2830
Using Compressed Sense Technique for Lumbar Vertebra Imaging: Comparison with Conventional Parallel Imaging
Tianyang Gao1, Shinong Pan1, Zhao Lu1, Fengzhe Wang1, and Jiazheng Wang2
1Shengjing Hospital of China Medical University, Shenyang, China, 2Clinical Science, Philips Healthcare, Beijing, China
1Shengjing Hospital of China Medical University, Shenyang, China, 2Clinical Science, Philips Healthcare, Beijing, China
Synopsis
SENSE-TSE is widely used in routine joint scanning, which requires a considerable length of scan duration. Staying in the same position for a long time inevitably causes discomfort and unwanted movement of patients, resulting in image quality degradation. Therefore, shortening imaging time to reduce motion artifacts has become an important goal in the application of CS acceleration in clinical practice.This study aims to retrospectively compare the image quality and diagnosis accuracy of CS-TSE and SENSE-TSE in lumbar vertebra MRI.
Introduction
Compressed SENSE technology is built on compressed sensing theory and SENSE technology by leveraging a balanced variable density incoherent undersampling acquisition scheme and iterative reconstruction to solve an inverse problem with a sparsity constraint1.With the purpose of this study is to compare conventional sensitivity encoding turbo spin echo (SENSE-TSE) to compressed sensing plus SENSE turbo spin echo (CS-TSE) in lumbar vertebra MRI.Methods
A retrospective analysis of lumbar vertebra MRI from 600 patients, including 300 patients with SENSE-TSE and 300 patients with CS-TSE. The SENSE acceleration factor of the SENSE-TSE was 1.4 for T1WI, 1.7 for T2WI and 1.7 for PDWI. The CS total acceleration factor was 2.4, 3.6, 4.0and 4.0 for T1WI, T2WI and PDWI sagittal, and T2WI transverse, respectively. The image quality of all sequences was evaluated objectively by SNR and CNR. The subjective image quality was evaluated by the five-point scale method2. Two radiologists independently diagnosed 300 cases of CS-TSE and their consistency was evaluated. The degree of intervertebral foraminal stenosis and nerve root compression3 was evaluated by T1WI sagittal and T2WI transverse of CS-TSE.The sensitivity, specificity, positive predictive value and negative predictive value of these two sequences were compared.Results
The scan time of using CS-TSE was reduced from 7min28s to 4min26s. There was no significant difference between SNR, CNR and subjective evaluation of two sequences. The subjective median score of nerve roots image quality was 5 points. Two radiologists were highly consistent in diagnosing lumbar diseases(κ> 0.750) and evaluating the degree of lumbar foraminal stenosis and nerve root compression (κ= 0.882) by using CS-TSE. The Sensitive, Specificity, Positive predictive value and Negative predictive value of two sequences had no difference.Discussion
In this study, the MR images on lumbar vertebra remained acceptable when CS acceleration is incorporated into TSE acquisition, while the imaging time was cut down by approximately 40%,similar to the results previously reported4-6.In the objective evaluation of image quality SNR and CNR, although the SNR and CNR of some parts acquired by the CS-TSE were lower than that of SENSE-TSE, the difference was not significant (p > 0.050). The overall image results of the PDWI,T1WI and T2WI scans using CS-TSE were considered sufficient for routine clinical practice, as exampled in Fig.1-2.In T1WI images of SENSE-TSE and CS-TSE, the two reviewers made very similar rating on the image quality for the contours of nerve root where no CSF presented in the background , as exampled in Fig.3.The two radiologists showed used CS-TSE to diagnose lumbar vertebral diseases with a high consistency by using CS-TSE, all κ were greater than 0.750. CS-TSE was highly consistent in evaluating the degree of lumbar foraminal stenosis and nerve root compression (κ= 0.882), as exampled in Fig.4.Conclusion
This retrospective study showed that the combination of Compressed SENSE and TSE sequence is a potential tool in lumbar vertebra and intervertebral disc disease diagnosis, provided the similar image quality, diagnostic consistency, and dramatically reduced imaging time when compared to the SENSE-TSE sequence. The reduced imaging time could potentially improve the patient comfortableness, enhance the hospital patient throughput, and be exploited to acquire more information at higher imaging resolution for better diagnosis of osteoarthrosis.Acknowledgements
No acknowledgement found.References
- F, L., et al., Compressed sensing MRI combined with SENSE in partial k-space. Physics in medicine and biology, 2012. 57(21): p. N391-403.
- Hu, Y., et al., Value and Clinical Application of Orthopedic Metal Artifact Reduction Algorithm in CT Scans after Orthopedic Metal Implantation. Korean Journal of Radiology, 2017. 18(3): p. 526.
- Lee, S., et al., A Practical MRI Grading System for Lumbar Foraminal Stenosis. American Journal of Roentgenology, 2010. 194(4): p. 1095-1098.
- Altahawi, F.F., et al., Comparing an accelerated 3D fast spin-echo sequence (CS-SPACE) for knee 3-T magnetic resonance imaging with SENSE 3D fast spin-echo (SPACE) and routine 2D sequences. Skeletal Radiol, 2017. 46(1): p. 7-15.11.
- Kijowski, R., et al., Knee imaging: Rapid three-dimensional fast spin-echo using compressed sensing. Journal of Magnetic Resonance Imaging, 2017. 45(6): p. 1712-1722.13.
- Lee, S.H., et al., Rapid acquisition of magnetic resonance imaging of the shoulder using three-dimensional fast spin echo sequence with compressed sensing. Magnetic Resonance Imaging, 2017. 42: p. 152-157.
Figures

Fig.1.1: 45-year-old male patient with low back pain for one week were examined by SENSE-TSE.Fig.1.2: 43-year-old male patient with radiation pain of left lower limb were examined by CS-TSE.
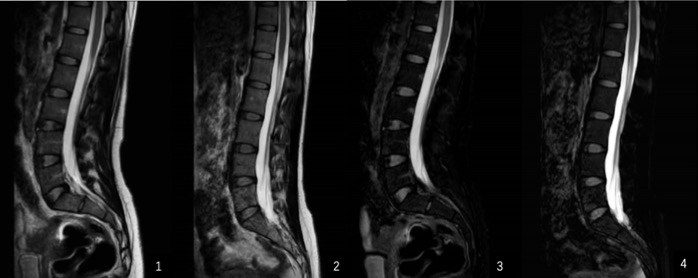
Fig.2.1 and 3: T2WI and PDWI of SENSE-TSE was used for 35-year-old female patient with low back pain for 1 year.Fig.2.2 and 4: T2WI and PDWI of CS-TSE was performed on a 40-year-old female patient with lumbar back discomfort for 6 months.
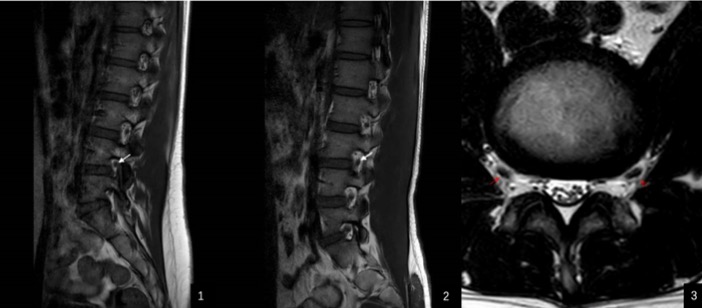
Fig.3.1: SENSE-TSE-T1WI, Fig.3.2: CS-TSE-T1WI, Fig.3.3: CS-TSE-T2WI.
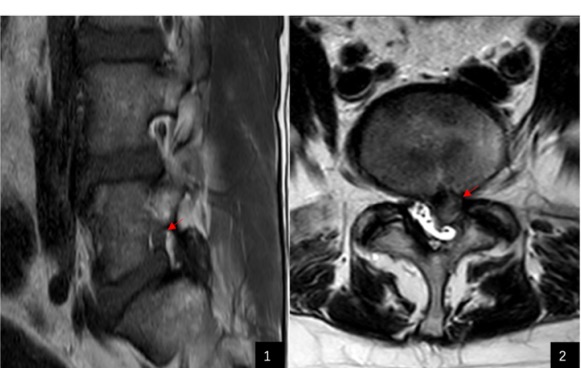
Fig.4.1: Grade 1 foraminal stenosis, Fig.4.2: Grade 3 foraminal stenosis.