MRI when compared with each modality. Total of 22 prostate lesions were identified. Average SUVmax of the prostate lesions on the PET torso was 5.9 and 7.0 on the focused PET. Seventeen of the 18 patients had an increase in SUVmax (average 20%) from torso to focused PET. Total of 19 tracer avid nodal regions were identified. Average SUVmax of the tracer avid lymph nodes on the PET torso was 5.4 and 6.1 on the focused PET.Discussion
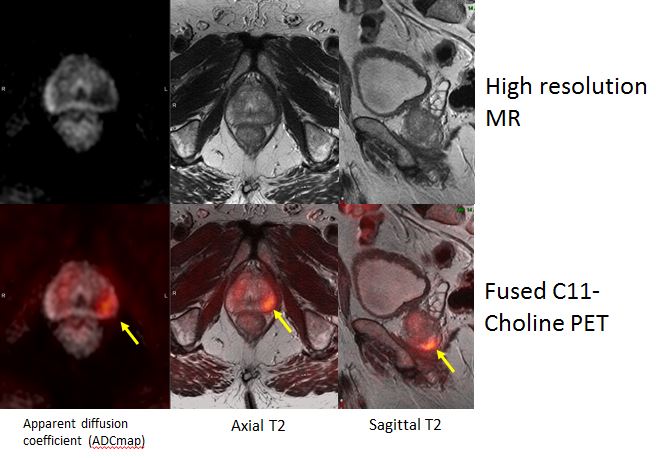
All lesions delineated on mpMRI which exhibited increased C-11 Choline uptake were confirmed as malignant on surgical pathology. Supplementation with the C-11 choline data improved staging accuracy in 5 of the 18 cases with the fusion of the C-11 choline PET+mpMRI as most accurate in 3 of the 18 cases. The joint analysis of C-11 choline PET with MR also adds confidence to radiologic diagnosis.Conclusion
Our preliminary results demonstrated a comprehensive C-11 choline PET/MRI including body PET/MRI as well as simultaneous focused pelvic PET/MRI and mpMRI improves preoperative staging in untreated patients with high risk prostate cancer. Further analysis of the data is necessary to optimize patient selection for which fusion C-11 choline PET+mpMRI is the most accurate staging modality.Acknowledgements
No acknowledgement found.References
1. Giovacchini, G., Picchio, M., Coradeschi, E., Scattoni, V., Bettinardi, V., Cozzarini, C., … Messa, C. (2008). [11C]Choline uptake with PET/CT for the initial diagnosis of prostate cancer: relation to PSA levels, tumour stage and anti-androgenic therapy. European Journal of Nuclear Medicine and Molecular Imaging, 35(6), 1065–1073.
2. Perez-Lopez, R., Tunariu, N., Padhani, A. R., Oyen, W. J. G., Fanti, S., Vargas, H. A., … Koh, D.-M. (2019). Imaging Diagnosis and Follow-up of Advanced Prostate Cancer: Clinical Perspectives and State of the Art. Radiology, 292(2), 273–286.
3. Schiavina, R., Scattoni, V., Briganti, A., Franceschelli, A., Sanguedolce, F., Bertaccini, A., … Martorana, G. (2008). 11C-Choline-Positron Emission Tomography/ Computerised Tomography For Preoperative Lymph- Node Staging In Intermediate-Risk And High-Risk Prostate Cancer: Comparison With Clinical Staging Nomograms. European Urology Supplements, 7(3), 283.
4. Wibmer, A. G., Burger, I. A., Sala, E., Hricak, H., Weber, W. A., & Vargas, H. A. (2016). Molecular Imaging of Prostate Cancer. RadioGraphics, 36(1), 142–159.
Figures