2825
Real-time Imaging of the TMJ: Comparison of Methods1Department of Internal Medicine II, University Medical Center Ulm, Ulm, Germany
Synopsis
Disorders of the temporomandibular joint (TMJ), such as pain and blockage, usually arise while the joint is in motion. Capturing this dynamic process requires high temporal resolutions and good contrast between condyle and articular disk, which is possible with advanced sequences that often need sophisticated reconstruction algorithms. In this contribution, the widely available or easily implemented and reconstructed TSE-Zoom sequence was compared to advanced radial and spiral sequences employing uniform and tiny golden angle(tyGA) profile ordering. While tyGA sequences allow fluid rendering of the joint motion, TSE-Zoom can be considered a viable alternative with excellent contrast between condyle and disk.
Introduction
Static MR images of the mouth in opened and closed positions are a conventional approach for the diagnoses of disorders of the temporomandibular joint (TMJ)1. However, pain and blockage in the joint usually arises while the TMJ is in motion2, e.g. during chewing or speaking. Capturing this dynamic process with MRI is challenging, since it requires high temporal resolutions to visualize the course of motion of the joint with good contrast between the condyle and the articular disk. Furthermore, the advanced sequences, especially in combination with sophisticated reconstruction algorithms, are not readily available on clinical systems. The TSE-Zoom sequence3 is, if not already available for the scanner, easy to implement and due to its use of Cartesian k-space sampling requires merely a Fourier transform for image reconstruction. For this contribution, we compared a single-shot TSE-Zoom sequence to radial and spiral balanced sequences for dynamic in vivo imaging of the TMJ.Methods
TSE-Zoom applies slice selection gradients during the refocusing pulses on an axis perpendicular to the selection gradients for the excitation pulse, thus reducing the FOV in one direction. Choosing the same direction for phase encoding a single-shot TSE image can be acquired within a few hundred milliseconds4, dependent on the flip angles and SAR limitations. For dynamic TMJ imaging the FOV was reduced from 192 mm to 48 mm in anterior-posterior direction, just ensuring the visibility of the condyle during the entire range of motion of the jaw. With excitation and refocusing flip angles of 90°-180° a temporal resolution of 600 ms could be achieved. Lowering the refocusing angle to 160° allowed the image acquisition in 300 ms. Further reduction of the flip angles made the identification of the condyle impossible due to low SNR. Balanced radial and spiral sequences with uniform and tiny golden angle5 (tyGA) profile ordering were chosen for comparison. For tyGA sequences an angular increment of $$$\psi_7$$$ = 23.6281° was used, while profile angles for the uniform ordering scheme were adapted to match the temporal resolutions of TSE-Zoom. Relevant imaging parameters are listed in Table 1.All data were acquired with a 1.5T whole-body clinical imaging system (Achieva, Philips Healthcare, The Netherlands) using a four-element dental surface coil (NORAS, Hoechberg, Germany). In vivo scans of the left and right TMJ were acquired from six volunteers after obtaining written informed consent. Each scan had a duration of 25 s during which the volunteers moved their jaws at two different speeds, a slow motion for opening and closing lasting 10 s each and a faster motion with 4 s duration.
The contrast ratio between condyle and articular disk was calculated according to $$$r_c = (I_c - I_d)/I_c$$$ , with $$$I_c$$$ and $$$I_d$$$ being the signal intensities in ROIs of the condyle and disk, respectively.
Results
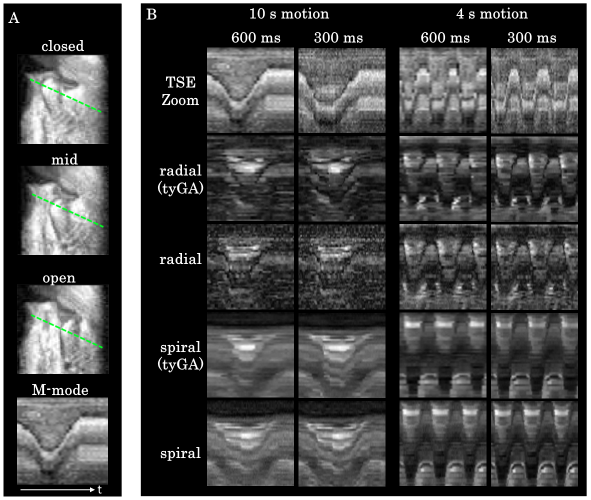
Fig. 1 shows images acquired in one volunteer with the TMJ in closed position for all sequences and temporal resolutions. All sequences successfully acquired images of TMJ structures that appear slightly blurred in the spiral images and sharpest for the TSE-Zoom sequences. While an increase in temporal resolution leads to an overall reduction in SNR, this is especially noticeable in the TSE-Zoom images.Fig. 2 depicts the TMJ during maximal condyle movement. While the condyle head remains sharp through all motion phases for tyGA radial and TSE-Zoom images, blurring occurs in the spiral images and to a lesser extend for the uniform radial sequences. The disk is clearly discernible in tyGA radial, spiral and TSE-Zoom images for slow and fast TMJ motions.
Fig. 3A displays the TMJ in closed, middle and open position and an M-mode plot of a profile through the moving condyle head (green striped line) for assessment of motion fluidity. M-mode plots for all sequences, motion speeds and temporal resolutions are shown in Fig. 3B. Although all sequences benefit from a higher temporal resolution, the tyGA sequences achieve an almost continuous depiction of the joint motion.
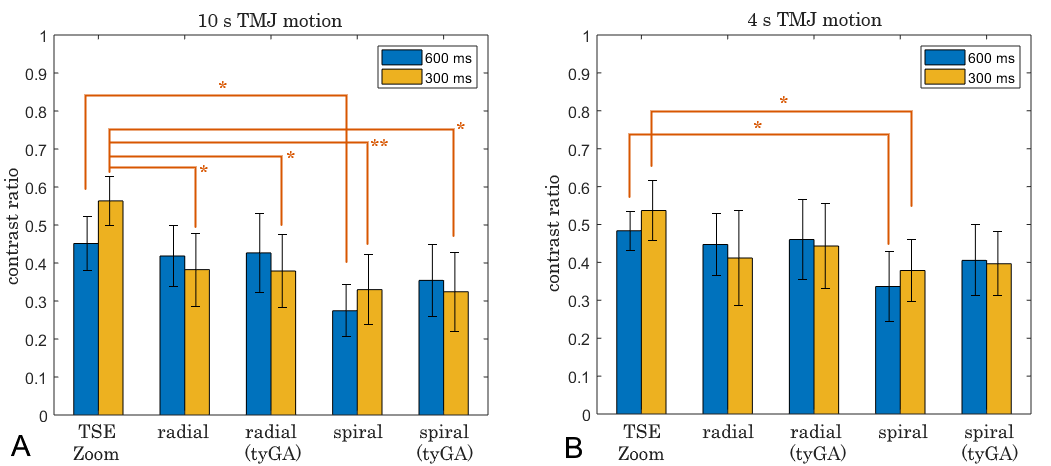
Contrast ratios calculated for slow and fast movements are depicted in Fig. 4 A and B. Overall strongest contrast between condyle head and disk was calculated for TSE-Zoom. For the faster 4 second jaw motion (B) the differences in contrast ratios between the sequences is smaller, with uniform spiral images displaying the overall lowest contrast ratio.
Discussion and Conclusion
The TSE-Zoom sequence allows for a sharp depiction of the condyle head for slow and fast jaw motions, since the actual images are acquired within 100 ms, whereas the longer repetition times of 300 and 600 ms, required due to SAR limitations, may cause an uneven visualization of the motion. The apparent motion with the uniform radial and spiral sequences appear smooth with some residual blurring since data is acquired over the entire 300 / 600 ms. Completely smooth depictions of the TMJ motion is achieved with the tyGA sequences, due to the ideal profile distribution that allows sliding window reconstructions with small step sizes.In conclusion, the TSE-Zoom sequence appears as attractive alternative to more sophisticated techniques especially due to its excellent contrast and availability. Limitations from the non-even motion visualization needs further clinical evaluation.
Acknowledgements
The authors thank the Ulm University Center for Translational Imaging MoMAN for its support.References
[1] Abolmaali ND, Schmitt J, Schwarz W, et al. Visualization of the articular disk of the temporomandibular joint in near-real-time MRI: feasibility study. Eur Radiol. 2004;14:1889–1894
[2] Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the international RDC/TMD consortium network and orofacial pain special interest group. J Oral Facial Pain Headache 2014; 28: 6–27.
[3] Feinberg DA, Hoenninger JC, Crooks LE, Kaufman L, Watts JC, Arakawa M. Inner volume MR imaging: technical concepts and their application. Radiology. 1985;156(3):743–747.
[4] Beer M, Held P, Leibrock A, Fellner C, Handel G. Diagnostic potential of pseudo-dynamic MRI (CINE mode) for evaluation of internal derangement of the TMJ. Eur J Radiol 1996; 23: 212–5.
[5] Wundrak S, Paul J, Ulrici J, Hell E, Rasche V. A small surrogate for the golden angle in time-resolved radial MRI based on generalized fibonacci sequences. IEEE Trans Med Imaging 2014;34.
Figures