2787
Advanced Knee Imaging Study in NCAA Division 1 Basketball Update: Study Design and Considerations for Multi-Site Longitudinal Study1Radiology, Stanford University, Stanford, CA, United States, 2Radiology, Hospital for Special Surgery, New York City, NY, United States, 3GE Healthcare, Waukesha, WI, United States, 4Stanford University, Redwood City, CA, United States, 5Hospital for Special Surgery, NYC, NY, United States, 6University of California San Francisco, San Francisco, CA, United States, 7Stanford University, Stanford, CA, United States
Synopsis
Knee injuries are especially common in jumping athletes, and, in particular, elite basketball players. We present an update two years into a multi-site study analyzing the results of a common phantom in assessing biases across and within MRI scanners, as well as to characterize the effectiveness of recruitment, assessment, and study design strategies. It was shown that more timepoints of quantitative values potentially corrects for quantitative biases longitudinally within one scanner. As attrition rates are high for athletes in general, consistent and effective methods of recruitment, early identification of key athletes, and standardized methods of assessment are all necessary.
Introduction
Knee injuries are common in jumping athletes, and, in particular, elite basketball players, who place high loads on their knee 1,2 To evaluate early degenerative changes in elite college basketball players, we have implemented a multi-site, longitudinal study. This study utilizes advanced quantitative MRI techniques to assess joint structures and articular cartilage across multiple collegiate seasons of Division 1 National Collegiate Athletic Association (NCAA) female and male basketball players and a comparison group of NCAA swimmers 3. In this work, we present an update two years into the study, including strategies and challenges in recruitment and retention as well as methods to assess biases in phantom quantitative measurements with the study protocol. The objective is to analyze the results of a common phantom in assessing biases across and within study scanners, as well as to characterize the effectiveness of the strategies used in recruitment, retention, and study design.Methods
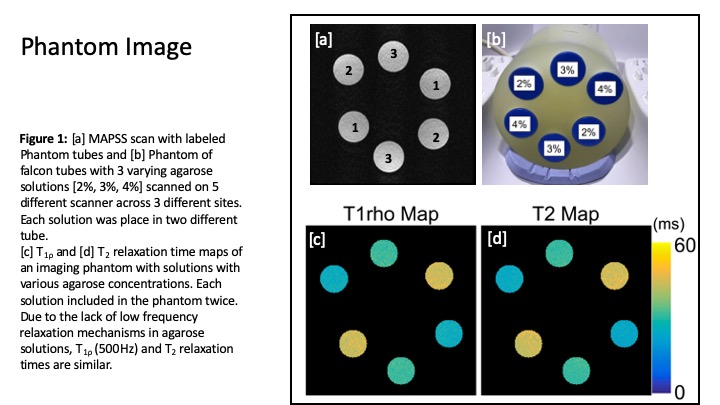
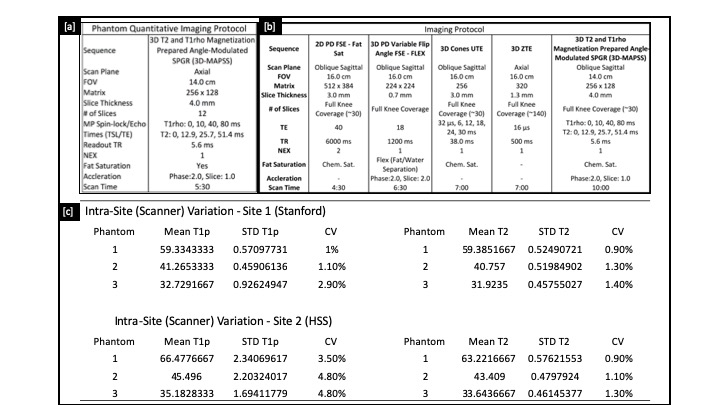
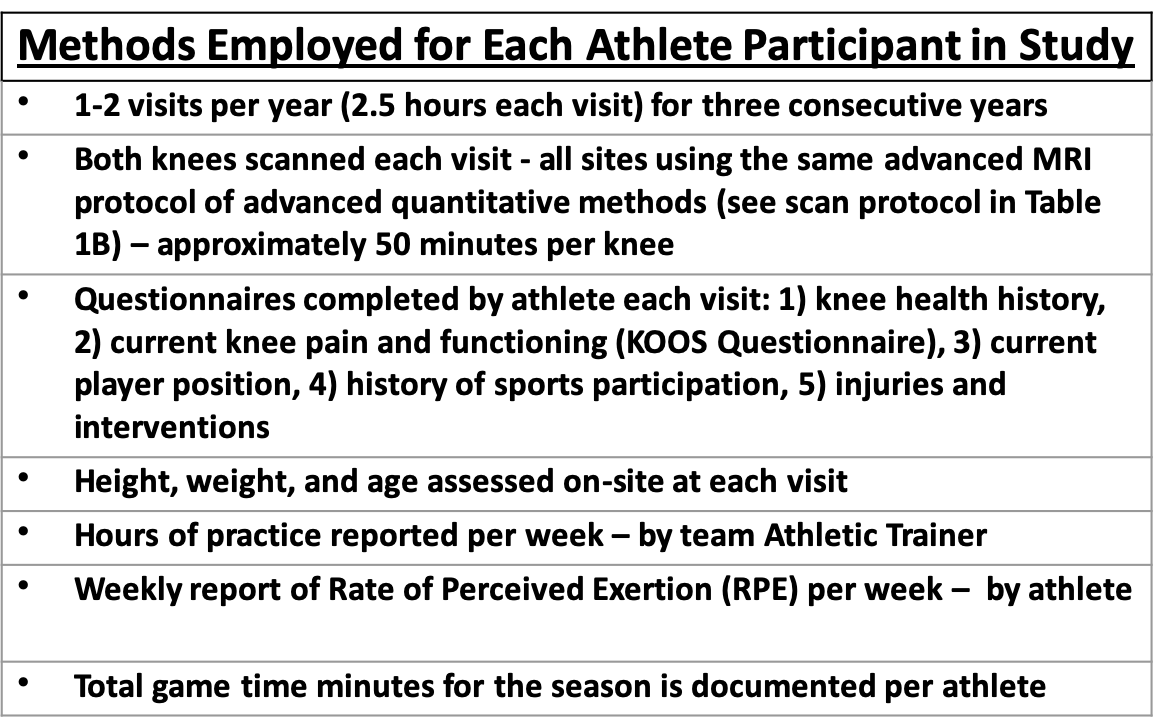
Phantom Study: To evaluate bias of quantitative metrics across sites, scanner hardware, and time points, identical phantoms with known T2/T1ρ values (Figure 1a&b) were imaged on multiple participating scanners at 3 different time points (Baseline, Year 1 and Year 2). Imaging was performed with a 3D sagittal combined T1ρ/T2 magnetization-prepared angle-modulated portioned k-space spoiled gradient echo snapshots (MAPSS) sequence 4. T2/T1ρ relaxation time maps were computed using a mono-exponential fit of signal data acquired at various echo/spin-lock (TE/TSL) times. Intra-scanner reproducibility of T2/T1ρ measurements for each phantom solution was assessed with coefficients of variation (CV). 5,6,7Imaging Study: The imaging protocol is shown in Table 1. The standard procedure for each visit is listed in Table 2. Standardized tools were used to identify knee pain (Knee injury and Osteoarthritis Outcome Score (KOOS)) and practice intensity (session Rate of Perceived Exertion (sRPE)) 8,9. in addition, history questionnaires, practice, and game playing data was collected. Recruitment was done through initial identification of qualifying athletes by the Athletic Trainer for each team, then taken over by the Study Coordinator. Statistical analysis of attrition rates was done using a one-way ANOVA test.
Results
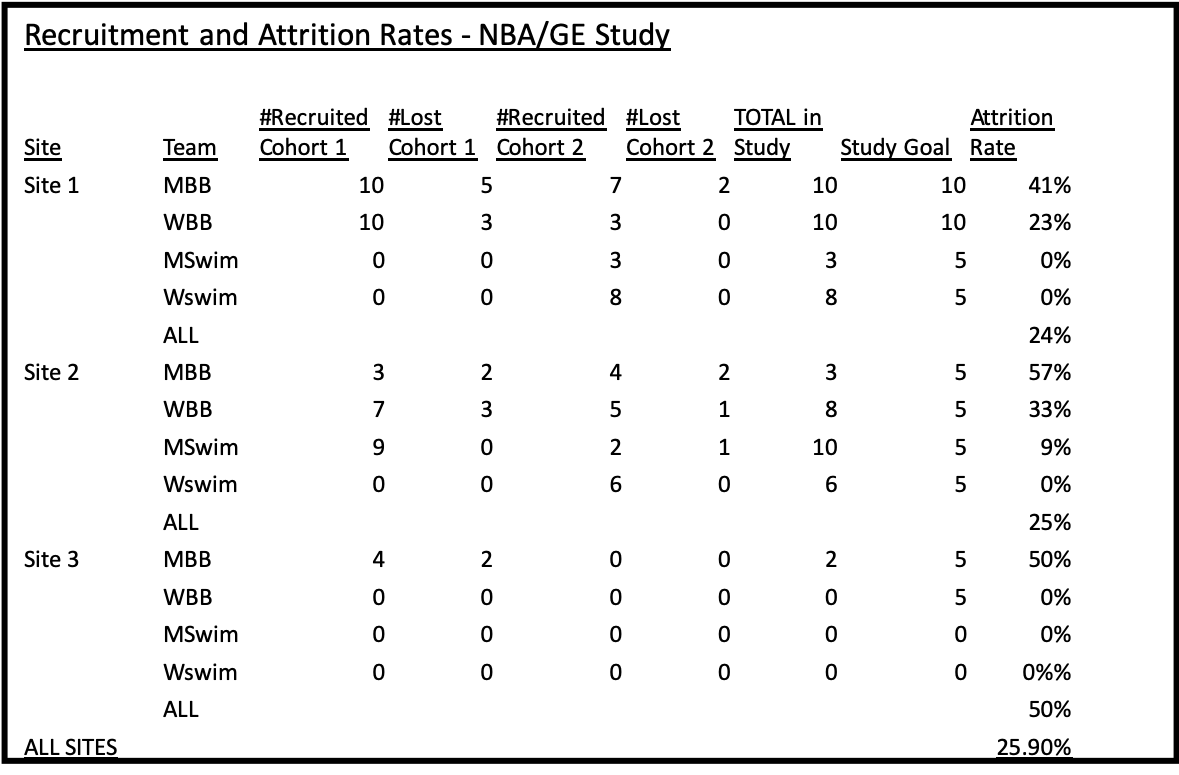
Phantom Study: Intra-scanner repeatability was high for T2/T1ρ relaxation times in Site 1 and T2 of Site 2 with CVs ranging from 0.9%-2.9%. Intra-scanner T1ρ measurements for Site 2 were less consistent with CV’s ranging from 3.5%-4.8% (Table 1).Imaging Study: To date, 33 basketball players and 27 swimmers are currently enrolled in the study (Table 3). Recruitment challenges were largely driven by the limited availability of qualifying student athletes as well as communication challenges between study investigators, team physicians and trainers. An additional site and second cohort were added due to low overall initial recruitment as well as high attrition rates (25.9%). The rate of attrition for basketball players was significantly higher than swimmers overall (XX% vs. YY%, P=0.001), and within the basketball players, male attrition was significantly higher than females (WW% vs. ZZ%, P=0.047). The largest factor leading to a high attrition rate was athletes leaving the athletic program. Identifying assessment tools and procedures that were consistent across the three sites was challenging, as introducing new methods or procedures into an athletic program was occasionally rejected by athletic staff as being too disruptive.
Discussion
The phantom data shows the challenges of quantitative measurements in a multi-year study. The low intra-scanner CVs from a scan repeated three times in one day of 0.2-2.2% 3 compared to CVs ranging from 0.9%-4.8% across three timepoints over 1.5 years indicates greater longitudinal variability. Quantifying the magnitude of T1p and T2 changes within a site as well as between sites, due to site-specific scanning hardware, is necessary to aid in correcting for quantitative biases longitudinally, as well as for assigning thresholds of T1p and T2 values to clearly define clinically relevant changes within the articular cartilage.Regarding our multi-site study design, methods of recruitment and assessment were consistent across all sites. Study methods were standardized whenever possible and did not interfere with the current procedures employed the participating sites. Attrition rates were highest for male basketball players as compared to female basketball players, and all swimmers. Attrition needs to be accounted for when determining target recruitment goals for the study. For this multi-site study, it was essential to establish the key coordinators for each site, each on-site data-collection staff, and an easily navigable data collection tool before any data collection occurred in order to have a smooth and effective study.
Conclusion
In this study, there is a wealth of quantitative information that is being collected. Prospectively studying these changes, between high and low impact athletes, as well as correlating imaging findings with training intensity data, will help provide some insight into the ability of cartilage and other tissues to handle stress and recover homeostasis. This will further our understanding of the rate of changes to the joint tissues and the cumulative effects of a training season, as well as the timing and ability to recover, which is critical to keeping players healthy and informing effective injury prevention programs.Acknowledgements
This work was funded by the NBA and GE Healthcare Orthopedics and Sports Medicine Collaboration.References
1. Brunner MC, Flower SP, Evancho AM, Allman FL, Apple DF, Fajman WA. MRI of the athletic knee. Findings in asymptomatic professional basketball andcollegiate basketball players. Invest Radiol 1989; 24:72-75.
2. Major NM, Helms CA. MR Imaging of the knee: findings in asymptomatic collegiate basketball players. AJR Am J Roentgenol 2002; 179:641-644.
3. Young KA, Kogan, F, Peters, RD, et al. Advanced Knee Imaging Study in NCAA Division 1 Basketball: Protocol Development and Preliminary Results, ISMRM, Paris, France, 2018.
4. Li, X., Han, E. T., Busse, R. F., & Majumdar, S. (2008). In vivo T(1rho) mapping in cartilage using 3D magnetization-prepared angle-modulated partitioned k-space spoiled gradient echo snapshots (3D MAPSS). Magnetic resonance in medicine, 59(2), 298–307. doi:10.1002/mrm.21414
5. Li X, Cheng J, Lin K, Saadat E, Bolbos RI, Jobke B, Ries MD, Horvai A, Link TM, Majumdar S. Quantitative MRI using T1rho and T2 in human osteoarthriticcartilage specimens: correlation with biochemical measurements and histology. Magn Reson Imaging 2011; 29:324-334.
6. Stahl R, Luke A, Li X, Carballido-Gamio J, Ma CB, Majumdar S, Link TM. T1rho, T2 and focal knee cartilage abnormalities in physically active and sedentary healthy subjects versus early OA patients –a 3.0-Tesla MRI study. Eur Radiol 2009; 19:132-143.
7. Li X, Pai A, Blumenkrantz G, Carballido-Gamio J, Link T, Ma B, Ries M, Majumdar S. Spatial distribution and relationship of T1rho and T2 relaxation times in knee cartilage with osteoarthritis. Magn Reson Med 2009; 61:1310-1318.
8. Turner A, Bishop C, Marshall G, Read P. How to Monitor Training Load and Mode using sRPE. Professional Strength and Conditioning, 2015; 39:15-19.
9. Clark N, Farthing JP, Norris SR, Arnold BE, Lanovaz JL. Quantification of Training Load in Canadian Football
Figures