2828
Feasibility of Rapid MRI Assessment of Leg Alignment1Department of Radiology, Stanford University, Stanford, CA, United States, 2Department of Mechanical Engineering, Stanford University, Stanford, CA, United States, 3Palo Alto Veterans Affairs Hospital, Palo Alto, CA, United States
Synopsis
Varus and valgus alignment are associated with the presence and progression of knee osteoarthritis. We assessed the feasibility of rapidly assessing leg alignment with a non-weight bearing MRI in under a minute. Good agreement was observed between alignment measurements from MRI and weight-bearing radiographs. This technique offers a sub-one-minute scan that can be incorporated into routine MRI knee scans to add important knee alignment information and potentially removes the need for additional scanning.
Introduction
Varus and valgus alignment are associated with the presence and progression of knee osteoarthritis (1). Knee alignment is most commonly assessed with a weight-bearing full-lower-limb radiograph. However, there is concern about the radiation of these exams to the pelvic regions. Further, there is increasing application of MRI to studying OA in research and clinical settings (2,3). In this work, we develop and assess a rapid method to assess leg alignment on MRI that can be incorporated into all knee MRI exams.Materials and Methods
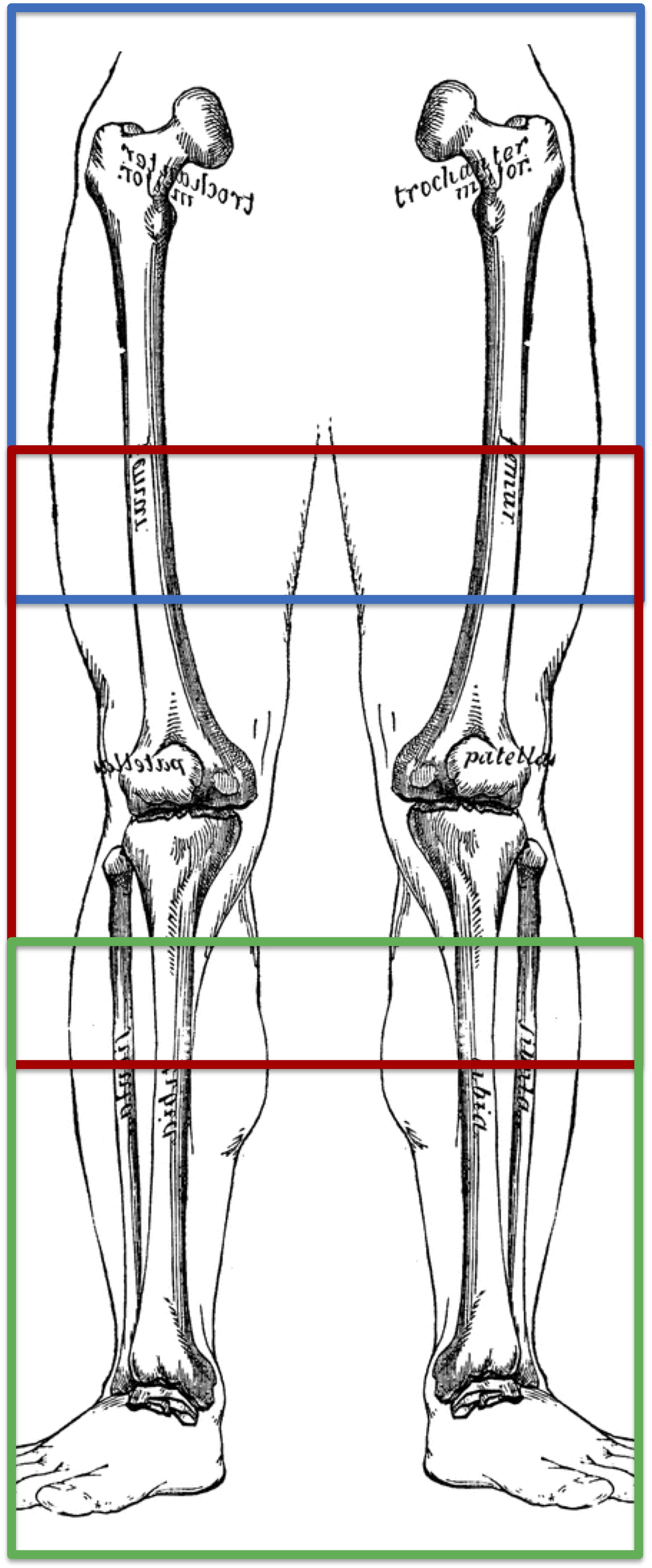
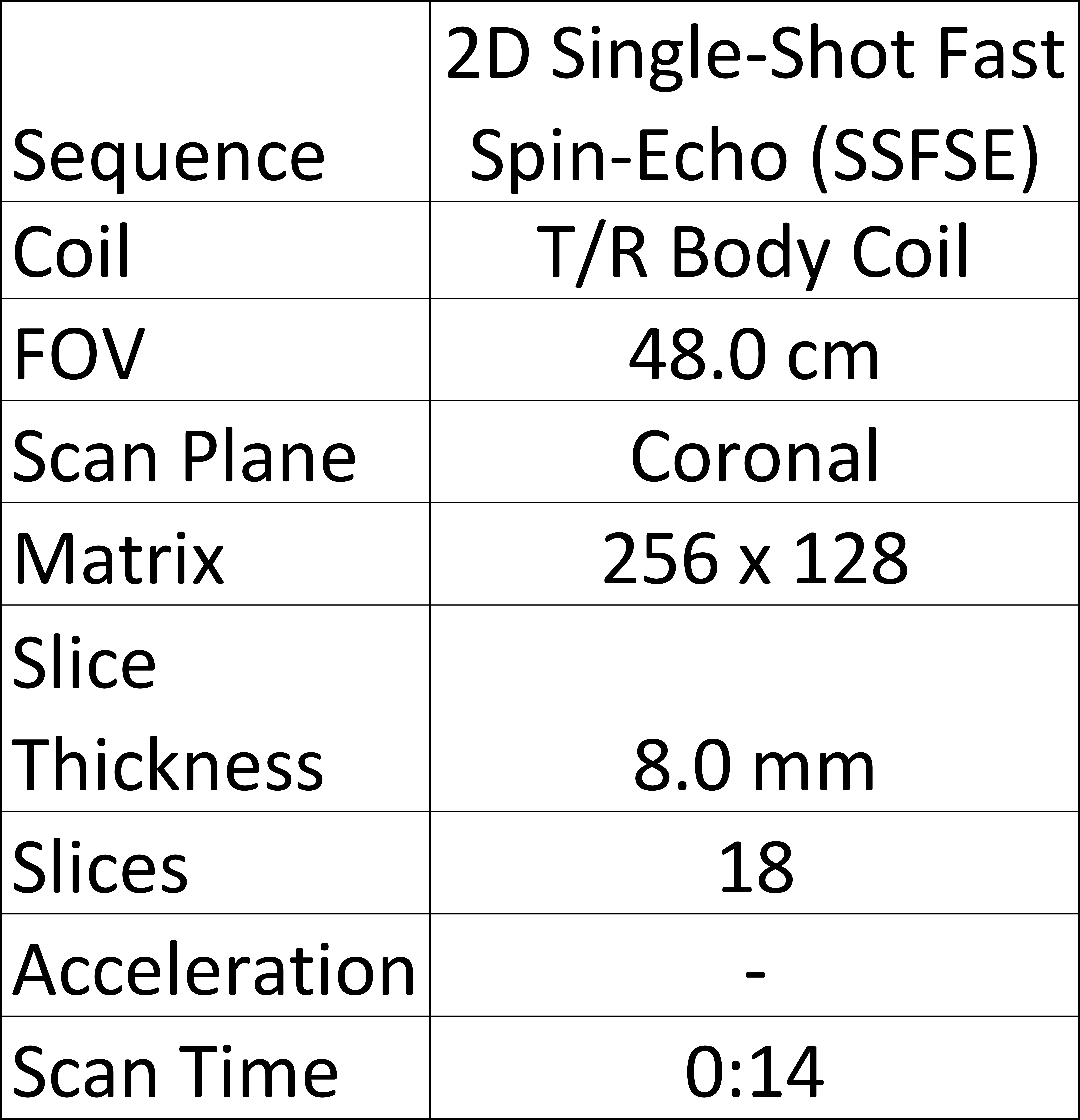
Ten patients underwent a weight-bearing whole-leg radiograph as well as a unilateral knee MRI on a 3T whole-body scanner. While single-knee scanning was performed with a dedicated 16-channel receive-only flexible phased-array coil, whole-leg MRI was performed with a 3-station single-shot fast spin-echo (SSFSE) sequence using the scanner transmit/receive body coil (Fig. 1) and the imaging parameters listed in Table 1. For each station, maximum-intensity projections of the bone were created around the anatomical points of interest and stitched together to create whole-leg projections (Fig. 2). On radiographs and MRI, alignment was measured as the angle from the center of the femoral head to the midpoint of the tibial plateau to the midpoint of line from the lateral fibula to the medial tibia at the height of the tibial plafond (Fig. 3). Differences between measures were assessed by Bland-Altman analysis and concordance correlations. Differences between alignment measures in the leg undergoing primary knee MRI scans and the contralateral leg were assessed with a Wilcoxon rank-sum test.Results
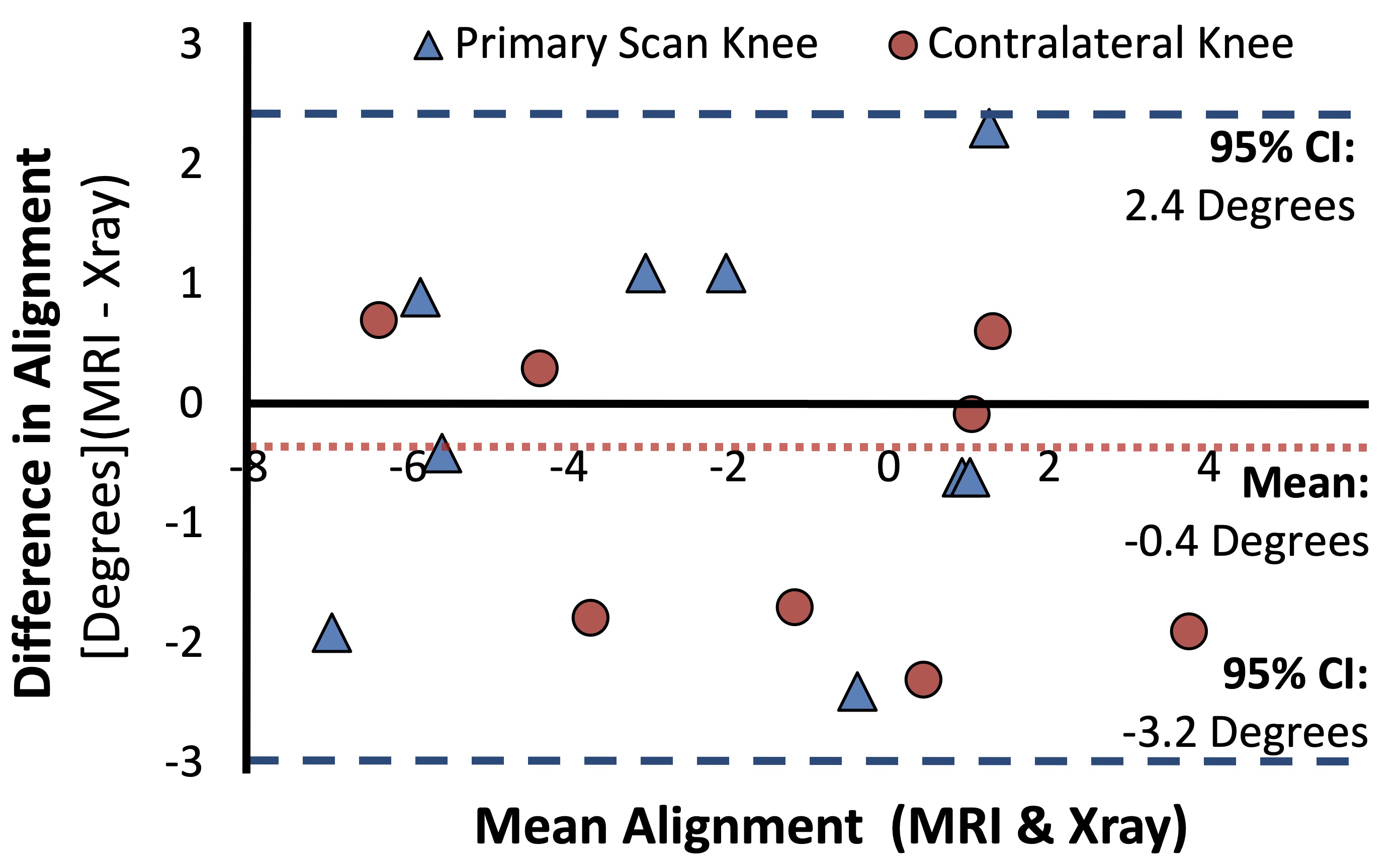
In total 17 whole-leg MRI projections were included for analysis. One subject was excluded due to laxity in his knees while the left leg of another subject was excluded due to a hip implant which made localization of the femoral head impossible on MRI. The mean difference in alignment between MRI and radiograph measurements was -0.4±1.4 degrees (95% Limits of Agreement: -3.2 to 2.4 degrees) [0.4 degrees more varus] with a high concordance correlation of 0.91 (p<0.001) (Fig. 4). No statistical difference was observed between the MRI differences in alignment (from radiographs) between the leg undergoing primary knee MRI scans and the contralateral leg (p=0.81). Additionally, no correlation was observed between differences in alignment measurements (between MRI and radiographs) and the degree of varus or valgus alignment (R = -.12, p = 0.64). Three station scanning was performed in 45-60 seconds including table movement and prescan.Discussion
MRI alignment scans can replace the typical localizer for the individual clinical and quantitative knee MRI that is conventionally performed (usually on the order of 20-45 seconds). It is very important to note that MRI scanning in our study was not under load while radiographs are performed in a weight-bearing position. Nevertheless, the high correlation and narrow limits of agreement between MRI and radiograph measures suggest that that unloaded MRI assessment can be used to approximate measures of knee alignment, with minimal scan time. There was no correlation between the difference in MRI and radiograph alignment measures and the knee alignment suggesting minimal bias from MRI measures. Further, similar measurement differences were observed in the leg undergoing a knee MRI, which is consistently positioned with a straight knee in the flexible MRI coil and foot positioned at a constant angle on a base board, and the contralateral leg for which positioning was not controlled. This suggests that this technique is relatively robust to positioning.Conclusion
We presented a new method for rapid measurement of knee alignment on MRI which showed good agreement with radiographic measures. This technique can easily be incorporated as a localizer into routine MRI knee scans to add important knee alignment information and remove the need for additional scanning.Acknowledgements
We receive research support from GE Healthcare and NIH Grants R00EB022634, R01EB002524, R01AR0063643, and K24AR062068.References
[1] Hunter, D. J., Sharma, L. & Skaife, T. Alignment and osteoarthritis of the knee. J Bone Joint Surg Am 91 Suppl 1, 85-89, doi:10.2106/JBJS.H.01409 (2009).
[2] Li, Q., Amano, K., Link, T. M. & Ma, C. B. Advanced Imaging in Osteoarthritis. Sports Health 8, 418-428, doi:10.1177/1941738116663922 (2016).
[3] Roemer, F. W., Eckstein, F., Hayashi, D. & Guermazi, A. The role of imaging in osteoarthritis. Best Pract Res Clin Rheumatol 28, 31-60, doi:10.1016/j.berh.2014.02.002 (2014).
Figures