2788
Value of fractional anisotropy and apparent diffusion coefficient of diffusion tensor imaging in diagnosing early carpal tunnel syndrome1Radiology, Toho University Sakura Medical Center, Sakura, Japan
Synopsis
There are
decreased FA and increased ADC significantly with age in healthy subjects. There
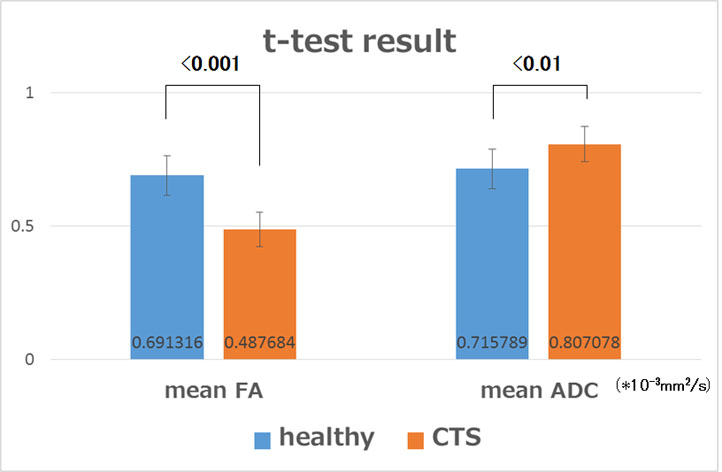
are significant differences in FA and ADC between early-stage CTS
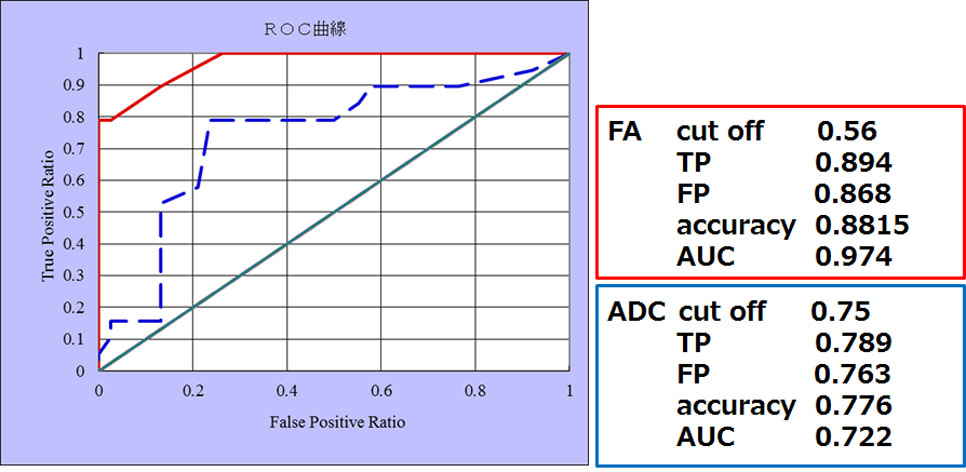
subjects and age-matched healthy subjects. 0.56 was found to be cutoff value for FA with 89% sensitivity and 88% accuracy and 0.75x10-3mm2/s was found to be cutoff value for ADC with 79% sensitivity and 78% accuracy. Although FA and ADC well correlate with clinical examinations and NCS results,
the value of FA is much stronger than that of ADC for diagnosing CTS earlier. DTI can be used for the early diagnosis of CTS.
Purpose
Early diagnosis and treatment are important to avoid permanent damage to the median nerve. The sign of peripheral nerve impairment including carpal tunnel syndrome is important to detect and assess background diseases. The purpose of this study was to assess the value of fractional anisotropy (FA) and apparent diffusion coefficient (ADC) in diagnosing early carpal tunnel syndrome (CTS).Materials and methods
At the first step, 100 wrist joints in 50 healthy subjects (30 males, 20 females; 20-69 years) were enrolled. Correlations of FA and ADC in diffusion tensor imaging of the median nerve (DTI) with age, sex, and nerve conduction study of the median nerve (NCS) were assessed. At the second step, 19 wrist joints 12 subjects with early stages of CTS (8 males, 4 females; mean age=62years) and 38 wrist joints in 19 age-matched healthy subjects (11 males, 8 females; mean age=52years) were enrolled. Diagnosis and severity of CTS were determined based on clinical and NCS examinations. All the subjects underwent DTI of the wrist joint at 3T (MAGNETOM Skyra; Siemens). The imaging parameters were as follows; single-shot EPI, FOV: 130mm, matrix: 100x100, TR/TE: 6500/81ms, dist.fact: 0%, BW: 1220Hz/px, PAT mode: GRAPPA, Fay.sap: SPAIR, slice thickness: 4mm, MPG-directions: 10, NEX: 3. On the transverse images of DTI at the distal end of the radius, FA and ADC of the median nerve were measured. All the subjects underwent NCS. In the healthy subjects, to correlate FA and ADC with NCS results, Pearson’s correlation test was used. To assess the differences of FA and ADC between early CTS and age-matched healthy subjects, Student T-test and ROC curve analysis were used. P value < .05 indicated a statistically significant difference.Results
In the healthy subjects, FA decreased with age, while ADC increased with age. FA had a good correlation with NCS results (p<0.001). There was no significant difference in FA and ADC depending on sex. There were statistically significant differences in FA (p<0.001) and ADC (p<0.01) between early CTS and age-matched healthy subjects (Fig.1). From the ROC curve analysis, the cutoff values for FA and ADC used for the early diagnosis of CTS were 0.56 and 0.75x10-3mm2/s with AUC of 0.974 and 0.722, respectively (Fig.2).Discussion
The main findings in this study are that there are decreased FA and increased ADC significantly with age in healthy subjects. There are significant differences in FA and ADC between early CTS and age-matched healthy subjects. Although FA and ADC well correlate with clinical examinations and NCS results, the value of FA is much stronger than that of ADC for the early diagnosis of CTS.Quantitative evaluation of DTI in CTS subjects has already been shown to be feasible by calculating two commonly used parameters, FA and ADC, in attempting to obtain values for CTS and healthy subjects, with wide diversity shown in different studies (1-9). In the previous studies, FA ranging between 0.359 and 0.64 and ADC ranging between 0.99x10-3mm2/s and 1.866x10-3mm2/s were shown for CTS subjects. Our calculated values for CTS subjects fall within the range of FA, but do not fall within the range of ADC: 0.488 and 0.807x10-3mm2/s for mean FA and ADC, respectively. Although the range of ADC in the previous studies showed wider, our results of mean ADC were lower than those in the previous studies. This may be attributed to the difference in severity of CTS subjects enrolled in the study. Several investigators speculated that reduction in FA and increase in ADC may be due to chronic compression, which may lead to histologic changes within the nerves.
To the best of our knowledge, there are few studies that could determine cutoff values for FA and ADC for diagnosing CTS. Guggenberger et al.(1) showed 0.47 as a cutoff value for FA with a sensitivity and specificity of 83% and 67%, respectively and 1.05x10-3mm2/s as a cutoff value for ADC with a sensitivity and specificity of 83% and 54%, respectively. Klauser et al. (8) showed 0.62 as a cutoff value for FA with a sensitivity and specificity of 83% and 67%, respectively. In our study, 0.56 was found to be cutoff value for FA with 89% sensitivity and 88% accuracy, while 0.75 x10-3mm2/s was found to be cutoff value for ADC with 79% sensitivity and 78% accuracy. Our results regarding cutoff value for FA are within the range of the two previous studies, but those regarding cutoff value for ADC are not in accord with Guggenberger et al.. This may be attributed to the difference in severity of CTS subjects enrolled in the study. There is considerable variation in ADC relative to FA.
Our study did have some limitations, with the relatively low number of CTS subjects included being the first and most important of them. Second, cross-sectional areas of the median nerve were not measured and analyzed.
Conclusion
DTI can be used for diagnosing early CTS. Cutoff values for FA and ADC used for the diagnosis of CTS were 0.56 with high accuracy and 0.75x10-3mm2/s with moderate accuracy, respectively. Although FA and ADC well correlate with clinical examinations and NCS results, the value of FA is much stronger than that of ADC for diagnosing CTS earlier.Acknowledgements
No acknowledgement found.References
1. Guggenberger R, et al. Assement of median nerve with MR neurography by using diffusion-tensor imaging: normative and pathologic diffusion values. Radiology 265:194-203, 2012
2. Hiltunen J, et al. Pre- and post-operative diffusion tensor imaging of the median nerve in carpal tunnel syndrome. Eur Radiol 22(6):1310-1319, 2012
3. Stein D, et al. Diffusion tensor imaging of the median nerve in healthy and carpal tunnel syndrome subjects. J Magn Reson Imaging 29(3):657-662, 2009
4. Naraghi A, et al. Diffusion tensor imaging of the median nerve before and after carpal tunnel release in patients with carpal tunnel syndrome: feasibility study. Skeletal Radiol 42(10):1403-1412, 2013
5. Lindberg PG, et al. Diffusion tensor imaging of the median nerve in recurrent carpal tunnel syndrome-initial experience. Eur Radiol 23(11):3115-3123, 2013
6. Kabakci N, et al. Diffusion tensor imaging and tractography of median nerve: normative diffusion values. AJR Am J Roentgenol 189(4):923-927, 2007
7. Filli L, et al. Accelerated magnetic resonance diffusion tensor imaging of the median nerve using simultaneous multi-slice echo planar imaging with blipped CAIPIRINHA. Eur Radiol 26(6):1921-1928, 2016
8. Klauser AS, et al. Carpal tunnel syndrome assessment with diffusion tensor imaging: value of fractional anisotropy and apparent diffusion coefficient. Eur Radiol 28:1111-1117, 2018
9. Paniandi V, et al. MR neurography of median nerve using diffusion tensor imaging (DTI) and its efficacy to diagnose carpal tunnel syndrome in Malaysian population. Neurology Asia 23(1):17-25, 2018
Figures