2779
Zero Echo Time Imaging of the knee
Saya Horiuchi1, Taiki Nozaki1, Shigekazu Funada1, Atsushi Nozaki2, Hiroyuki Kabasawa2, Yasuyuki Kurihara1, and Nobuto Kitamura3
1Radiology Department, St. Luke's International Hospital, Tokyo, Japan, 2GE Healthcare, Japan, Tokyo, Japan, 3Orthopedic Department, St. Luke's International Hospital, Tokyo, Japan
1Radiology Department, St. Luke's International Hospital, Tokyo, Japan, 2GE Healthcare, Japan, Tokyo, Japan, 3Orthopedic Department, St. Luke's International Hospital, Tokyo, Japan
Synopsis
Zero Echo Time (ZTE) MR imaging provides “CT-like” contrast for cortical bone of the knee. We compared sagittal images of CT and ZTE of 15 patients, and demonstrated inter-modality agreement between morphology of the cortical bone of the tibia from CT and ZTE images. Metallic screws were blurred on ZTE in patients who underwent Anterior cruciate ligament (ACL) reconstruction. ZTE may be used clinically instead of CT in some cases who can undergo ACL reconstruction.
Introduction
- Anterior cruciate ligament (ACL) reconstruction is one of the most commonly performed sports medicine procedures, with approximately 100,000 procedures performed in the United States per year1. Correct positioning and alignment of the femoral and tibial tunnels are crucial for graft stability and good clinical outcomes, and it should be evaluated in every patient who has undergone ACL reconstruction2. CT is a useful modality for the evaluation of bone morphology of the knee, but radiation exposure is unavoidable. Traditional magnetic resonance (MR) imaging pulse sequences have been used to evaluate ligamentous injury, but cortical bone is depicted as signal void because of its inherent short T2 relaxation time. Therefore, information for diagnosis or surgical planning, possible complications frequently requires patients to undergo multiple cross-sectional examinations to assess both ligamentous injury and osseous structure.
- Zero echo time (ZTE) imaging provides enhanced bone contrast in MR imaging and may obviate concomitant CT and its attendant radiation. ZTE imaging has a great signal-to-noise ratio and scan time efficiencies, advantageous to acquiring images at near-isotropic resolution and multiplanar reconstruction3,4.
- The purpose of this study is to compare the usefulness of ZTE imaging and CT for the evaluation of the skeletal shape of the knee.
Materials and Methods
- The study protocol was approved by the institutional review board, and all subjects provided written informed consent. Fifteen patients (14 males, 1 female; age range, 17-47 years; mean age 27.7) undergoing CT and MR imaging of the knee without intervening knee surgery were recruited from May to October 2019.The average time between CT and MR imaging was 208 days (range, 0 to 540 days). Of these 15 patients, 10 had a surgical history of the ACL reconstruction procedure.
- We acquired helical scans on a 64-channel detector CT scanner (Optima CT660, GE, Boston, MA, USA). The scan parameters were tube voltage, 120kV; tube current, 310 mA; rotation time, 0.5 s; pitch factor, 0.969; scan FOV, 32 cm; display FOV, 26 cm; detector configuration, 32 × 0.625 mm; reconstruction slice thickness, interval, 0.5 mm, and bone reconstruction. All axial images were reformatted into sagittal planes.
- ZTE MR images were acquired by using a prototype ZTE pulse sequence provided by GE Healthcare with a 3.0-T GE Discovery MR750w (GE Healthcare, Milwaukee, WI, USA) using an 8-channel knee coil (HD T/R Knee Array). Section thicknesses were 1 mm, and the field of view was 20 cm (pixel size, 0.625mm). Matrixes of 200 was used with repetition times of 484 msec, a flip angle of 1°, and a receiver bandwidth of 25 kHz. ZTE imaging time was 5 minutes and 42 seconds. After ZTE acquisition (Fig. 1A), a bias-correction algorithm (“N4”5) was applied to further flatten soft-tissue intensities and correct signal inhomogeneity due to coil geometry and variable tissue cross sections. Then, Image data were rescaled inverse-logarithmically (-log[image]), yielding positivecontrast for bone (Fig. 1B). Histogram-based thresholding was used to remove the background, retaining bone and soft tissue6,7.
- Visualization of the bones and metallic interference screws that were used in post-ACL reconstruction patients on ZTE MR images was scored using CT images as the reference standard. Scores were made on sagittal reformatted CT and ZTE images (Fig. 2). To evaluate the tibial plateau, we used volume-rendering (VR) images (Fig.3). The diagnostic performance of MR and CT images with respect to bone sharpness and morphology was compared and graded on the 5-point Likert scale8,9 as 5 = MRI definitely superior, 4 = MRI slightly superior, 3 = MRI and CT almost the same, 2 = MRI slightly inferior to CT but diagnosis possible, 1 = MRI definitely inferior. Image evaluation was performed by two board-certified musculoskeletal radiologists independently (S.H. and T.K., with 9 and 16 years of experience, respectively). Disagreements on scores were resolved by discussion.
- When the number of specimens with a score of 4 or 5 exceeded that of specimens with a score of 1 or 2, we considered the diagnostic ability of MRI superior to CT. On the other hand, when the number of specimens with a score of 1 or 2 exceeded that of specimens with a score of 4 or 5, we considered the diagnostic ability of CT superior to MRI.
Results
Results of the visualization scores are shown in Table 1. All of the visualization scores of sagittal images of femur and tibia were 3 (the depiction of shape and edge of the bone are the same on CT and ZTE images). In 3 of 15 patients, visualization scores of patella were 2 (The cortical bone is blurred on the ZTE but its contour can be identified). All of the visualization scores of VR images of tibial plateau were 3. All of the visualization scores of screws were 1 (screws are blurred, and the contour is uncertain on the ZTE) (Fig. 4).Summary
- ZTE MR imaging provides “CT-like” contrast for bone.
- The results of this study demonstrate the inter-modality agreement between morphology and sharpness of the cortical bone of the tibia from CT and ZTE images. Metallic screws were blurred on ZTE in patients who underwent ACL reconstruction.
- ZTE may be used clinically instead of CT in some cases who can undergo ACL reconstruction.
Acknowledgements
No acknowledgement found.References
- Csintalan RP, Inacio MC, Funahashi TT, et al. Incidence rate of anterior cruciate ligament reconstructions. The Permanente Journal 2008; 12:3
- omczak RJ, Hehl G, Mergo PJ, et al. Tunnel placement in anterior cruciate ligament recon- struction: MRI analysis as an important factor in the radiological report. Skeletal Radiol 1997; 26:409–413
- Weiger M, Pruessmann KP. MRI with zero echo time. eMagRes 2012;1(2):311–321.
- Breighner RE, Endo Y, Konin GP, et al. Technical Developments: Zero Echo Time Imaging of the Shoulder: Enhanced Osseous Detail by Using MR Imaging. Radiology. 2018 Mar;286(3):960-966.
- Tustison NJ, Avants BB, Cook PA, et al. N4ITK: improved N3 bias correction. IEEE Trans Med Imaging 2010;29(6):1310–1320.
- Wiesinger F, Sacolick LI, Menini A, et al. Zero TE MR bone imaging in the head. Magn Reson Med 2016;75(1):107–114.
- Delso G, Wiesinger F, Sacolick LI, et al. Clinical evaluation of zero-echo-time MR imaging for the segmentation of the skull. J Nucl Med 2015;56(3):417–422.
- Phelps AS, Naeger DM, Courtier JL, et al. Pairwise comparison versus Likert scale for biomedical image assessment. AJR Am J Roentgenol 2015; 204:8–14.
- Matsubara Y, Higaki T, Tani C, et al. Demonstration of Human Fetal Bone Morphology with MR Imaging: A Preliminary Study. Magn Reson Med Sci. 2019 Oct 15. doi: 10.2463/mrms.mp.2019-0105. [Epub ahead of print]
Figures
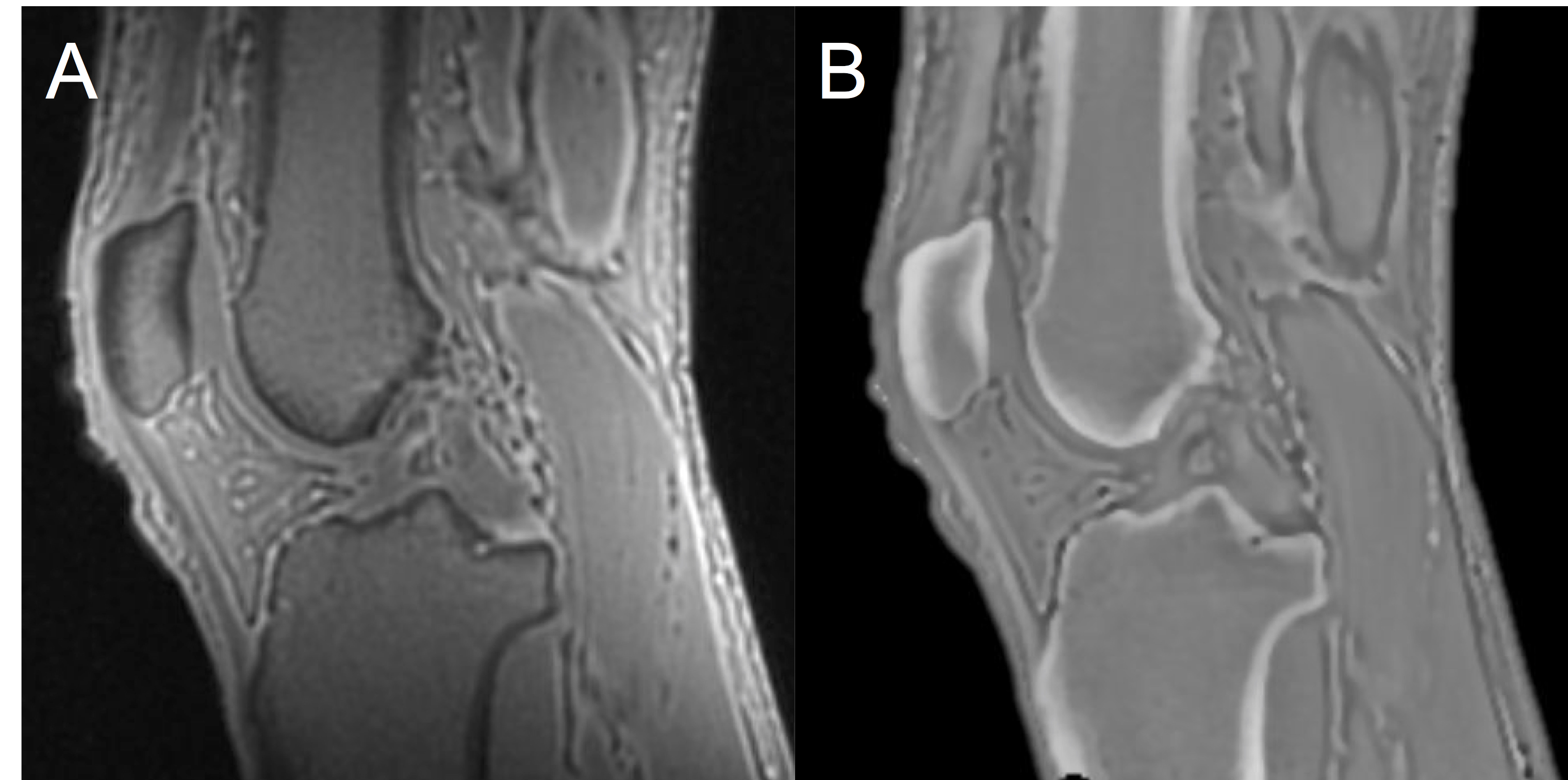
Figure 1: Sagittal MR images show postprocessingof ZTE data for CT-like positive bone contrast in a 41-year-oldman. (A) As-acquired ZTE MR image. (B) N4 bias- corrected and inverse-logarithmic rescaled image with background segmented.
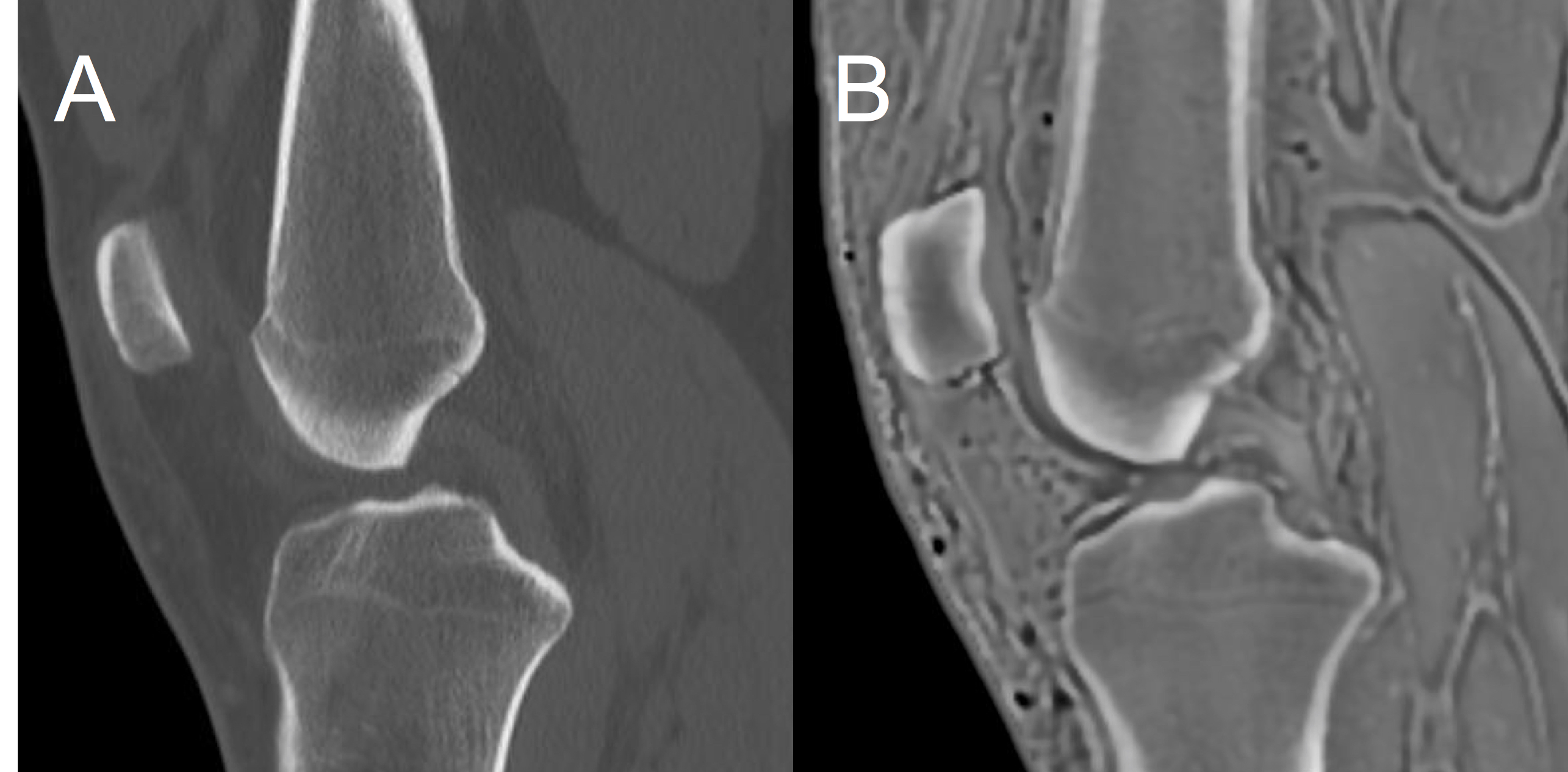
Figure 2: Sagittal images from (A) CT and (B) ZTE in a 20-year-old man. The shape and edge of the cortical bone are clear and the same on CT and ZTE image.
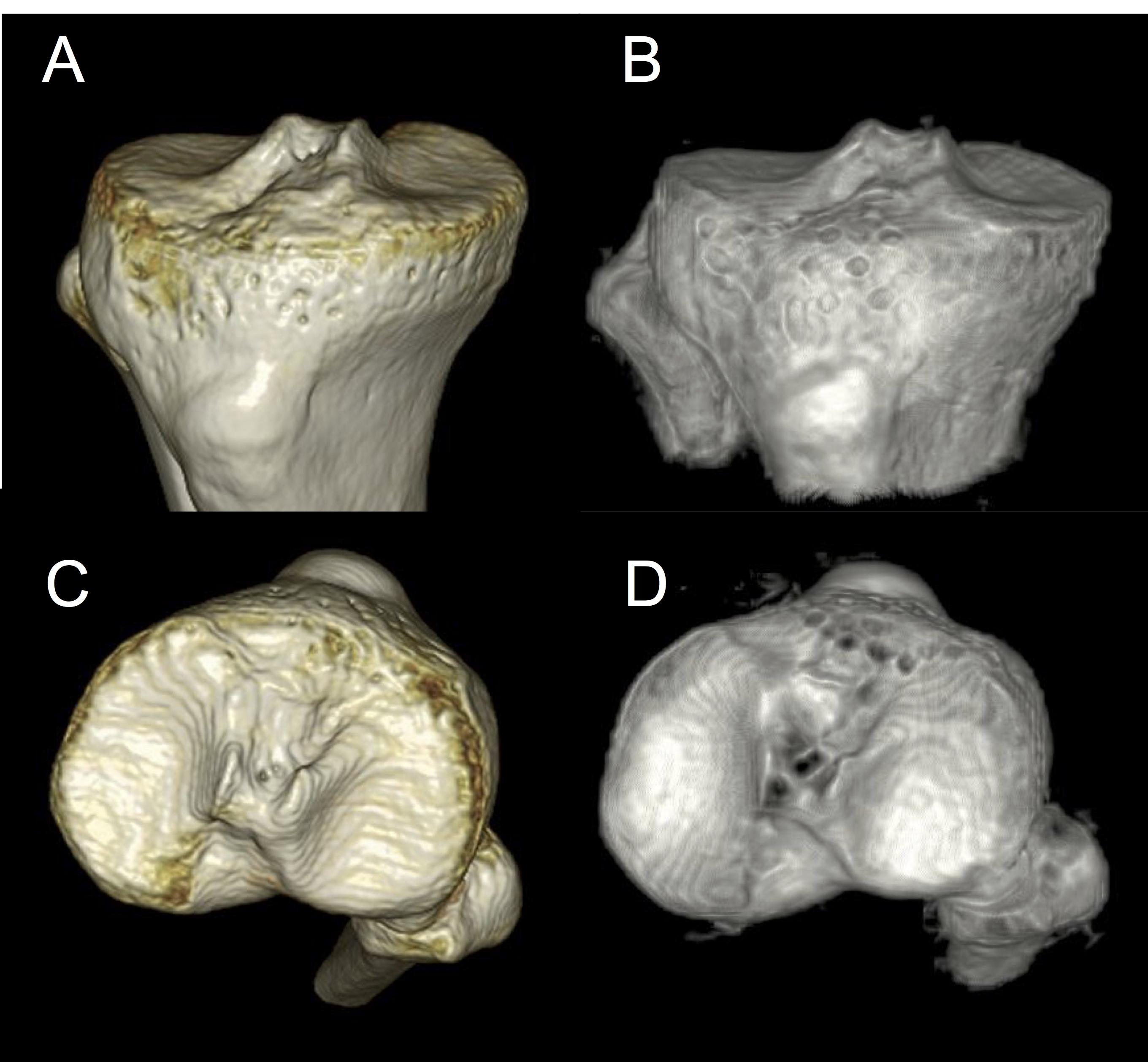
Figure 3. Volume rendering reconstructions from CT (A, C) and ZTE (B, D) in a 20-year-old man (the same patient as Figure 2). Slight differences are apparent between the three-dimensional models, due primarily to the difference in resolution between the CT and ZTE acquisitions, however, the shapes of the tibialplateau are the same on CT and ZTE image.
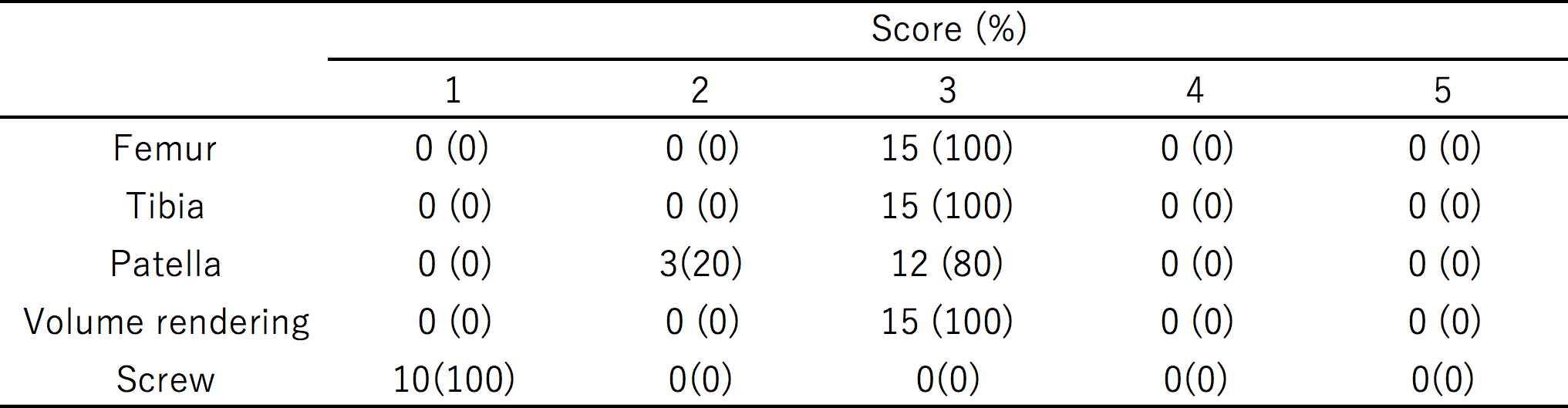
Table 1. Visualization scores of the bones and screws on ZTE MR images using CT images as the reference standard
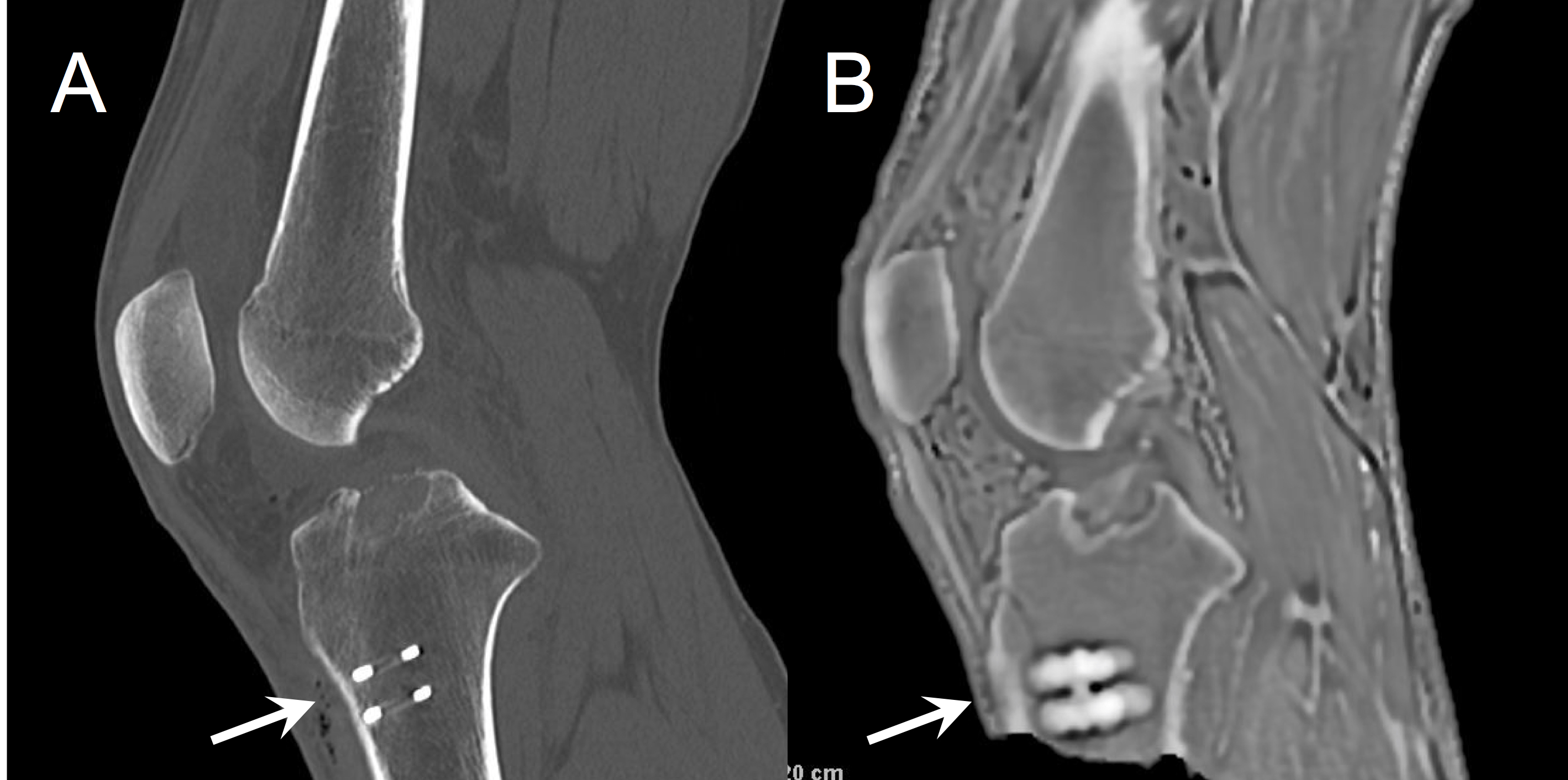
Figure 4: Sagittal imagesfrom (A) CT and (B) ZTE in a 33-year-old man with a history of ACL reconstruction. The screws (arrows) are blurred ,and the contour is uncertain on the ZTE.