2778
MRI models of the Age-Related Bone Loss: Insights from Multi-modal Imaging Study1Iran University of Medical Science, Tehran, Iran (Islamic Republic of), 2Quantitative Medical Imaging Systems Group, Tehran, Iran (Islamic Republic of), 3Tehran University of Medical Science, Tehran, Iran (Islamic Republic of), 4Laleh Hospital, Tehran, Iran (Islamic Republic of), 5Tehran University of medical science, Tehran, Iran (Islamic Republic of)
Synopsis
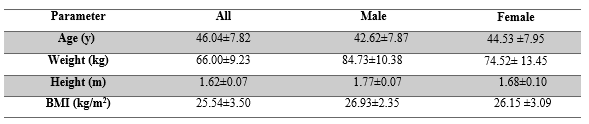
This study deals with assessing the ability of current clinical measures of bone to model the systematic age-related alteration of bone during aging and where does MRI stand as a new modality. Fifty Healthy volunteers with an average age of 44.53 ±7.95 were enrolled based on oral interviews and blood tests. Quantitative measurements were performed by various modalities for lumbar spine, forearm (DXA), Calcaneus (QUS), and Tiba (QCT and MRI). Pearson correlation coefficients was calculated between the bone parameters and age. The highest correlation coefficient between bone parameters and age was related to T1 (r = 0.766, p <0.01).
Introduction
Bone is a dynamic organ that serves mechanical and homeostatic functions, which alters during aging. This organ has a complex structure that can be studied from the macro-structural level (cortical and trabecular) to the microstructural level (Haversian system). Bone mineral density (BMD) quantification is currently the common clinical tool for the diagnosis of osteoporosis and is performed by dual-energy x-ray absorptiometry (DXA). BMD as a gold standard is not a good marker in many cases. There are cases where BMD is close to normal but with high fracture risk1, 2. Moreover, there are three main components in the cortical bone as mineral, collagen, and water, while BMD only provides information regarding minerals. Our main aim was to assess the relationships between bone features and age, extracted from different sites with available modalities; DXA, QUS, MRI, and MDCT-QCT to see which modality can model the age-related alterations for bone. We explored this relationship with a healthy population of 50 participants.Methods
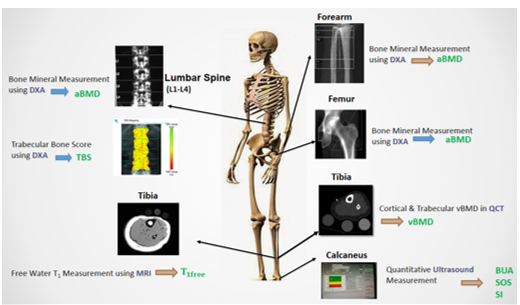
Participants: After approval of the human ethics committee and written informed consent, a cross-sectional population of 50 Iranian healthy volunteers (22M.28F, 30-60 years old) were recruited (Table 1).The population of the two genders was both age and BMI matched. The healthiness of the participants was investigated through four steps: filling a questionnaire, blood test, DXA scan, and eventually the specialist confirmation. Each participant went under four different modalities of bone assessment and different parameters were extracted as shown in Figure 1. The imaging site was selected according to the clinical routine of the imaging modality.
DXA: aBMD for L1-L4 spine, proximal femur, and forearm was measured by DXA (discovery W, Hologic Inc., Walton, MA).The mineral content was also used to see if the participant is in the normal category defined by WHO (aBMD; T score ≥ 3,4 Ultrasound (QUS): Ultrasound measurements of the calcaneus were performed with an Achilles plus device (GE Medical Systems Lunar, Madison, WI). This modality provided parameters as follows: Speed of Sound (SOS), Broadband Ultrasound (BUA) and Stiffness Index (SI).
Quantitative Computed Tomography (QCT): Multi-Detector Computed Tomography (MDCT) images of the distal tibia (38%) (Brilliance, Philips Medical Systems, Amsterdam, Netherlands) was acquired in Laleh hospital for all participants. The imaging parameters validated 5 were as follows: Hybrid iterative reconstruction algorithm (iDose - level 7), 90 kVp, ~30 effective mAs, 3 mm section thickness, 0.15*0.15 mm2 pixel size, 0.8 pitch factor, YC kernel, and 16×0.7 mm nominal collimation. The left leg of the subjects and solid-CIRS phantom (50, 100 and 250 mg CHA/cm3) were scanned, simultaneously. The cortical, trabecular and integral (cortical plus trabecular) volume BMD (vBMD) was calculated. Magnetic Resonance Imaging (MRI): T1 quantification was assessed on the left leg (distal tibia (38%)) at 1.5 T MR scanner (Siemens Healthcare, Erlangen, Germany) with variable time repetition (VTR) 6 Statistical Analysis: To test the normality assumption of the parametric tests, Kolmogorov-Smirnov was used. Mean and standard deviation (SD) were provided as descriptive statistics. The correlation between bone features and age were analyzed by Pearson correlation (r) analysis (ᾱ=0.05).
Results
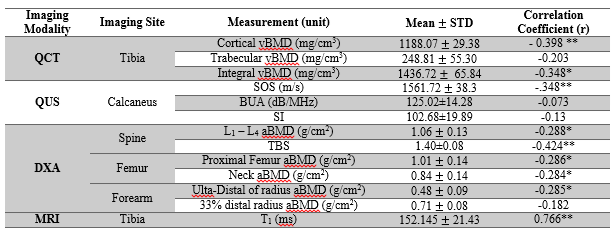
The mean and standard deviation (SD) of the measurements are presented in Table 2. The highest correlation with age were related to free water T1 in cortical bone (r= 0.77), (p<0.001). Moreover, the correlations between SOS and cortical vBMDs with age were (r=-0.35) and (r=-0.40) (p<0.001), respectively.Discussion and conclussion
Table 2 demonstrated that among QUS-derived features, SOS that measures the elasticity and architecture of bone7 showed the highest correlation (-0.348, p<0.05), which could barely be enough to model the age-related alterations. DXA and QCT parameters (measures of BMD) had a low correlation with age. QCT-derived features with the mean correlation of 0.316 (p<0.05) predicted age-related alterations better than DXA-derived features (-0.285, p<0.05) due to the ability to discriminate between trabecular and cortical and measuring vBMD rather than aBMD (being independent of the patient’s size). Cortical bone-free water T1 shows the highest correlation with age. The pulse sequence used for measuring T1 deployed proper TE value; large enough for the bound water signal to decay and small enough for free water to be captured. Therefore, T1 of free water, residing in the pores of the cortical bone is captured which reflects the information of the pore size and volume. During aging, the surface-to-volume ratio of the pores decreases leading to the restricted mobility of the water molecules and increasing the value of their T1 6. There was no correlation between trabecular or integral vBMD measurements and age. This might be due to small trabecular area and relatively poor resolution of MDCT at 38% of the distal tibia length.The systematic bone alteration with aging, in the bony skeleton, in 50 Iranian healthy population was assessed. The study showed that MRI could be a good modality to be added to the clinical routine for this purpose.
Acknowledgements
No acknowledgement found.References
1. Ettinger MP. Aging bone and osteoporosis: strategies for preventing fractures in the elderly. Archives of internal medicine. 2003;163(18):2237-46.
2. Lespessailles E, Chappard C, Bonnet N, Benhamou CL. Imaging techniques for evaluating bone microarchitecture. Joint bone spine. 2006;73(3):254-61.
3. Organization WH. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: report of a WHO study group [meeting held in Rome from 22 to 25 June 1992]. 1994.
4. Siris ES, Chen Y-T, Abbott TA, Barrett-Connor E, Miller PD, Wehren LE, et al. Bone mineral density thresholds for pharmacological intervention to prevent fractures. Archives of internal medicine. 2004;164(10):1108-12.
5. Malekzadeh M, Abbasi-Rad S, Keyak JH, Nabil M, Asadi M, Mobini N, et al. Liquid Calibration Phantoms in Ultra-Low-Dose QCT for the Assessment of Bone Mineral Density. Journal of Clinical Densitometry. 2019.
6. Akbari A, Abbasi-Rad S, Rad HS. T1 correlates age: A short-TE MR relaxometry study in vivo on human cortical bone-free water at 1.5T. Bone. 2016;83:17-22.
7.Hans D, Wu C, Njeh C, Zhao S, Augat P, Newitt D, et al. Ultrasound velocity of trabecular cubes reflects mainly bone density and elasticity. Calcified tissue international. 1999;64(1):18-23.
Figures