2804
High-resolution 3T MRI of the dorsal and volar radioulnar ligament of the wrist1Department of radiological sciences, University of California, Irvine, Irvine, CA, United States, 2Radiology Department, St. Luke's International Hospital, Tokyo, Japan
Synopsis
It is technically challenging to diagnose injuries to the radioulnar ligaments (RUL) of the wrist on magnetic resonance imaging (MRI). We identified and classified the morphology of the dorsal and volar radioulnar ligaments (RUL) of the wrist into five types using 3T MRI. Two hundred and nine participants were retrospectively evaluated using 3T axial 2D and reformatted axial isotropic 3D images. Both dorsal and volar RULs attach to the radial to dorsal side of the ulnar styloid. The RUL was equally identified on high-resolution two-dimensional and on isotropic three-dimensional MRI.
Introduction
- The triangular fibrocartilage complex, which was named by Palmer in 1981,1is known to stabilize the distal radioulnar joint. The triangular fibrocartilage complex has been thought to consist of various components, including the disc proper, ulnar capsule, meniscus homologue, ulnar collateral ligament, ulnocarpal ligaments, tendon floor of the extensor carpi ulnaris tendon, and dorsal and volar radioulnar ligament (RUL).
- In particular, the RUL, which connects the distal radius and ulna, has been thought of as the major stabilizer of the distal radioulnar joint under dynamic loading.2-4 However, it is technically challenging to diagnose injuries to the RUL of the wrist on MRI. Also, the morphology and precise location of the RUL attachment on the styloid process has been unclear.5
- The purpose of this study was to investigate usefulness of high-resolution two-dimensional (2D) and isotropic three-dimensional (3D) magnetic resonance imaging (MRI) for identifying and classifying the ulnar attachment site of the dorsal and volarRUL.
Materials and Methods
- The study protocol was approved by the institutional review board, and all subjects provided written informed consent. Two hundred and seventeen participants (114 male, 103 female; age range, 15-84 years; mean age 45.4) were evaluated retrospectively over a period from January 2012 through September 2018 using 3T axial 2D and reformatted axial isotropic 3D images.
- All MRI images were obtained using an eight-channel wrist coil on a 3 T unit (AchievaTX, Philips Healthcare, Best, Netherlands). Each subject was placed in the supine position with the wrist at the side of the body and the forearm in neutral position. Axial 2D FSE PDWI and reformatted images from coronal three-dimensional (3D) isotropic fast spin echo (FSE) proton density-weighted images (PDWI)-fat suppression (FS) were reviewed for evaluation of this study. Imaging parameters are listed in Table 1. A parallel imaging technique named sensitivity encoding (SENSE) was used in both the 2D and 3D sequences. All 3D images were obtained in combination with the driven equilibrium (DRIVE) technique. Acquisition time was approximately 5 minutes for 3D isotropic MRI images and approximately 2 minutes 30 seconds for 2D FSE sequence.
- A board-certified radiologists with 8 years of clinical experience in musculoskeletal radiology reviewed MRI images using a DICOM viewer (OsiriX, version 3.9.1, 64-bit; OsirixFoundation, Geneva, Switzerland). The course and ulnar styloid attachment site of the RUL were classified into five types as follows: A, the RUL is straight and attaches on the same side of the ulnar styloid; B, the RUL is curved and attaches on the same side of the ulnar styloid; C, the RUL attaches on the radial side of the ulnar styloid; D, the RUL is curved and attaches on the opposite side of the ulnar styloid; E, the RUL is straight and attaches on the opposite side of the ulnar styloid (Figure 1). The distance from the base of the styloid process to dorsal and volar RUL attachment was determined on 2D-Ax PDWI. Slice numbers were counted from the most proximal slice of the styloid process to a slice of volar RUL (a in Figure 2), a slice of dorsal RUL (b in Figure 2), and a slice of the tip of the styloid process ( c in Figure 2). A ratio of b to c (b/c) was defined as length of the dorsal RUL attachment from the ulnar styloid base divided by the styloid process length, and a ratio of a to c (a/c) was defined as length of the volar RUL attachment from the ulnar styloid base divided by the styloid process length.
Results
- Eight cases out of 217 participants were excluded from the analysis. These included 6 participants with severe rheumatoid arthritis and two participants with prior severe fracture.
- Table 2 shows the results of morphological classification of the dorsal and volar RUL. Fifty-nine % of the dorsal RUL and 94% of the volar RUL were identified. Type C was the most common in both dorsal and volar RULs (67% of identified dorsal RUL and 41% of identified volarRUL). Thirty-three percent of the dorsal RUL (Type A, 11%; Type B, 22%) and 59% of the volarRUL (Type D, 20%; Type E, 39%) attached to the dorsal side of the ulnar styloid. RUL attachment to the volarside of the ulnar styloid was not observed.
- Figure 3 shows the number of cases and percentages of each combination of the morphological type of the dorsal and volar RUL. The combination of type C dorsal RUL and type C volarRUL was the most common (19%).
- Mean b/c was 0.69, while mean a/c was 0.45. There was significant difference between these values (p<0.001 with paired T test).
Summery
- We identified and classified ulnar attachment patterns of the dorsal and volar RUL of the wrist using 3T MRI. Ninety-four percent of the volar RUL were identified, while only 59% of the dorsal RUL were identified on MRI.
- All of the identified dorsal and volar RULs attached at the dorsal to radial aspect of the styloid process.
- Mean b/c was larger than mean a/c. Therefore, RUL attachment to the styloid process distributed asymmetrically and the dorsal RUL attaches more distally on the styloid process than the volarRUL.
Acknowledgements
References
- Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist--anatomy and function. J Hand Surg Am. 1981;6:153–162.
- Bain GI, Eng K, Lee YC, McGuire D, Zumstein M. Reconstruction of chronic foveal TFCC tears with an autologous tendon graft. J Wrist Surg. 2015;4:9–14.
- Haugstvedt JR, Berger RA, Nakamura T, Neale P, Berglund L, An KN. Relative contributions of the ulnar attachments of the triangular fibrocartilage complex to the dynamic stability of the distal radioulnar joint. J Hand Surg Am. 2006;31:445–451.
- Nakamura T, Makita A. The proximal ligamentous component of the triangular fibrocartilage complex. J Hand Surg Br. 2000;25:479–486.
- Nakamura T, Yabe Y. Histological anatomy of the triangular fibrocartilage complex of the human wrist. Ann Anat. 2000;182:567–572.
Figures
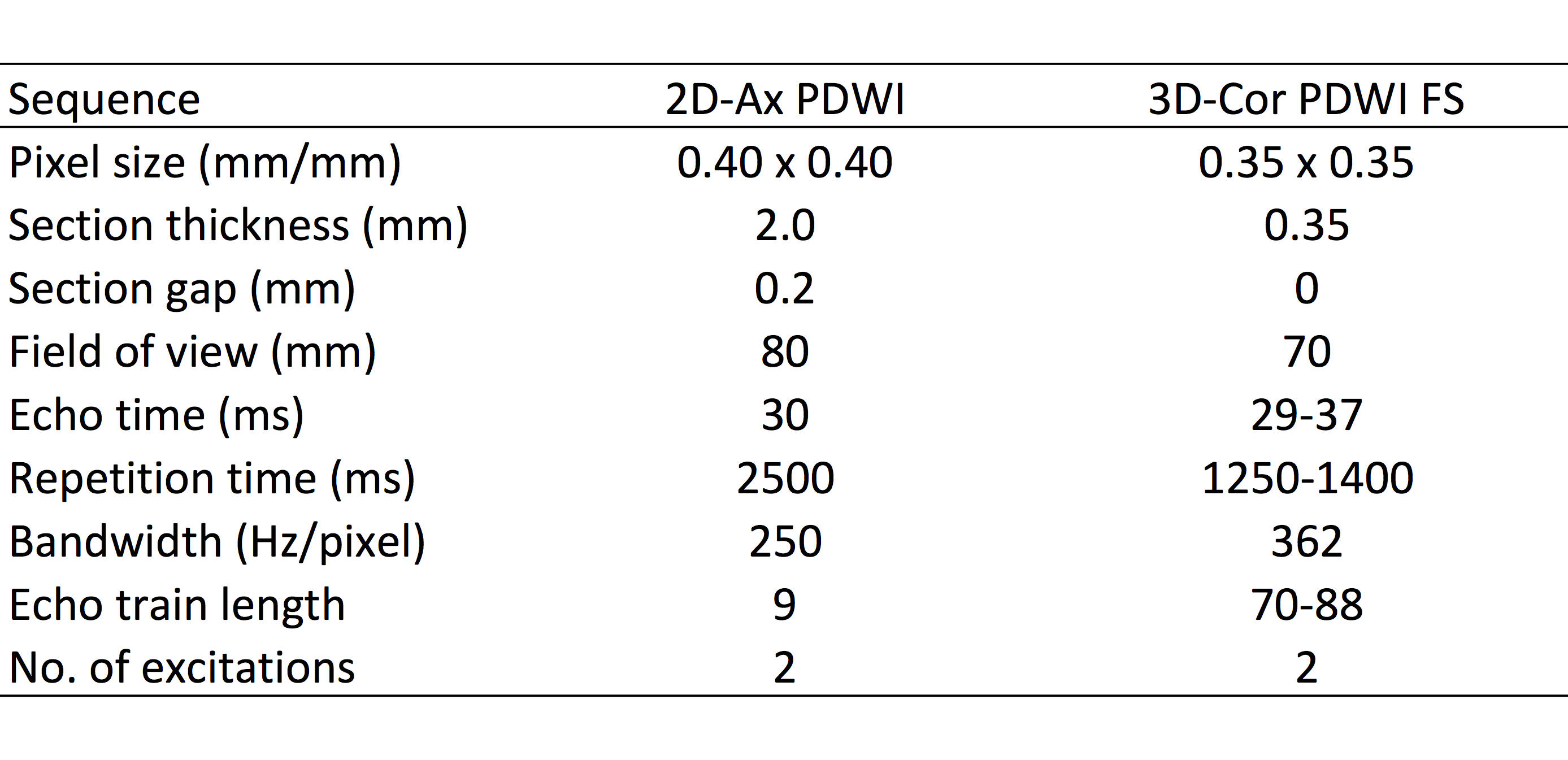
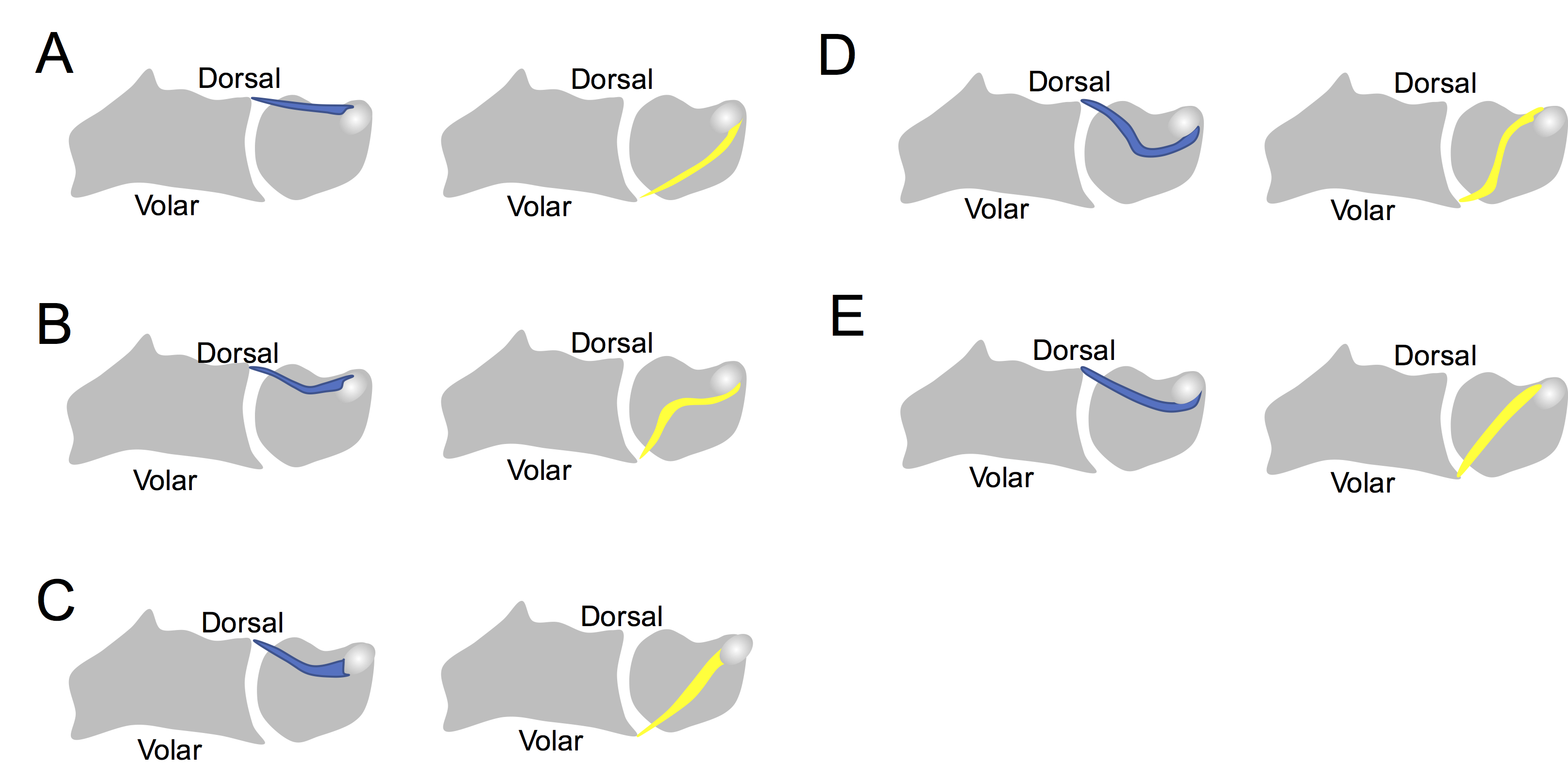
Figure 1. Illustration of the dorsal and volar RUL
The course and the attachment site of the RUL were classified into five types as follows: A, the RUL is straight and attaches on the same side of the ulnar styloid; B, the RUL is curved and attaches on the same side of the ulnar styloid; C, the RUL attaches on the radial side of the ulnar styloid; D, the RUL is curved and attaches on the opposite side of the ulnar styloid; E, the RUL is straight and attaches on the opposite side of the ulnar styloid
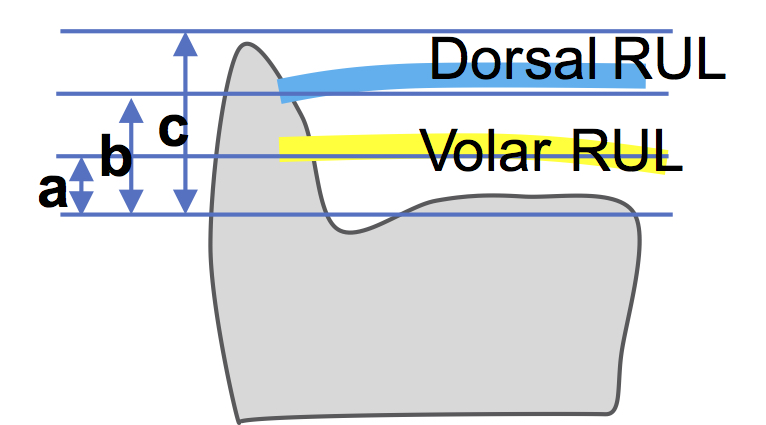
Figure 2. The distance of the dorsal and volar RUL attachment from the base of the styloid process
A ratio of b to c (b/c) was defined as length of the dorsal RUL attachment from the ulnar styloid base divided by the styloid process length, and a ratio of a to c (a/c) was defined as length of the volar RUL attachment from the ulnar styloid base divided by the styloid process length (a, length between the base of the styloid process and volarRUL attachment; b, length between the base of the styloid process and dorsal RUL attachment; c, length between the base and tip of the styloid process.)
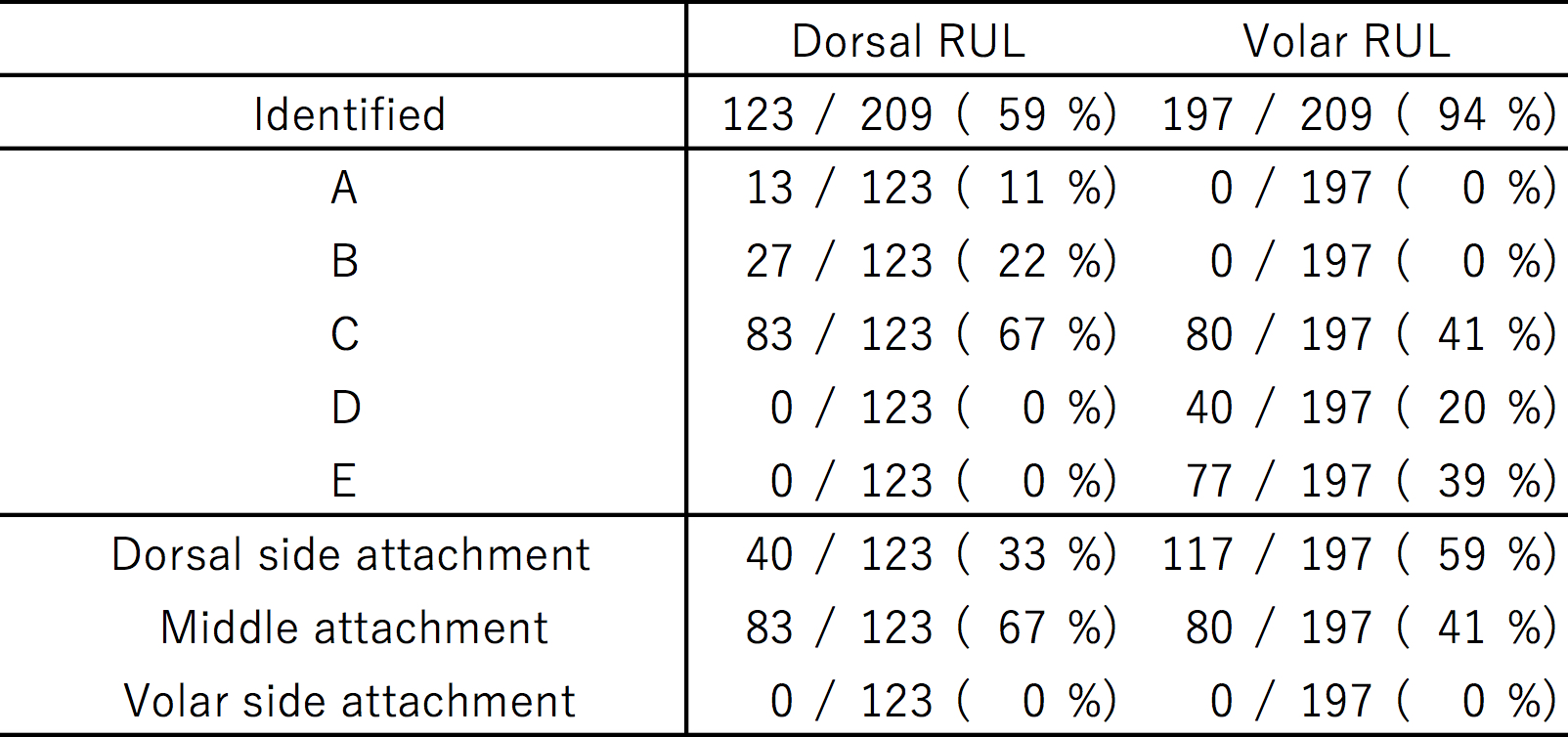
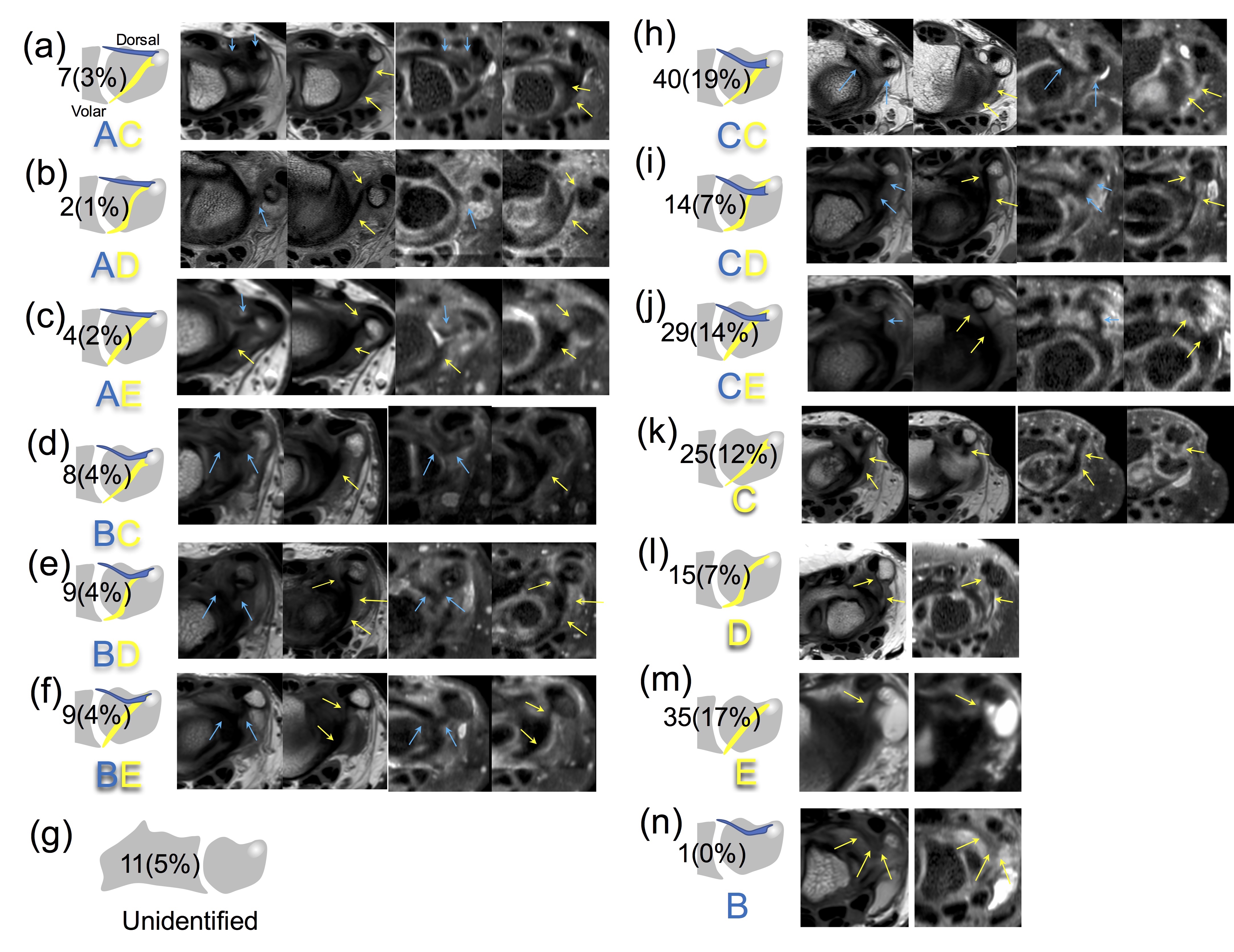
Figure 3. The number of cases and percentage of each combination, and corresponding MRI of the dorsal and volar RUL
The dorsal RULs were not identified in (g), (k), (l) and (m), and the volar RULs were not identified in (g) and (n). Blue arrows on MR images indicates the dorsal RULs, and yellow arrows indicates the volarRULs.