2838
Osteochondral Junction Imaging Using Adiabatic Inversion Recovery Prepared Fat-Saturated Zero Echo Time MR Imaging: A Feasibility Study1University of California, San Diego, San Diego, CA, United States, 2GE Healthcare, La Jolla, CA, United States, 3VA San Diego Healthcare System, San Diego, CA, United States
Synopsis
Cartilage has a complex structure comprised of multiple zones with different MR signal properties. Among them, osteochondral junction (OCJ) cannot be directly imaged with conventional MR imaging techniques. In this study, we explore the feasibility of inversion recovery prepared fat-saturated zero echo time (IR-FS-ZTE) to image the human knee OCJ. To accentuate the signal from the OCJ region with short T2*, adiabatic inversion recovery along with fat-saturation preparation was applied, followed by continous, slient ZTE imaging. The feasibility and efficacy of IR-FS-ZTE were shown in ex vivo cadaveric human knee joints and in in vivo healthy volunteers.
Introduction
Osteoarthritis (OA) is one of the most common joint disease, afflicting ~30 million people in the US alone1. Degeneration of articular cartilage usually accompanies OA, making it a common indicator for diagnosis and prognosis of the disease. Cartilage has a complex structure comprised of multiple zones: superficial, intermediate, deep, and calcified layer. Osteochondral junction (OCJ) is the region where calcified cartilage meets subchondral bone. Recently, it has been shown that inversion recovery (IR) prepared ultrashort echo time (UTE) imaging can directly resolve the short T2* signal from the OCJ region2. In this study, we explore the feasibility and efficacy of IR prepared fat saturated zero echo time (IR-FS-ZTE) for imaging the OCJ region in a human knee.Methods
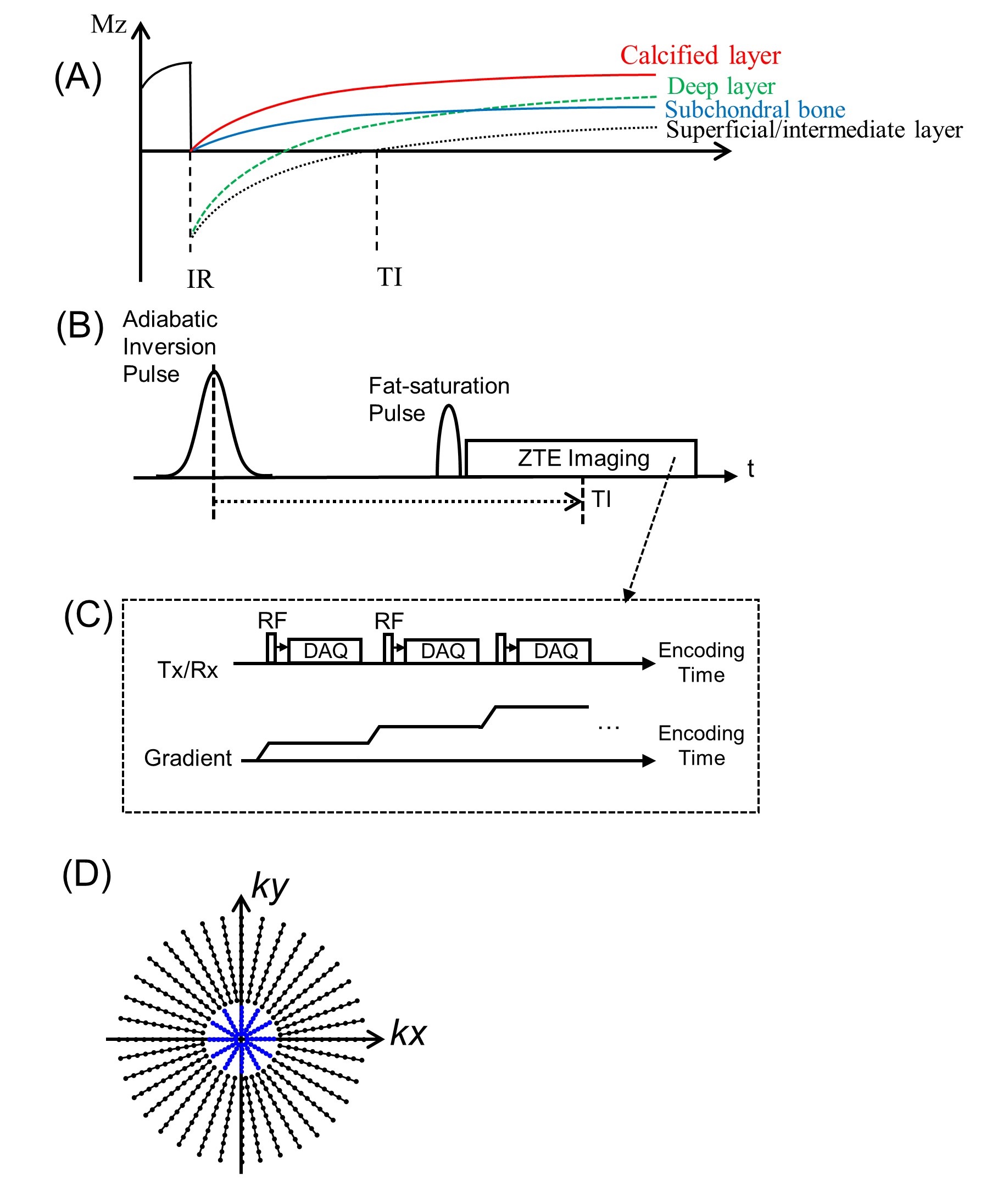
Figure 1-A illustrates a typical inversion recovery curve in the different cartilage layers and subchondral bone. Due to the short T2* (<1ms), the longitudinal magnetization in calcified layer and subchondral bone is not inverted, but partially saturated, by the relatively long adiabatic inversion pulse (~10 ms). By selecting TI tuned to the nulling point of the superficial/intermediate layer, the signal from OCJ region can be accentuated, allowing improved image contrast and dynamic range for the short T2 component. Figure 1-B shows a pulse sequence for the signal preparation, where an adiabatic inversion recovery is followed by fat saturation to suppress signal from tissues in the superficial/intermediate layer and marrow fat simultaneously. Then, silent ZTE imaging is performed immediately after the fat-saturation pulse, where multiple spokes are continuously acquired with smoothly rotating readout gradient, as shown in Figure 1-C. Unfortunately, ZTE encoding inevitably leaves a hole of missing data in the encoded k-space due to the RF coil deadtime (a blind time during RF transit/receive mode switching). In this study, the hole was filled with additional encoding with a reduced readout bandwidth (BW), as in Water- and Fat-suppressed Proton Projection MRI (WASPI)3, as illustrated with blue dots in Figure 1-D.The 3D IR-FS-ZTE sequence was implemented on a 3T clinical scanner (MR750, GE Healthcare, Waukesha, WI, USA) and evaluated with three cadaveric human knee joints (81F, 61M, and 57M donors) and three healthy volunteers (28M, 35M, and 36M) using an 8-channel transmit/receive knee coil (GE Healthcare). MR imaging parameters were as follows: 1) IR-FS-ZTE: an adiabatic inversion pulse (GE Silver-Hoult pulse with width of 8.64ms and BW of 1.5kHz); a GE standard fat-saturation pulse; a 24μs hard pulse; flip angle=8o; readout BW=62.5kHz; FOV=13x13x8cm3; matrix=256x256x40 (ex vivo) or 220x220x40 (in vivo); TR/TE=1200ms/12μs; TI=200, 300, 420, 520, and 700ms (ex vivo) or 580ms (in vivo); RF-to-RF timing=2.3ms (ex vivo) or 1.9ms (in vivo); number of spokes per IR=24 (ex vivo) or 36 (in vivo); and scan time=25min 20sec (ex vivo) or 9min 58sec (in vivo); 2) FS-ZTE: no IR preparation, other parameters matched with IR-FS-ZTE, scan time = 1min 41sec; 3) PDw-FSE: FOV=15×15cm2, matrix=352×256, TR/TE=3220ms/27.8ms, number of slices=40, acceleration factor=2, and scan time=2min 30sec; 4) T2w-FSE: FOV=15×15cm2, matrix=352×256, TR/TE=7585/71.5 ms, number of slices=40, acceleration factor=2, scan time=2min 32sec.
All MR images were reconstructed using online reconstruction based on GE Orchestra SDK v1.7.1. The following gridding parameters were used: alpha=2 and kernel width=3 data points. Density function was analytically calculated based on the inter-spoke distance and intra-spoke sampling density. The low resolution k-space data acquired using WASPI were combined with high resolution data using a linear merging filter with width of 2 data points. The reconstructed images in each RF receiver channel were combined using weighted sum of squares method, in which the weighting factors were calculated based on the noise power in each channel.
Results
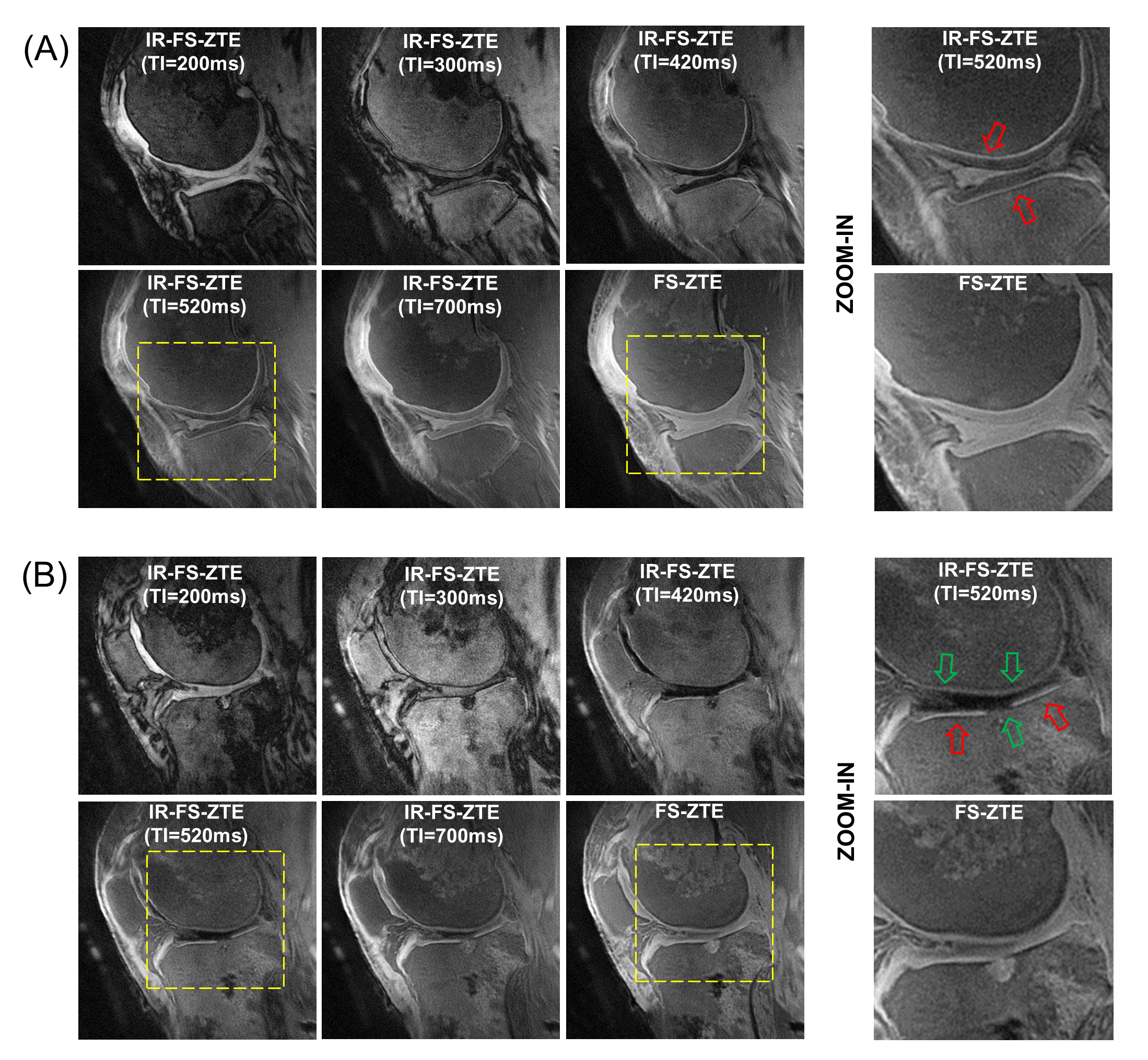
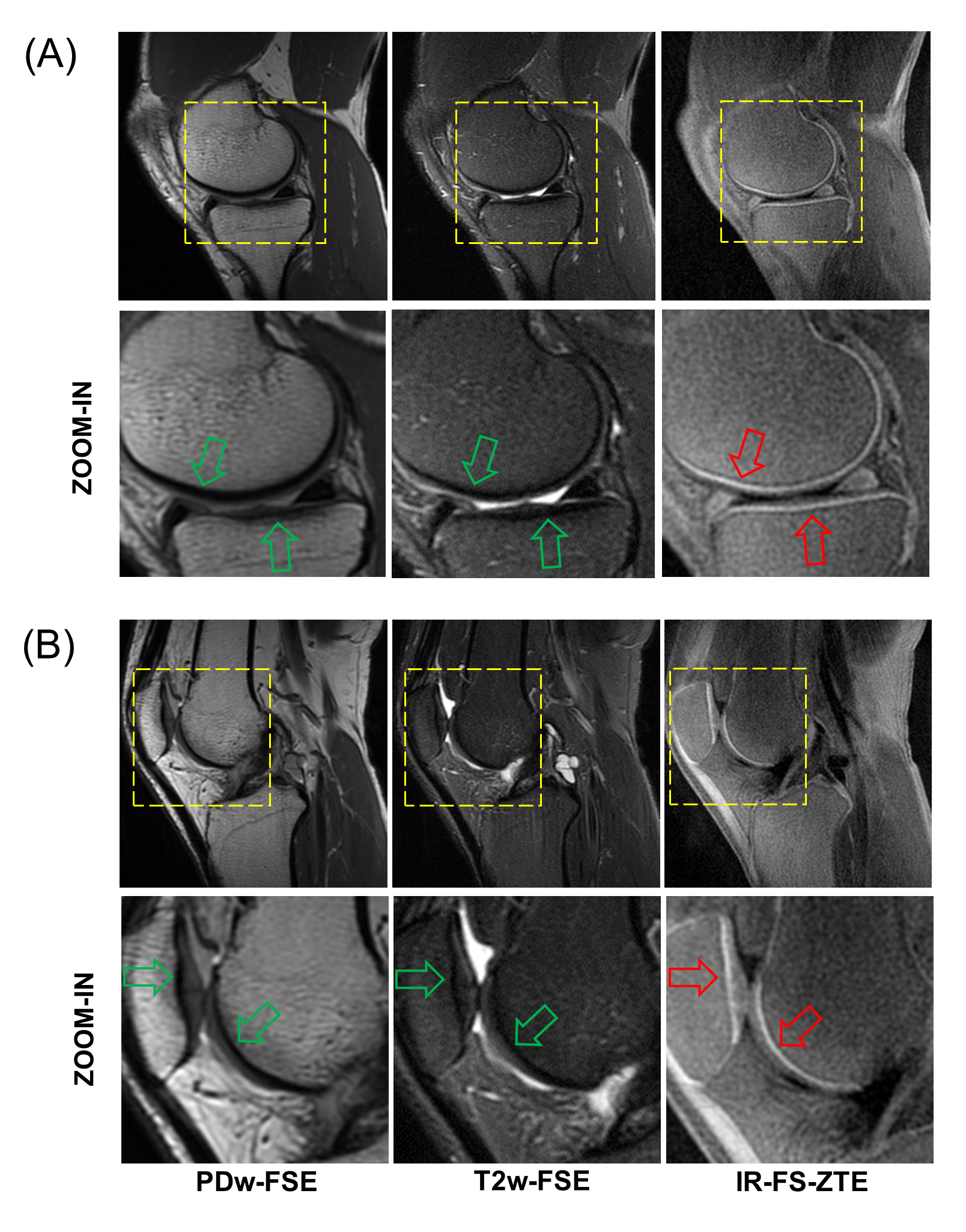
Figure 2 shows the IR-FS-ZTE images from a representative ex vivo knee sample (from an 81-year-old female donor) acquired with the five different TIs (200, 300, 420, 520, and 700ms) and the FS-ZTE image as a comparison. The IR-FS-ZTE with TI=520ms showed the best contrast for the OCJ region. Compared to the FS-ZTE, the IR-FS-ZTE clearly revealed the morphology in the OCJ region (red arrows) and the degenerated lesion (green arrows). Figure 3 shows the IR-FS-ZTE images from a representative healthy volunteer (35-year-old male). In the clinical sequences, the signal from the OCJ region is invisible due to the short T2 decay (green arrows). The proposed IR-FS-ZTE shows the high signal intensity from the OCJ region owing to the adiabatic IR preparation, fat saturation, and near-zero TE (red arrows).Discussion and Conclusion
In this study, we developed and evaluated the feasibility of IR-FS-ZTE MR sequence for imaging of the OCJ region. In the ex vivo and in vivo experiments, the proposed IR-FS-ZTE showed highly specific morphological imaging of the OCJ region. Potentially, the proposed IR-FS-ZTE can be advantageous over other IR-FS-UTE techniques in terms of faster encoding for the signal with extremely short T2* due to the near-zero nominal TE (12μs) and shorter effective TE due to the constant gradient encoding (no need for ramping up gradients). Moreover, the reduced acoustic noise compared with other UTE sequences could be beneficial for patient comfort4. However, ZTE is limited in FA and readout BW5. In future studies, we will systematically compare ZTE with other UTE techniques2,6–8 in phantoms, ex vivo samples, and in vivo subjects.Acknowledgements
The authors acknowledge grant support from NIH (R01AR075825, 2R01AR062581, 1R01 AR068987), Veterans Affairs (Merit Awards 1I01RX002604), and GE Healthcare.References
1. Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis Rheum. 2008;58:26–35.
2. Ma Y, Jerban S, Carl M, et al. Imaging of the region of the osteochondral junction (OCJ) using a 3D adiabatic inversion recovery prepared ultrashort echo time cones (3D IR‐UTE‐cones) sequence at 3 T. NMR Biomed. 2019;32:e4080.
3. Wu Y, Dai G, Ackerman JL, et al. Water- and fat-suppressed proton projection MRI (WASPI) of rat femur bone. Magn. Reson. Med. 2007;57:554–567.
4. Weiger M, Brunner DO, Dietrich BE, Müller CF, Pruessmann KP. ZTE imaging in humans. Magn. Reson. Med. 2013;70:328–332.
5. Cheng Li, Magland JF, Seifert AC, Wehrli FW. Correction of Excitation Profile in Zero Echo Time (ZTE) Imaging Using Quadratic Phase-Modulated RF Pulse Excitation and Iterative Reconstruction. IEEE Trans. Med. Imaging 2014;33:961–969.
6. Jang H, Ma Y, Searleman AC, et al. Inversion recovery UTE based volumetric myelin imaging in human brain using interleaved hybrid encoding. Magn. Reson. Med. 2019:mrm.27986 doi: 10.1002/mrm.27986.
7. Jang H, Lu X, Carl M, et al. True phase quantitative susceptibility mapping using continuous single‐point imaging: a feasibility study. Magn. Reson. Med. 2019;81:1907–1914.
8. Lee YH, Suh JS, Grodzki D. Ultrashort echo (UTE) versus pointwise encoding time reduction with radial acquisition (PETRA) sequences at 3 Tesla for knee meniscus: A comparative study. Magn. Reson. Imaging 2016;34:75–80.
Figures