2941
Neurochemical Deregulation in Post-traumatic Stress Disorder1School of Clinical Sciences, Queensland University of Technology, Brisbane, Australia, 2Translational Research Institute, Woolloongabba, Australia, 3Griffith University, Brisbane, Australia
Synopsis
2D L-COSY has previously been used to demonstrate neurochemical differences between PTSD and healthy cohorts but requires a 19 minute acquisition. Single Voxel Spectroscopy (SVS), acquired in 3 minutes, was used to collect data from 3 brain regions in healthy controls and patients with Post-traumatic Stress Disorder. Neurochemical differences were seen in all the ACC, Thalamus and PCG. Data, analysed using LC Model, showed elevated levels of NAA, Lactate, GABA and Glutathione as well as glutamatergic dysfunction. Thus, SVS can be used to identify PTSD in a shorter time frame than 2D L-COSY.
Introduction
Posttraumatic stress disorder (PTSD) is a debilitating mental health condition precipitated by experiencing or witnessing a terrifying event(s). A pilot study of PTSD patients, primarily with trauma resulting from occupational traumatic exposure in emergency services and the police force, reported significant neurochemical differences when compared with healthy controls using in vivo neuro two-dimensional COrrelated SpectroscopY (COSY) in a clinical 3T MR scanner1. The method identified specific neurochemical changes not previously recorded. Here we have evaluated if in-vivo one-dimensional spectroscopy (1D), can provide similar information in a considerably shorter time.Materials and Methods
Patients and Healthy ControlsInstitutional Ethics approval was received. We recruited a total of 68 participants, 29 with PTSD and 39 healthy controls, from newspaper advertisements, local psychiatrists and psychologists. PTSD subjects were eligible if they had been diagnosed with PTSD according to the DSM-V using the Clinician-Administered PTSD scale (CAPS)2 and were aged between 18-65 yrs. Healthy control participants were aged between 18-65 years and had no current DSM-V Axis I disorder, as assessed by the Structured Clinical Interview for DSM V (SCID)3. The additional inclusion criteria for the control group and exclusion criteria for the PTSD group have been described elsewhere4. The groups were approximately matched for age and gender. A clinical psychologist interviewed all participants and administered the CAPS, SCID/IP and Life Events Checklist (LEC)5.
MRI and MRS
All scans were performed on a 3T Prisma (Siemens, Erlangen, Germany, software version VD13D and VE11C) with a 64-channel head and neck coil (Siemens, Erlangen).
Structural Imaging
A 3D T1-weighted magnetisation-prepared rapid gradient-echo (MPRAGE) was acquired (TR/TE/TI=2530/3.5/1100ms, flip angle=7°, FOV=256x256 mm, voxel size 1x1x1mm3, IPAT=3, acquisition time 4:28 minutes) and used for MRS voxel placement and whole-brain morphometry.
1D MRS acquisition
1D spectroscopy was acquired from three different brain regions, the anterior cingulate cortex (2x2x2cm3), thalamus (1.9x1.9x1.7cm3) and posterior cingulate gyrus (3x3x3 cm3). The 1D acquisition parameters were as follows: TR/TE: 1500/30ms, 96 averages, bandwidth 1200 Hz, delta frequency -2.3ppm, 1024 points. Acquisition time 3:22. Partial volume correction was performed using an in-house script utilising the ‘Suspects’ package6. Partial volumes were determined using FSL FAST7. Spectral Analysis was undertaken using LCModel8.
Statistical Analysis
Since the distribution of some metabolites exhibit partial deviation from normality, we also chose to perform Mann-Whitney tests as a non-parametric validation (p<0.05).
Results
PTSD and Healthy Volunteer CohortsThe average CAPS score for the PTSD cohort was 39.7 (± 9.8). The healthy controls were all evaluated and found to be normal.
1D spectroscopy
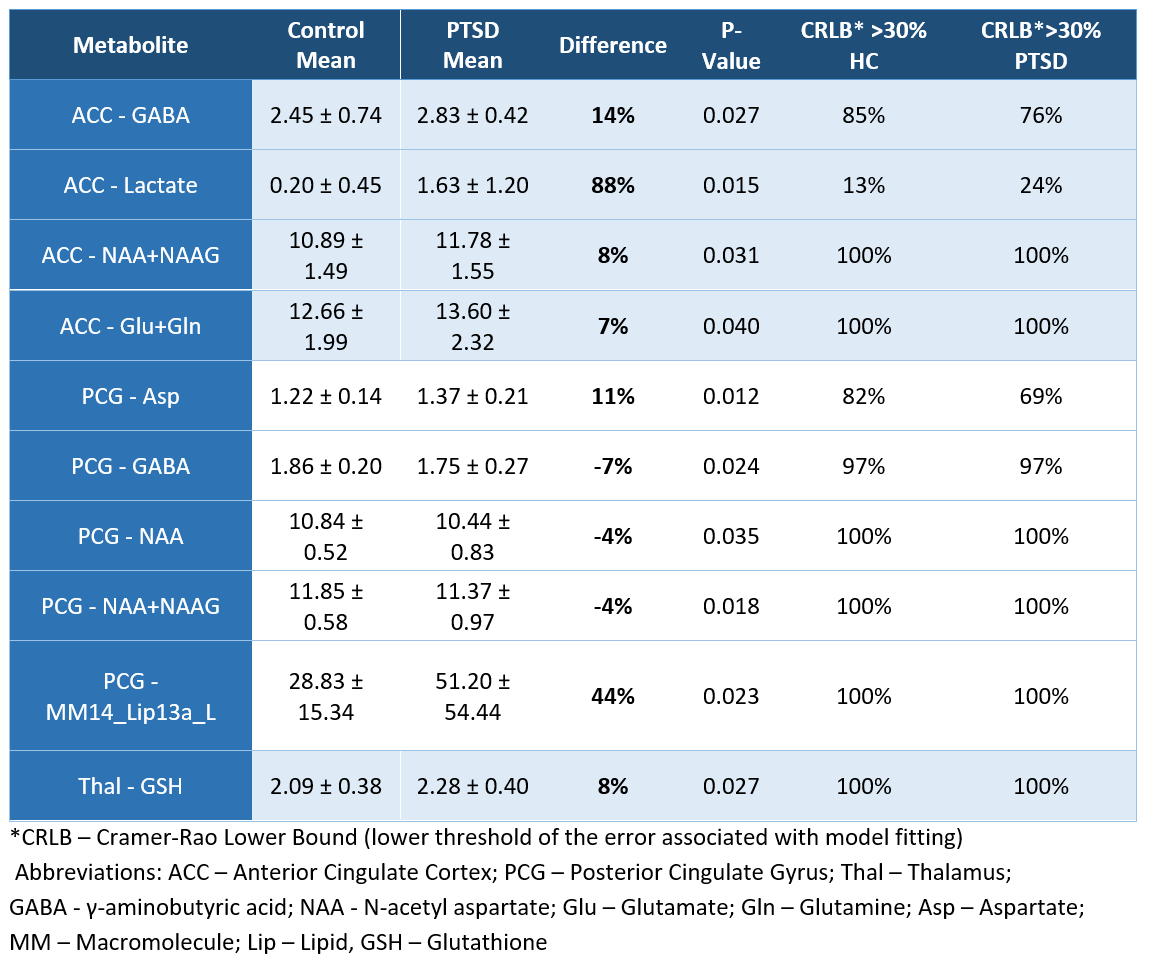
There were significant differences recorded between the healthy control cohort and the PTSD cohort in each of the three brain regions evaluated (Table 1). In the PTSD cohort in the PCG there were increases recorded in Aspartate (11%), composite resonance at 1.2ppm (44%) and decreases in γ-aminobutyric acid (GABA, -7%), N-acetyl aspartate (-4%) and N-acetyl aspartate + N-acetylaspartyl glutamate (-4%). In the ACC increases were recorded in GABA (14%), Lactate (88%), N-acetyl aspartate/N-acetylaspartyl glutamate (8%) and Glutamate/Glutamine (7%). The only statistically significant changes recorded in the Thalamus was an increase in Glutathione (8%).
Discussion
We have reported previously that It was possible to distinguish between the PTSD and healthy control groups using in vivo 1D MRS where the data was mined using modern informatics9. Here, using the LCModel method of evaluating the spectra, differences were recorded in each of the three brain regions examined. While tNAA was increased in the ACC, it was reduced in the PCG. The increased tNAA in the PTSD cohort is contrary to other reports of previous studies, where a reduction in total NAA has been reported. However, the directionality of NAA change is known to fluctuate in PTSD, and the current group are chronic PTSD sufferers, potentially explaining this finding. A small reduction in total NAA was identified in the PCG, which is more consistent with previous literature.The increase in the composite glutamine/glutamate resonances in the ACC of the PTSD cohort provides evidence of glutamatergic dysfunction. Furthermore, the PTSD group demonstrated increased GABA levels within the ACC, a finding in keeping with the study by Michels et. al10. Reduced GABA was noted in the PTSD cohort within the PCG, and no previous reports have identified GABA to alter with PTSD in the PCG, but others did identify reduced GABA/creatine in the insular cortex11 and GABA/creatine within the posterior occipital cortex and medial temporal lobes12.
The increase in measured glutathione within the thalamus of the PTSD cohort fits with previous findings. Glutathione is a marker of oxidative stress and is an emerging biomarker of importance in cognitive impairment in Alzheimer’s disease13 and potentially in PTSD10. Michels et. al10 identified an increased glutathione to creatine ratio in the ACC and dorsolateral prefrontal cortex of patients with PTSD when compared to trauma-exposed controls.
While the 1D method has far less information available than 2D L-COSY the time taken is only 3:22mins compared with 19:12mins for 2D MRS.
Conclusion
Biochemical differences have been recorded in a PTSD cohort compared to a healthy control group using in vivo 1D spectroscopy analysed by the LCModel method. The differences include altered NAA, GABA, Glutathione, Lactate and glutamatergic dysfunction in those with PTSD.Acknowledgements
Funding
This study was funded by the Department of Defence of Australia and Department of Defence USA under the MOU and task plan PP-3664-9 concerning combating terrorism research and development and USA Departments of Defence; and the Advance Queensland funding initiative to establish The Translational Research Institute (TRI) Innovation and Translation Centre (IAT Centre) in co-operation with Siemens Healthcare.
Conflict of Interest
CM and SQ have registered a Provisional Patent on the use of 2D COSY to evaluate the neurochemistry of patients with PTSD.
References
(1) Quadrelli, S.; Tosh, N.; Urquhart, A.; Trickey, K.; Tremewan, R.; Galloway, G.; Rich, L.; Lea, R.; Malycha, P.; Mountford, C. Post-traumatic stress disorder affects fucose-α (1–2)-glycans in the human brain: preliminary findings of neuro deregulation using in vivo two-dimensional neuro MR spectroscopy. Translational Psychiatry 2019, 9 (1), 27.
(2) Blake, D. D.; Weathers, F. W.; Nagy, L. M.; Kaloupek, D. G.; Gusman, F. D.; Charney, D. S.; Keane, T. M. The development of a Clinician-Administered PTSD Scale. J. Trauma. Stress 1995, 8 (1), 75.
(3) First, M. B., Spitzer, Robert L, Gibbon Miriam, and Williams, Janet B.W Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition (SCID-I/P); New York State Psychiatric Institute: New York, 2002.
(4) Quadrelli, S.; Tosh, N.; Urquhart, A.; Trickey, K.; Tremewan, R.; Galloway, G.; Rich, L.; Lea, R.; Malycha, P.; Mountford, C. Post-traumatic stress disorder affects fucose-alpha(1-2)-glycans in the human brain: preliminary findings of neuro deregulation using in vivo two-dimensional neuro MR spectroscopy. Transl Psychiatry 2019, 9 (1), 27.
(5) Weathers, F. W., Blake, D.D., Schnurr, P.P., Kaloupek, D.G., Marx, B.P., & Keane, T.M. The Life Events Checklist for DSM-5 (LEC-5), 2013.
(6) Rowland, B. C.; Liao, H.; Adan, F.; Mariano, L.; Irvine, J.; Lin, A. P. Correcting for Frequency Drift in Clinical Brain MR Spectroscopy. J. Neuroimaging 2017, 27 (1), 23.
(7) Zhang, Y.; Brady, M.; Smith, S. Segmentation of brain MR images through a hidden Markov random field model and the expectation-maximization algorithm. IEEE Trans. Med. Imaging 2001, 20 (1), 45.
(8) Provencher, S. W. Estimation of metabolite concentrations from localized in vivo proton NMR spectra. Magnetic resonance in medicine 1993, 30 (6), 672.
(9) Tosh, N., Mariano, Laura, Quadrelli, Scott, Galloway, Graham, Graves, Valerie, Urquhart, Aaron, Malycha, Peter, Trickey, Katie, Rich, Lisa, Tremewan, Rosanna, Irvine, John, Mountford, Carolyn. In Proceedings of the Joint Annual Meeting ISMRM-ESMRMB; ISMRM: Paris, France, 2018.
(10) Michels, L.; Schulte-Vels, T.; Schick, M.; O'Gorman, R. L.; Zeffiro, T.; Hasler, G.; Mueller-Pfeiffer, C. Prefrontal GABA and glutathione imbalance in posttraumatic stress disorder: preliminary findings. Psychiatry Res. 2014, 224 (3), 288.
(11) Rosso, I. M.; Weiner, M. R.; Crowley, D. J.; Silveri, M. M.; Rauch, S. L.; Jensen, J. E. Insula and anterior cingulate GABA levels in posttraumatic stress disorder: preliminary findings using magnetic resonance spectroscopy. Depress. Anxiety 2014, 31 (2), 115.
(12) Meyerhoff, D. J.; Mon, A.; Metzler, T.; Neylan, T. C. Cortical gamma-aminobutyric acid and glutamate in posttraumatic stress disorder and their relationships to self-reported sleep quality. Sleep 2014, 37 (5), 893.
(13) Saharan, S.; Mandal, P. K. The emerging role of glutathione in Alzheimer's disease. J. Alzheimers Dis. 2014, 40 (3), 519.
Figures