2826
INCREASED PREVALENCE OF FEMOROACETABULAR IMPINGEMENT ANATOMY AMONG ATHLETES WHO TREAD WATER1Radiology, Stanford University, Stanford, CA, United States, 2Cambridge University, Cambridge, United Kingdom, 3Stanford University, Stanford, CA, United States
Synopsis
Femoroacetabular impingement (FAI) is a disorder that causes hip pain and disability in young patients, particularly athletes. Treading water leads to increased stress on the hip, the effects of which are poorly understood. In this study, we used MRI to identify the prevalence of FAI anatomy in elite aquatic athletes that tread water. The prevalence of cam FAI was higher than that previously reported for any other sport. This study demonstrates that synchronized swimmers and water polo athletes are at increased risk of cam FAI, more than other sports.
INTRODUCTION
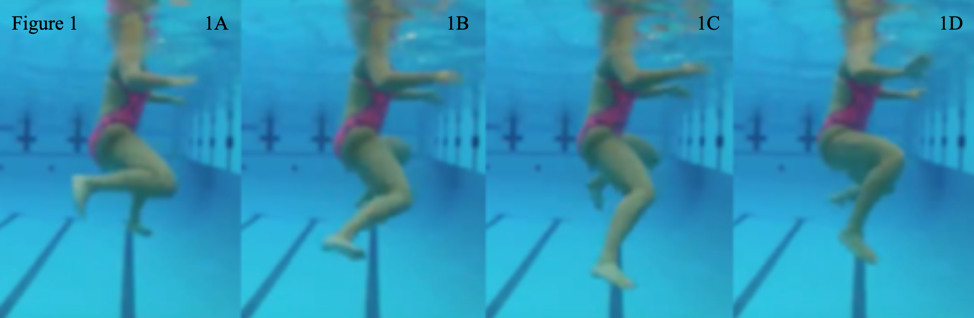
Femoroacetabular impingement (FAI) is a disorder that causes hip pain and disability in young patients, particularly athletes, and may lead to eventual hip osteoarthritis [1][2]. Increased stress on the hip due to continued rotational motion, like the egg-beater kick done while treading water, could put an individual at risk of FAI anatomy. Water polo and synchronized swimming require extensive egg-beater kicking to effectively participate in these activities (Figure 1A-1D). The goal of this study was to use MR imaging to identify whether athletes who tread water have an increased prevalence of FAI anatomy.METHODS
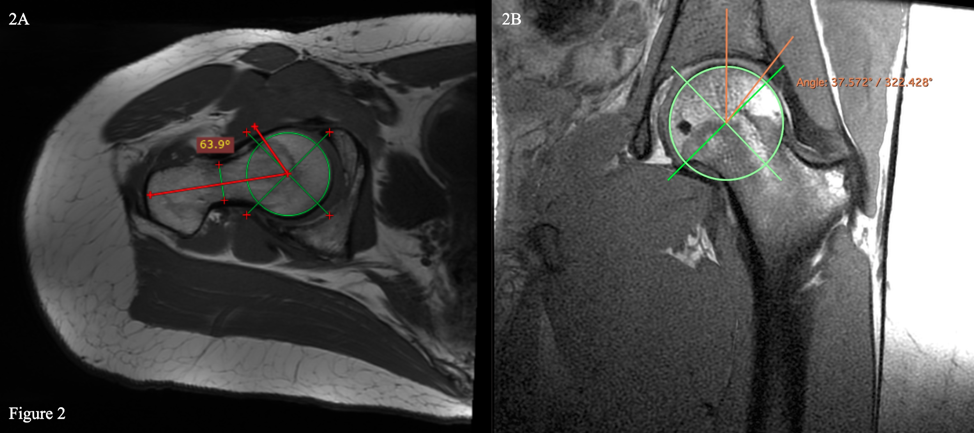
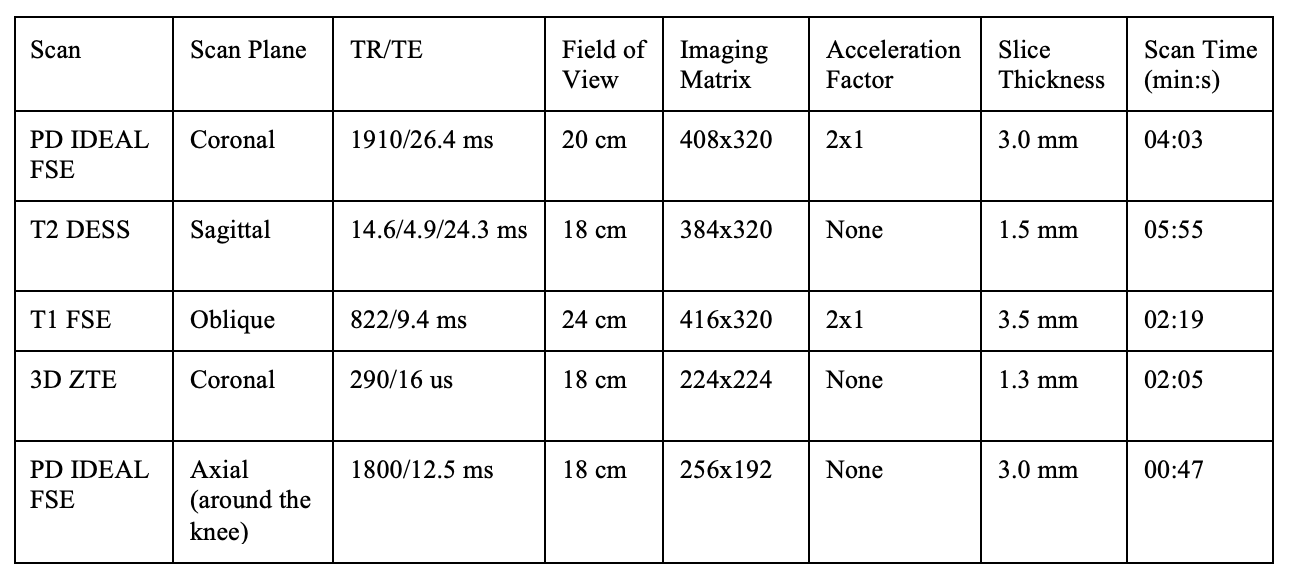
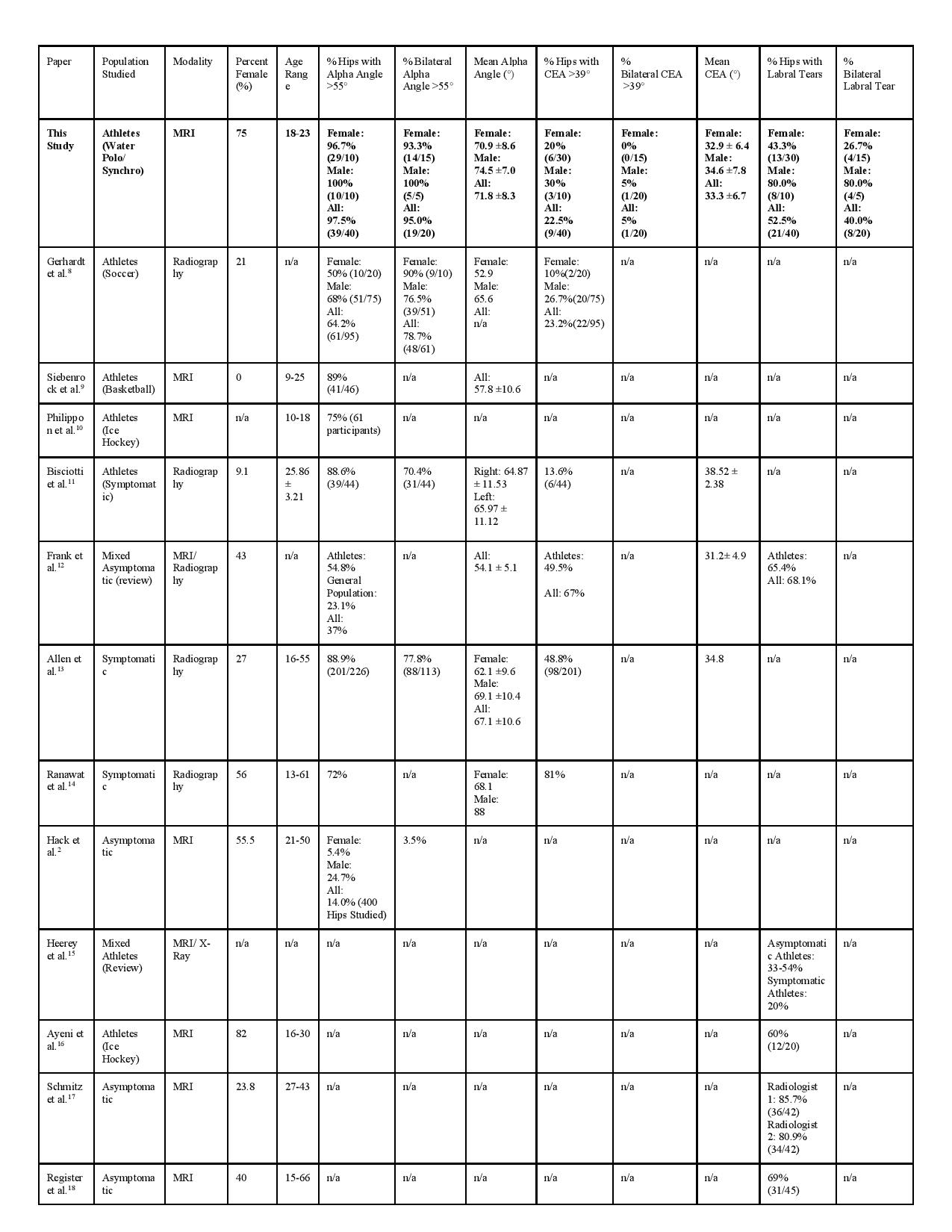
20 NCAA Division 1 varsity water polo players and synchronized swimmers (15 female, 5 male), ages 18-23 (mean 20.7 ± 1.4), underwent non-contrast MRI scans of both hips using a whole-body 3T MRI scanner (GE Healthcare) with a large, 16 channel flexible phased-array-receive-only coil (Table 1). The presence of abnormal cam/pincer anatomy and labral tears were identified. An oblique T1 FSE sequence was used to evaluate the alpha angle for cam identification. A coronal 3D ZTE image was fused with a water-only coronal PD IDEAL FSE image to evaluate the lateral center edge angle (CEA) for pincer identification. Alpha angles greater than 55° and CEA greater than 39° were considered abnormal [3][4][5]. RadiAnt DICOM viewer software was used for all angles (Figure 2). Labral tears were identified by an experienced musculoskeletal radiologist. These were scored using the Scoring Hip Osteoarthritis Using MRI (SHOMRI) semiquantitative grading scale [6]. Participants completed the 33-item International Hip Outcome Tool (iHOT-33) which is a patient-reported measure designed to evaluate hip-related quality of life [7]. Correlations were calculated between the angles and the estimated number of lifetime hours participants treaded water. A correlation was also done between iHOT-33 and SHOMRI. A Wilcoxon Rank Sum Test was used to compare the different groups split by sport, gender, and symptoms to look for differences in alpha angles, CEA, and iHOT-33 scores. The prevalence of FAI anatomy in this cohort was compared to published research on asymptomatic, symptomatic, and athletic cohorts.RESULTS
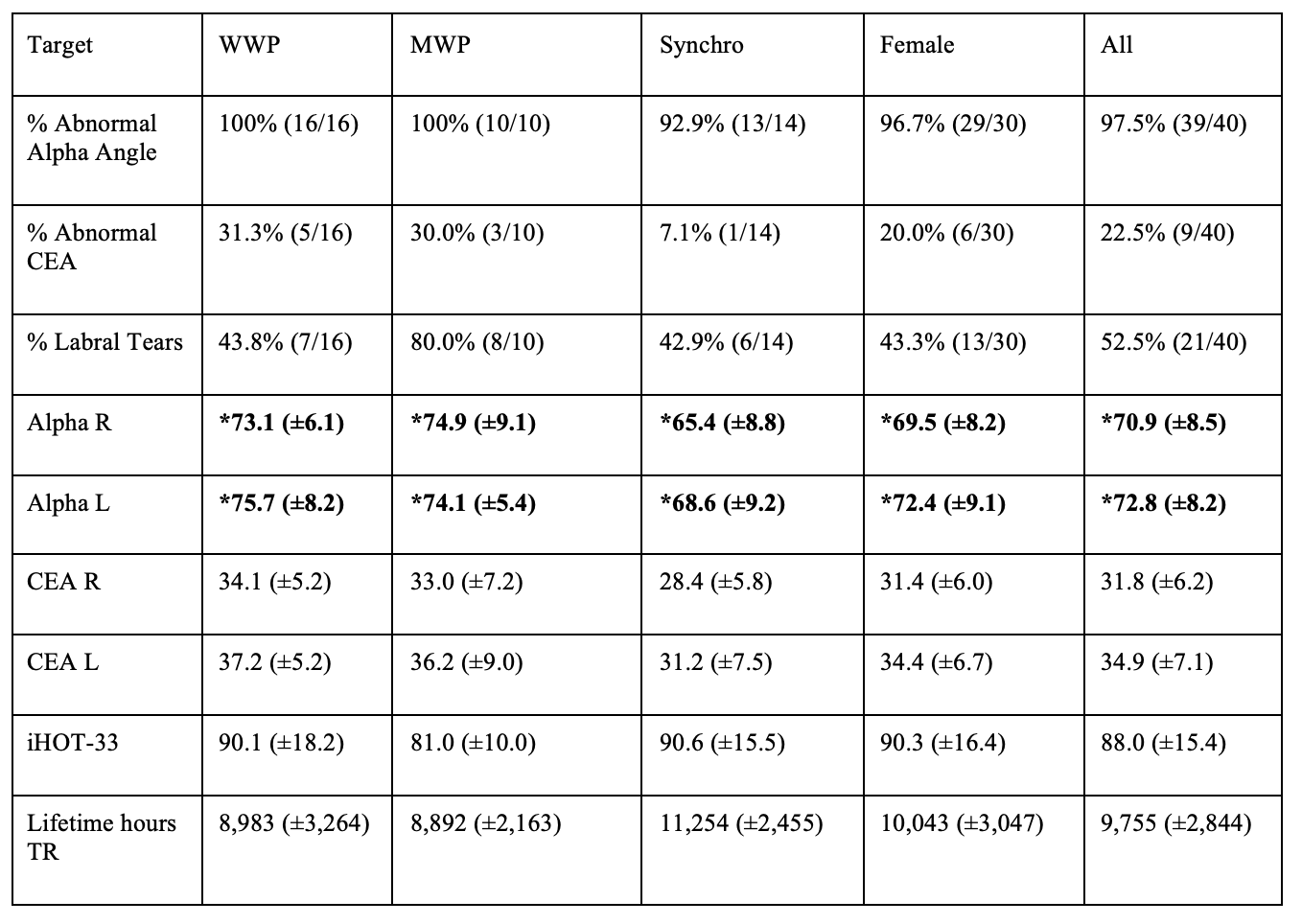
In our subjects, 70% (14/20) reported having pain in their hips yet only 15% (3/20) sought evaluation or treatment for hip pain. Cam deformity was identified in 97.5% (39/40) of hips while 22.5% (9/40) demonstrated pincer deformity. Additionally, 53% (21/40) of hips had evidence of a labral tear. Every participant had at least 1 hip with FAI anatomy (Table 2). This study found a higher prevalence of cam FAI anatomy in water polo players and synchronized swimmers compared to prior studies of athletes (Table 3). These trends were not seen for CEA or labral tears. No statistically significant differences between sport or gender was found on the basis of angles, iHOT-33, or labral tears. The exception is for iHOT-33 scores where there was a statistically significant difference for male versus female (p=0.043), with males having a mean value of 81.0 (±10.0) and females having a mean value of 90.3 (±16.4). No observed correlations were found between treading water and the measured outcomes. The correlation between iHOT-33 scores and SHOMRI (r=0.008) was not significant (p=0.963).DISCUSSION
Water polo players and synchronized swimmers have a high prevalence of cam FAI anatomy, indicating that treading water may be a risk factor for cam FAI. Cam FAI is often thought to be the result of abnormal forces on the femoral head physis, and this study would suggest that rotational forces associated with treading water may be the cause, as there is no ground contact in these sports. Pincer FAI and labral pathology were not greater than the prevalence reported for other athletes in other sports. We did not find a correlation with lifetime hours of treading water and measurements of FAI, though more detailed analysis of larger numbers of athletes may still be warranted. As would be expected, athletes who reported hip symptoms had a statistically significantly lower iHOT-33 score than the asymptomatic group. This validates the use of the iHOT-33 as being able to distinguish between symptomatic and asymptomatic hips. However, iHOT-33 scores were not correlated with SHOMRI scores, indicating that structural changes as seen on MRI may not correlate well with patient symptoms, but requires further analysis.CONCLUSION
This study demonstrates that synchronized swimmers and water polo athletes are at increased risk of cam FAI, more than other sports. Further, this study sheds some more light on the etiology of cam FAI, which contributes to our understanding of the development of FAI and the development of preventative treatments.Acknowledgements
The authors would like to thank the Stanford Athletics varsity water polo and synchronized swimming teams and coaches for allowing us to use them as subjects. This work was supported by a Major Grant from the Stanford University Vice Provost for Undergraduate Education as part of the Human Biology Honors Program. Research support also came from GE Healthcare, and grants NIH EB002524 and NIH AR06206.References
[1] Byrd, JW. Femoroacetabular impingement in athletes, part 1: cause and assessment. Sports Health. 2010; 2 (4): 321-333, doi:10.1177/1941738110368392. PMID: 23015955
[2] Hack, K, Di Primio, G, Rakhra, K & Beaulé, PE. Prevalence of cam-type femoroacetabular impingement morphology in asymptomatic volunteers. J Bone Joint Surg Am. 2010; 92 (14): 2436-2444, doi:10.2106/JBJS.J.01280. PMID: 20962194
[3] Fiorentino, G, Fontanarosa, A, Cepparulo, R et al. Treatment of cam-type femoroacetabular impingement. Joints. 2015; 3 (2): 67-71, doi:10.11138/jts/2015.3.2.067. PMID: 26605253
[4] Riley, GM, McWalter, EJ, Stevens, KJ et al. MRI of the hip for the evaluation of femoroacetabular impingement; past, present, and future. J Magn Reson Imaging. 2015; 41 (3): 558-572, doi:10.1002/jmri.24725. PMID: 25155435
[5] Wiberg, G. Studies on dysplastic acetabula and congenital subluxation of the hip joint: with special reference to the complication of osteoarthritis. Acta Orthop Scand. 1939; 83 1-135.
[6] Lee, S, Nardo, L, Kumar, D et al. Scoring hip osteoarthritis with MRI (SHOMRI): A whole joint osteoarthritis evaluation system. J Magn Reson Imaging. 2015; 41 (6): 1549-1557, doi:10.1002/jmri.24722. PMID: 25139720
[7] Mohtadi, NG, Griffin, DR, Pedersen, ME et al. The Development and validation of a self-administered quality-of-life outcome measure for young, active patients with symptomatic hip disease: the International Hip Outcome Tool (iHOT-33). Arthroscopy. 2012; 28 (5): 595-605; quiz 606-510.e591, doi:10.1016/j.arthro.2012.03.013. PMID: 22542433
[8] Gerhardt, MB, Romero, AA, Silvers, HJ et al. The prevalence of radiographic hip abnormalities in elite soccer players. Am J Sports Med. 2012; 40 (3): 584-588, doi:10.1177/0363546511432711. PMID: 22343678
[9] Siebenrock, KA, Ferner, F, Noble, PC et al. The cam-type deformity of the proximal femur arises in childhood in response to vigorous sporting activity. Clin Orthop Relat Res. 2011; 469 (11): 3229-3240, doi:10.1007/s11999-011-1945-4. PMID: 21761254
[10] Philippon, MJ, Ho, CP, Briggs, KK, Stull, J & LaPrade, RF. Prevalence of increased alpha angles as a measure of cam-type femoroacetabular impingement in youth ice hockey players. Am J Sports Med. 2013; 41 (6): 1357-1362, doi:10.1177/0363546513483448. PMID: 23562808
[11] Bisciotti, GN, Di Marzo, F, Auci, A et al. Cam morphology and inguinal pathologies: is there a possible connection? J Orthop Traumatol. 2017; 18 (4): 439-450, doi:10.1007/s10195-017-0470-y. PMID: 28921307
[12] Frank, JM, Harris, JD, Erickson, BJ et al. Prevalence of Femoroacetabular Impingement Imaging Findings in Asymptomatic Volunteers: A Systematic Review. Arthroscopy. 2015; 31 (6): 1199-1204, doi:10.1016/j.arthro.2014.11.042. PMID: 25636988
[13] Allen, D, Beaulé, PE, Ramadan, O & Doucette, S. Prevalence of associated deformities and hip pain in patients with cam-type femoroacetabular impingement. J Bone Joint Surg Br. 2009; 91 (5): 589-594, doi:10.1302/0301-620X.91B5.22028. PMID: 19407290
[14] Ranawat, AS, Schulz, B, Baumbach, SF et al. Radiographic predictors of hip pain in femoroacetabular impingement. HSS J. 2011; 7 (2): 115-119, doi:10.1007/s11420-010-9192-x. PMID: 22754409
[15] Heerey, JJ, Kemp, JL, Mosler, AB et al. What is the Prevalence of Hip Intra-Articular Pathologies and Osteoarthritis in Active Athletes with Hip and Groin Pain Compared with Those Without? A Systematic Review and Meta-Analysis. Sports Med. 2019; 49 (6): 951-972, doi:10.1007/s40279-019-01092-y. PMID: 30972659
[16] Ayeni, OR, Banga, K, Bhandari, M et al. Femoroacetabular impingement in elite ice hockey players. Knee Surg Sports Traumatol Arthrosc. 2014; 22 (4): 920-925, doi:10.1007/s00167-013-2598-5. PMID: 23842802
[17] Schmitz, MR, Campbell, SE, Fajardo, RS & Kadrmas, WR. Identification of acetabular labral pathological changes in asymptomatic volunteers using optimized, noncontrast 1.5-T magnetic resonance imaging. Am J Sports Med. 2012; 40 (6): 1337-1341, doi:10.1177/0363546512439991. PMID: 22422932
[18] Register, B, Pennock, AT, Ho, CP et al. Prevalence of abnormal hip findings in asymptomatic participants: a prospective, blinded study. Am J Sports Med. 2012; 40 (12): 2720-2724, doi:10.1177/0363546512462124. PMID: 23104610
Figures