2797
Clinical feasibility of mobile medical screening for wrist injuries in tennis players using a small car-mounted MRI1Institute of Applied Physics, University of Tsukuba, Tsukuba, Japan, 2Graduate School of Human Sciences, University of Tsukuba, Tsukuba, Japan, 3Institute of Clinical Medicine, University of Tsukuba, Tsukuba, Japan
Synopsis
We have developed a portable MRI that can provide opportunities for mobile operation in many environments including screening and primary care suites. Here we showed clinical feasibility of mobile medical screening using the portable MRI. We transported the scanner to a tennis club and imaged the wrists of 21 junior tennis players. The image quality was high enough to detect the TFCC injuries in most cases. Our results indicate that the portable system could be applicable for mass screening and early diagnosis of wrist injuries.
INTRODUCTION
Junior sports players have potential risk for overuse injuries. MRI is capable of detecting early disease of overuse injuries during sport [1], and regular MRI screening is quite useful for injury prevention. However, overuse injury screening on a medical site is impractical, because the number of clinical scanners are limited and most players have less opportunity to have a regular examination for asymptomatic injuries. To address this issue, we have recently developed a small-car mounted, elbow MRI [2-4] that provides opportunities for mobile operation in many environments. Here, we modified the portable system for wrist imaging, and validated the clinical feasibility of mobile screening for wrist injuries in junior tennis players.METHOD
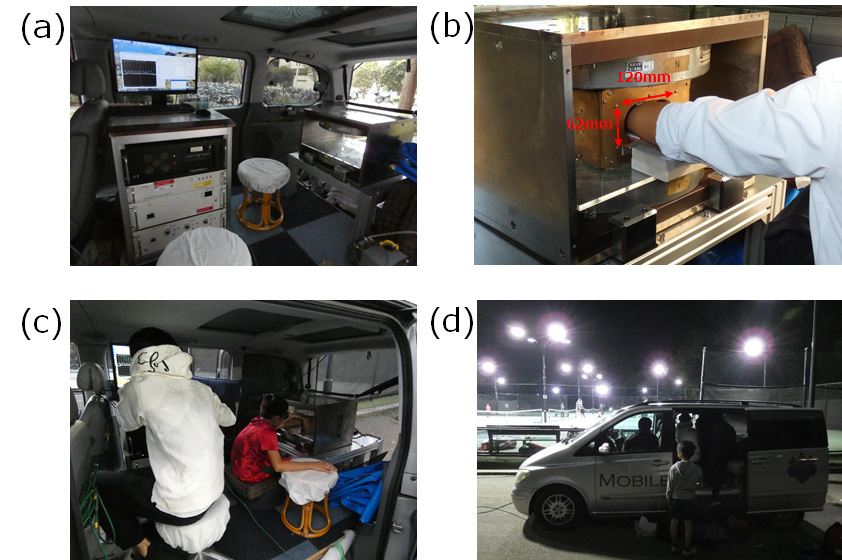
The portable MRI (Fig. 1(a)) consisted of a 0.2 T permanent magnet (NEOMAX Engineering Japan; 200kg; 16cm gap; 44cm×50cm×36cm; 10 cm diameter of spherical volume for imaging), RF probe with shielding, and console (56 cm×77 cm×60 cm). The RF probe (Fig. 1(b)) was newly designed and constructed for wrist imaging with a simplified shielding scheme. The external noise coming into a player’s wrist was shielded using an aluminum plate connecting to the RF shielding box, which reduced setup time for shielding.For a clinical feasibility test, the portable MRI system was transported to a tennis club, and 21 junior tennis players (11 boys and 10 girls; age range = 7-18 years) were examined in six hours. A player sat on a cushion and placed the posterior region of forearm onto the shielding plate. Scout sequences were used to check the positioning in 4 cases, but in the other 17 cases, they were not used to save the examination time.
The coronal and axial images were acquired for the right and left wrists. The sequence used was a multi-slice T2*-weighted gradient echo (TR/TE = 500/18ms; flip angle = 75°, slice thickness = 3mm, matrix size = 256×192, measurement time = 1 min 38 sec per image). The FOV of coronal and axial images were 180×180 mm2 and 126×126 mm2, respectively. The images shown in the figures were trimmed for clear visualization.
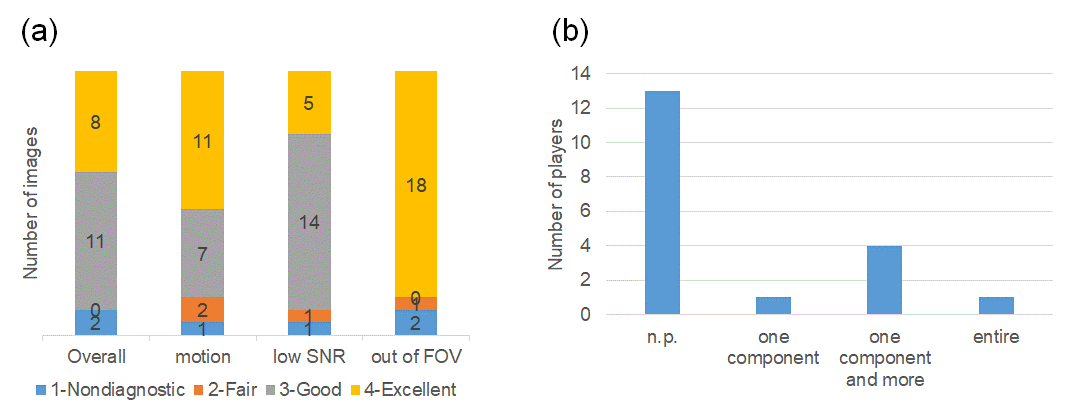
For the clinical evaluation, the MR images were assessed by an MSK radiologist for overall image quality, motion, low SNR, and being out of the FOV on a 4-point scale: 1 = nondiagnostic, 2 = fair, 3 = good, and 4 = excellent. For the images graded as diagnostic (2-4), the radiologist diagnosed the triangular fibrocartilage complex (TFCC) injuries using a four-level grading system: 1 = not particular (n.p.), 2 = one component, 3 = one component or more, 4 = entire.
RESULTS
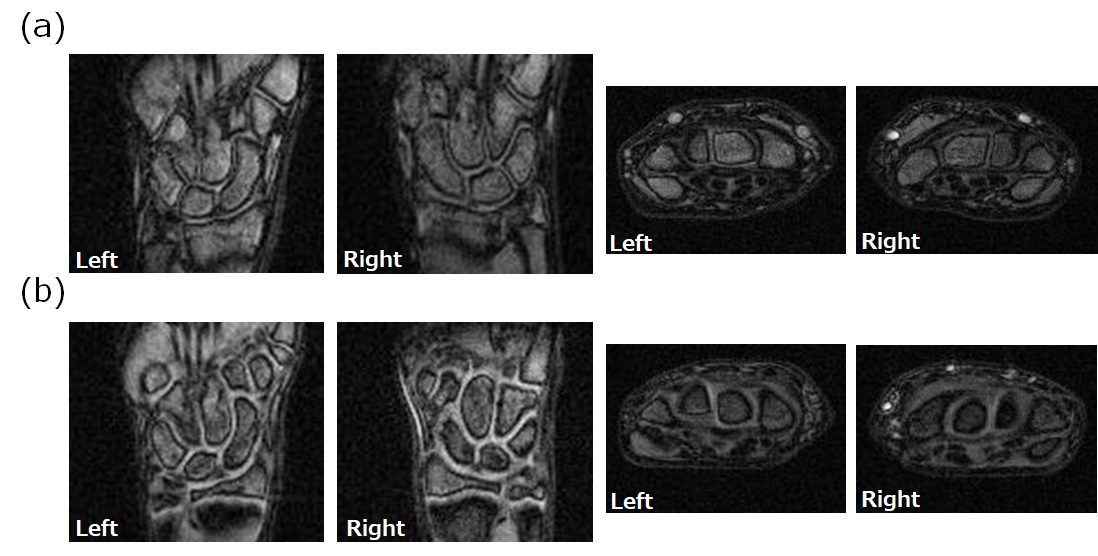
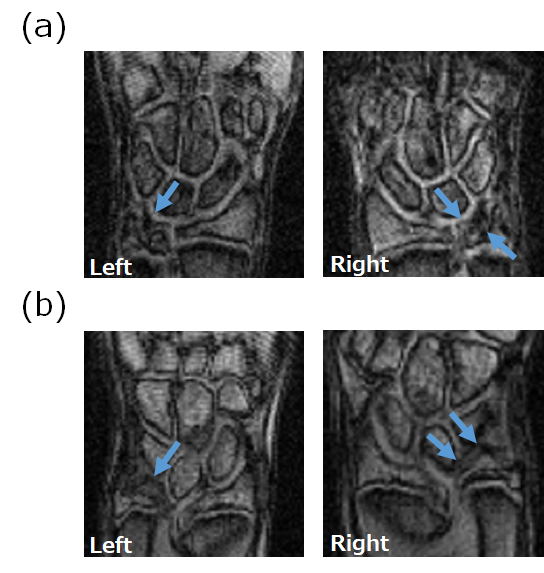
The mean SNR values were 14.1 (axial images for right wrists), 17.4 (coronal images for right wrists), 15.9 (axial images for left wrists), and 17.8 (coronal images for left wrists).Figure 2 shows an example of images graded as excellent quality for diagnosis. Figure 3 shows an example of images with positive findings (assigned as “one component and more” for (a) and “entire” for (b)). The signal intensity was high at two locations in the TFCC in Fig. 3(a) and entirely high in the TFCC in Fig. 3(b).
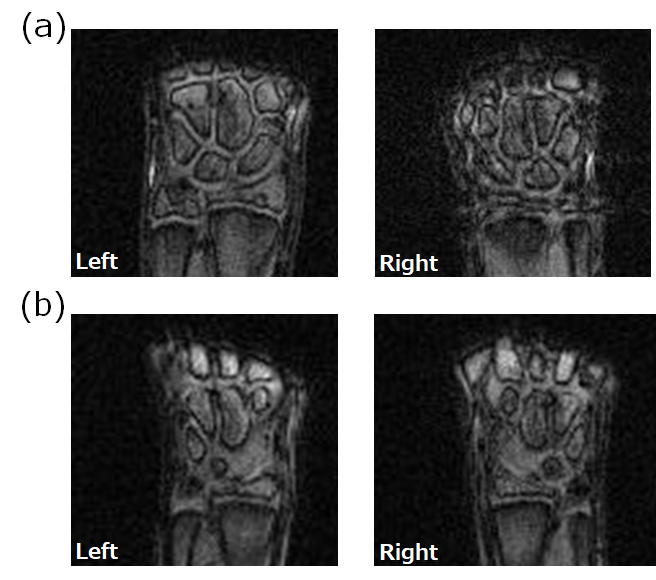
Figure 4 shows the evaluation results. Overall, the number of images with good and excellent quality was 19 out of 21 (90%), and there were only two cases assigned as nondiagnostic (Fig. 4(a)). These images were nondiagnostic because motion and low SNR artifacts appeared and the TFCC regions were out of FOV (Fig. 5). Overall, motion, low SNR, and out-of-FOV artifacts appeared less frequently. Six out of 19 players (32 %) showed positive findings (Fig. 4(b)), which was the unexpectedly high ratio.
DISCUSSION
The examination time was short enough to enable the mobile screening for many players. The image quality was good in most cases, and only two out of 21 cases were nondiagnostic because of motion, low SNR, and being out-of-FOV. In these two cases, the scout sequence was not used and the TFCC region was out of FOV, so that the out-of-FOV artifacts could be improved by using the scout sequence. Many players showed positive findings in this study. This results demonstrated the clinical feasibility of TFCC examination.CONCLUSION
We have validated the clinical feasibility of mobile medical screening for wrist injuries in tennis players using the portable MRI.Acknowledgements
No acknowledgement found.References
[1] Y. Okamoto et al., Incidence of elbow injuries in adolescent baseball players: screening by a low field magnetic resonance imaging system specialized for small joints, Jpn J Radiol, 34: 300-6 (2016).
[2] K. Tanabe et al., Development of a small-car mountable MRI system for human extremities using a 0.2 T permanent magnet, Proc. Intl. Soc. Mag. Reson. Med. 26, 4423, (2018).
[3] M. Nakagomi et al., Development of a small car-mounted magnetic resonance imaging system for human elbows using a 0.2 T permanent magnet, Journal of Magnetic Resonance 304 1-6, (2019).
[4] M. Nakagomi et al., Image denoising with deep transfer learning for screening baseball elbow injuries using portable scanners, Proc. Intl. Soc. Mag. Reson. Med. 27, 1419, (2019).
Figures