3026
Rapid Multi-Point B1+ Calibration for Large Field-of-View 13C Imaging1Medical Biophysics, University of Toronto, Toronto, ON, Canada, 2Physical Sciences, Sunnybrook Research Institute, Toronto, ON, Canada, 3GE Healthcare Technologies, Toronto, ON, Canada
Synopsis
This project aims to minimize the B1+ field inhomogeneities that arise when using a flexible transmit coil system in multi-organ hyperpolarized 13C MRI. A method for rapid B1+ measurement of several locations immediately prior to image acquisition was developed to determine scaling factors for the power input of slices over a large field-of-view. These scaling factors ensure that the desired flip angle is achieved across multiple organs. The rapid B1+ measurement technique has been tested in in vivo scans, giving values accurate within ±1μT. This method will be used to minimize the variability in multi-organ thoracic and abdominal imaging.
Introduction
Hyperpolarized 13C MRI often suffers from an inhomogeneous B1+ transmit field, as it requires the use of a secondary transmit coil system within the proton-only body coil. These field inhomogeneities lead to varying flip angles, making the image signals difficult to interpret in a large field-of-view. The varying spatial distribution of the B1+ field for a given transmit coil can be observed using a variety of methods;1,2 however, applying these methods during in vivo 13C scans is infeasible due to timing constraints. Moreover, referencing a pre-measured B1+ map to minimize variation in an in vivo scan is prone to error, as the field distribution varies with coil loading and positioning changes.To account for changes in the B1+ distribution that result from coil loading, some form of B1+ calibration is often performed using a 13C reference phantom placed near the region of interest. However, this calibration becomes inconsistent in large field-of-view applications as there is a distribution of B1+ fields within the target region.
In this work, a method that rapidly obtains multiple B1+ measurements during in vivo scans from multiple 13C reference phantoms is proposed. Placing these reference phantoms strategically within the coil allows for simultaneous calibration of areas that differ in B1+. This provides an opportunity for larger field-of-view imaging than was previously attainable with 13C MRI.
Methods
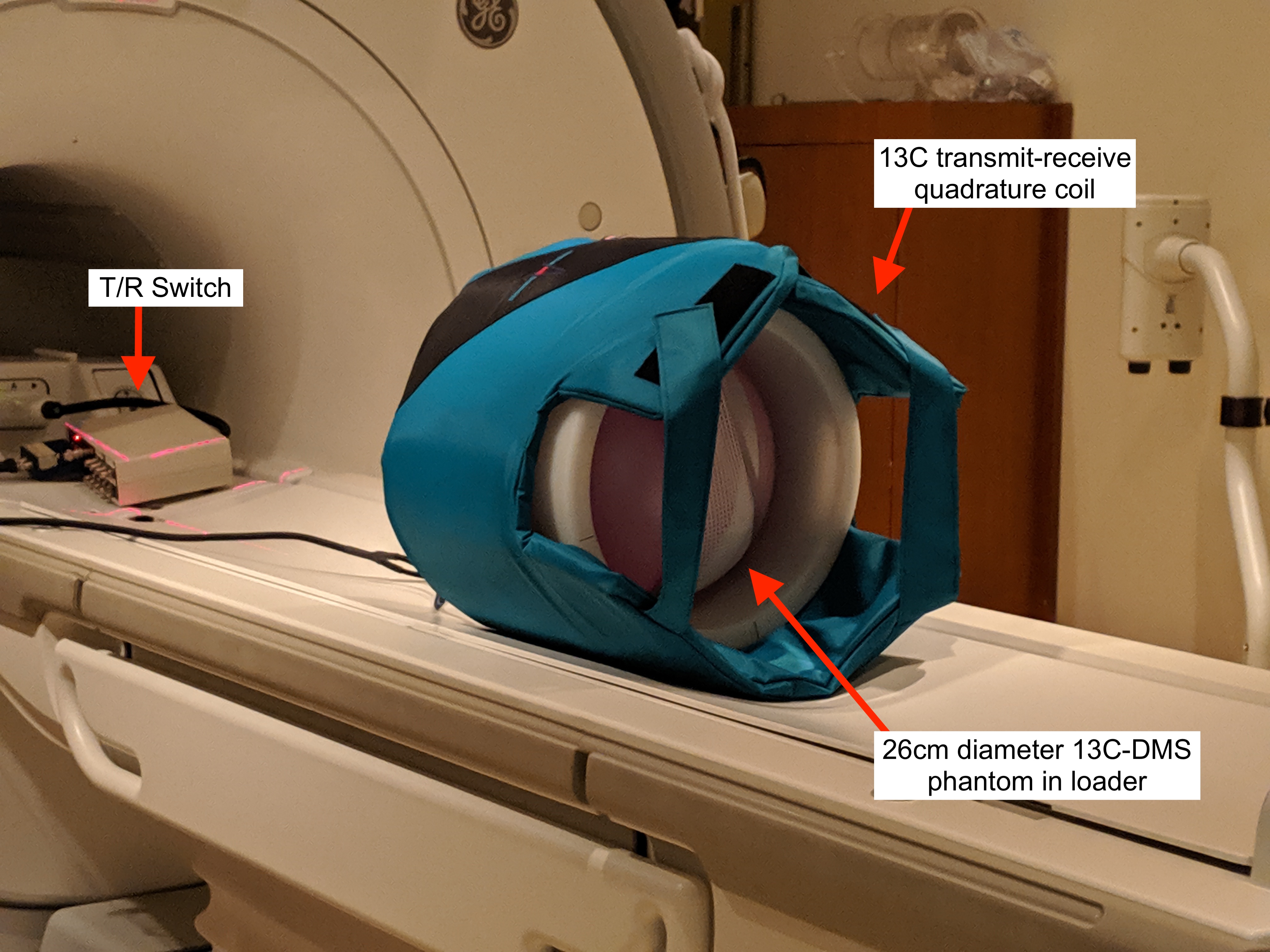
A transmit profile of a flexible 13C transmit-receive quadrature coil (Clinical MR Solutions, Brookfield, WI) (Figure 1) was measured using the double angle method. This spatial map of the transverse component of the B1 field, B1+, is used to determine where to place 13C phantoms for calibration. Phantoms are placed near anatomical regions of interest that show different B1+ in the transmit profile.A short TR pulse-acquire sequence with linearly increasing flip angles was designed to rapidly measure the B1+ at the reference phantoms. With TR = 310 ms and 30 iterations, the total scan time for the measurement is 9 s. The signal evolution from the train of excitations for each phantom creates a characteristic signal response for the particular B1+ at the corresponding location. These values are discrete samples of the B1+ field that is unique to each subject's positioning in the scanner.
The characteristic response is fit to a non-steady state model which determines the measured B1+ of the phantom and outputs the power adjustment required to achieve the desired B1+. These adjustment values will be input as control variables for the sequence, such that the power adjustment occur automatically. This will minimize the variability in the B1+ field that occurs towards the edges of the coil.
Results & Discussion
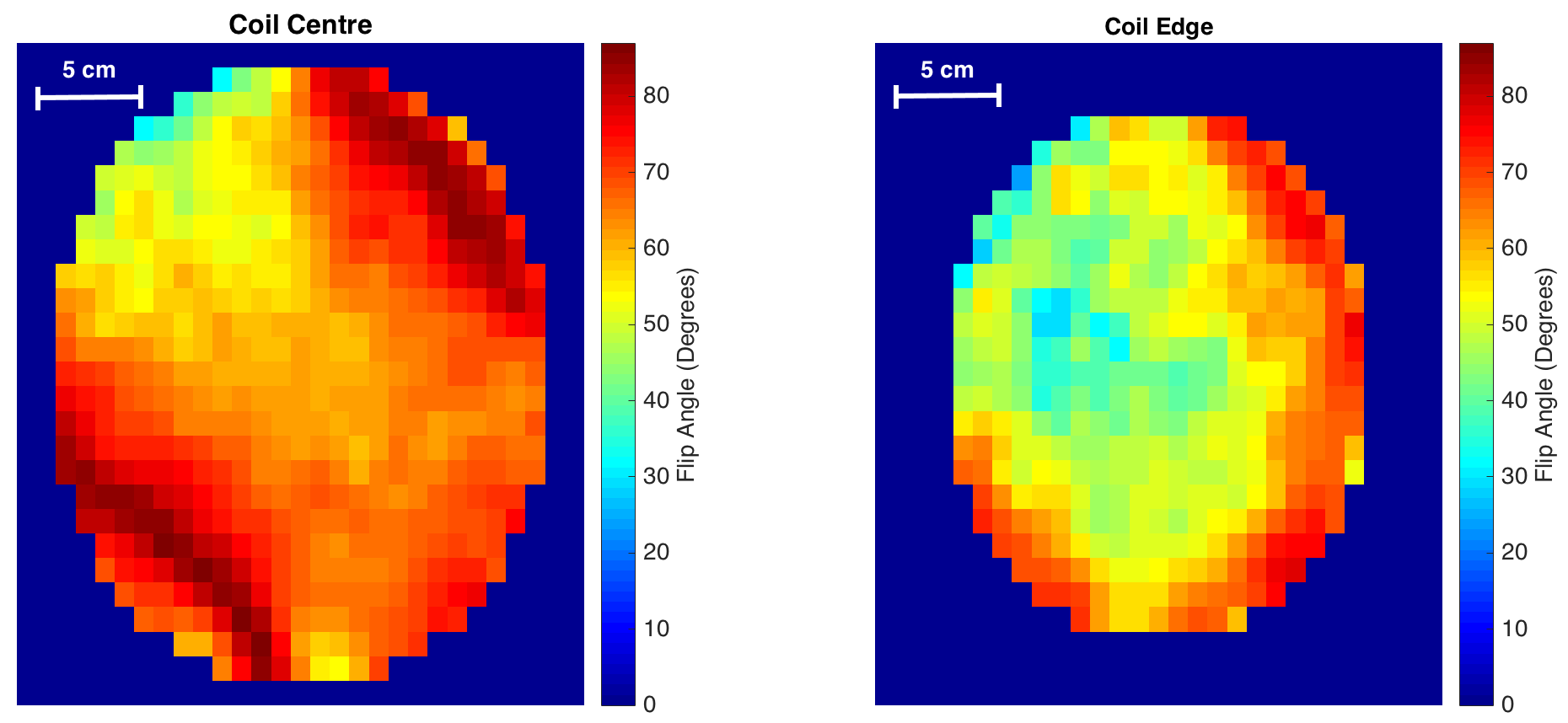
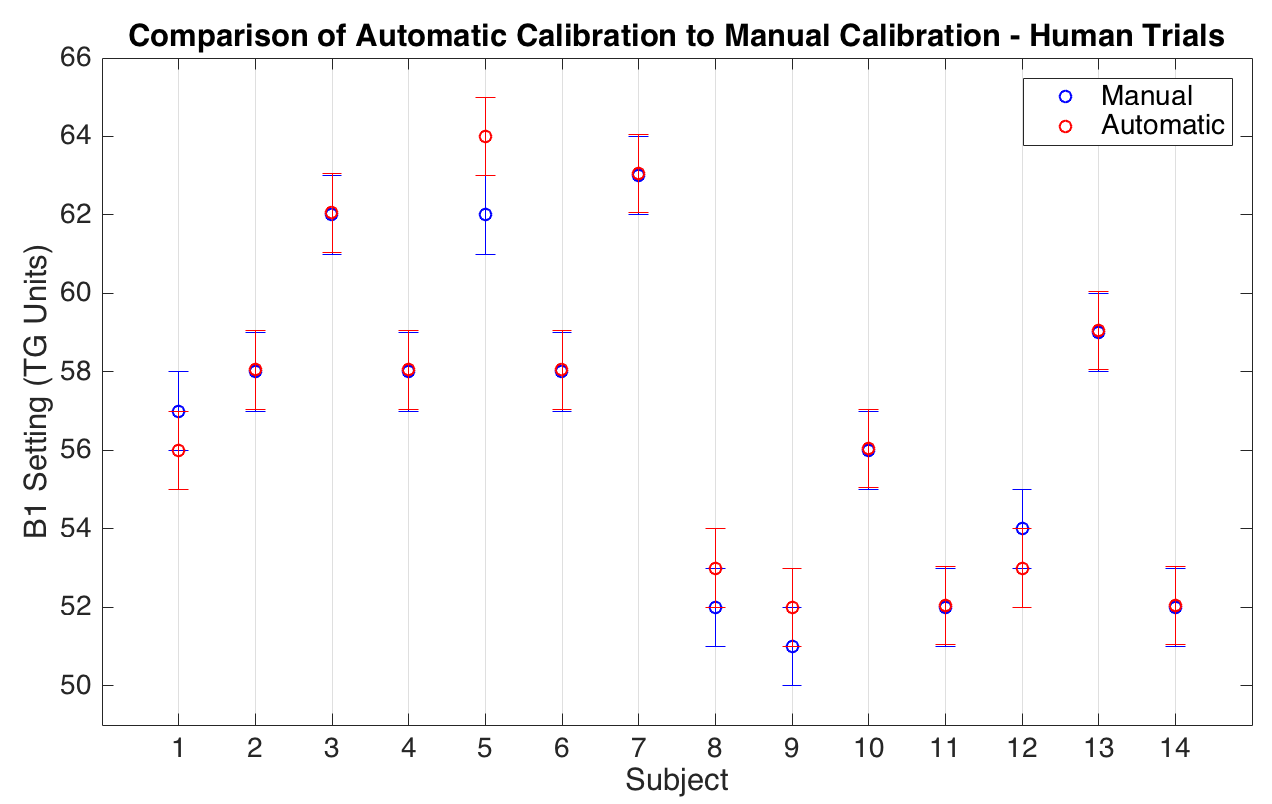
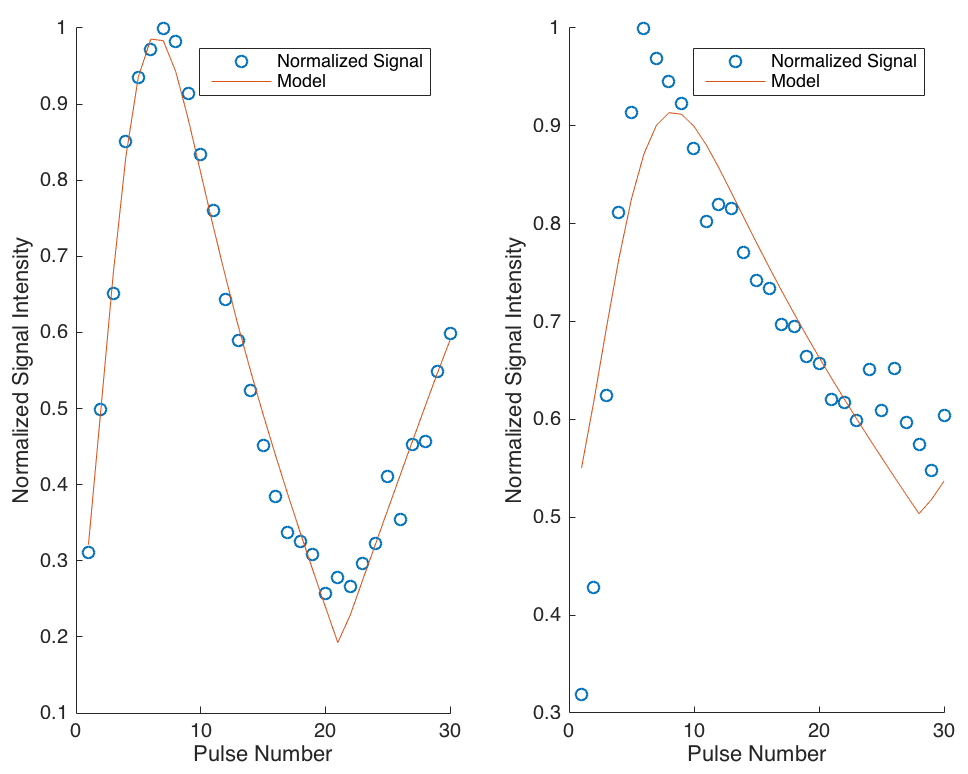
Two axial slices of the pre-computed B1+ map used to determine the location of the reference phantoms is shown in Figure 2. The relative B1+ distribution of these slices, one central to the coil and one near the edge, show the variability that occurs towards the coil perimeter. Such variability supports the need for a method that can correct for this in large field-of-view imaging.The rapid (9 s) B1+ measurement sequence was tested during human scans (n=14) using a 13C-urea phantom, showing that this method is capable of computing the B1+ field accurately within ±1μT. A comparison of B1+ measurements found using this method to manual measurements for each subject is shown in Figure 3. A sample calibration plot showing the non-steady state model fit to the signal responses of two reference phantoms obtained simultaneously is shown in Figure 4. This validates the ability of this method to acquire multiple point B1+ measurements simultaneously.
In the future, this method will be included in the scan protocol for hyperpolarized 13C MRI of the heart and kidneys to enable rapid calibration for slice-specific B1+ scaling.
Conclusion
A method was developed and validated for acquisition of rapid (9 s) B1+ field measurements from multiple 13C reference phantoms used during human 13C metabolic imaging. The method shown here can be used to minimize the variability in flip angle due to inhomogeneous B1+ in large field-of-view images, such as those containing the thoracic and upper abdominal cavities.Acknowledgements
The authors thank Julie Green and Sumeet Sachdeva for coordinating the study, and Ruby Endre for MR technical support. Funding support from the Canadian Institutes for Health Research Grant PJT152928.
References
1. Hornak JP, Szumowski J. Magnetic field mapping. Magn Reson Med. 1988;6:158-163.
2. Sacolick LI, Wiesinger F, Hancu I, Vogel MW. B1 mapping by Bloch-Siegert shift. Magn Reson Med. 2010;63(5):1315-22.
Figures