2735
To Evaluate the Effect of Normalization on Femur Cartilage T2 Values in Diagnosis of Osteoarthritis1Centre for Biomedical Engineering, Indian Institute of Technology, New Delhi, India, 2Biomedical Engineering, ASET, Amity University Haryana, Gurgaon, India, 3Mahajan Imaging Centre, New Delhi, India, 4Department of Biomedical Engineering, All India Institute of Medical Sciences, New Delhi, India
Synopsis
Quantitative MR parameters(such as T2-relaxation time) are sensitive to biochemical changes in the cartilage. The objective of the study was to evaluate the performance of different statistics parameters from T2 values of femur cartilage and normalized T2 map (Z-score T2 map) values for differentiating healthy vs OA patients as well as Early-OA (Grade-I and Grade-II), vs Risk-OA (Grade-III) patients. Multiple Statistic parameter from T2 map provided high accuracy in differentiation between healthy vs OA cartilage, while one of the static parameter of Z-score T2 map provided high accuracy in differentiation between early-OA vs Risk-OA.
INTRODUCTION
Quantitative analysis of changes in biochemical behaviour of cartilage using advanced MR techniques is helpful for the early diagnosis of OA1,2. One of the popular methods is T2 relaxation time mapping which is able to assess the changes in the collagen and water content present in the tissue2. Reported studies shows that the T2 value increases from healthy to OA patients; however, the trend is not following in different OA Grades2. One of the recent study3 reported that 36 % of the OA1 lesion showed lower T2 (ms) relaxation times due to focal lesions having low T2 value. Therefore, in some cases of OA Grade-I data shows a mixture of different focal lesions having low and high T2 value in the same region. It provides a biased mean T2 values which were not found to have a difference from the control group3. Objective of the current study is to evaluate the performance of different statistics parameters computed over T2 map and normalized T2 map (Z-score) values to differentiate the healthy vs OA as well as Early-OA(Grade-I and Grade-II) vs Risk-OA(Grade-III) categories.MATERIALS AND METHODS
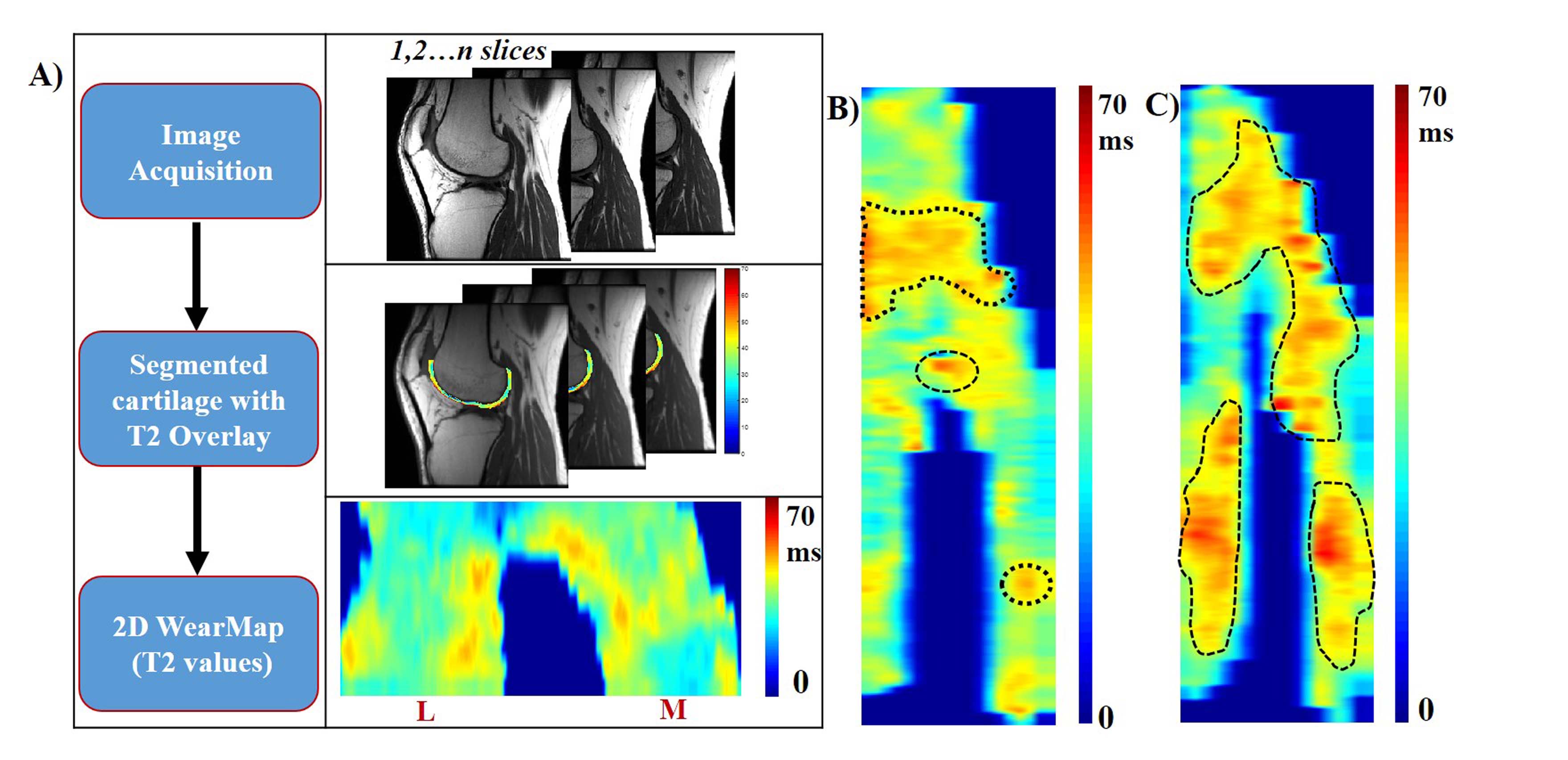
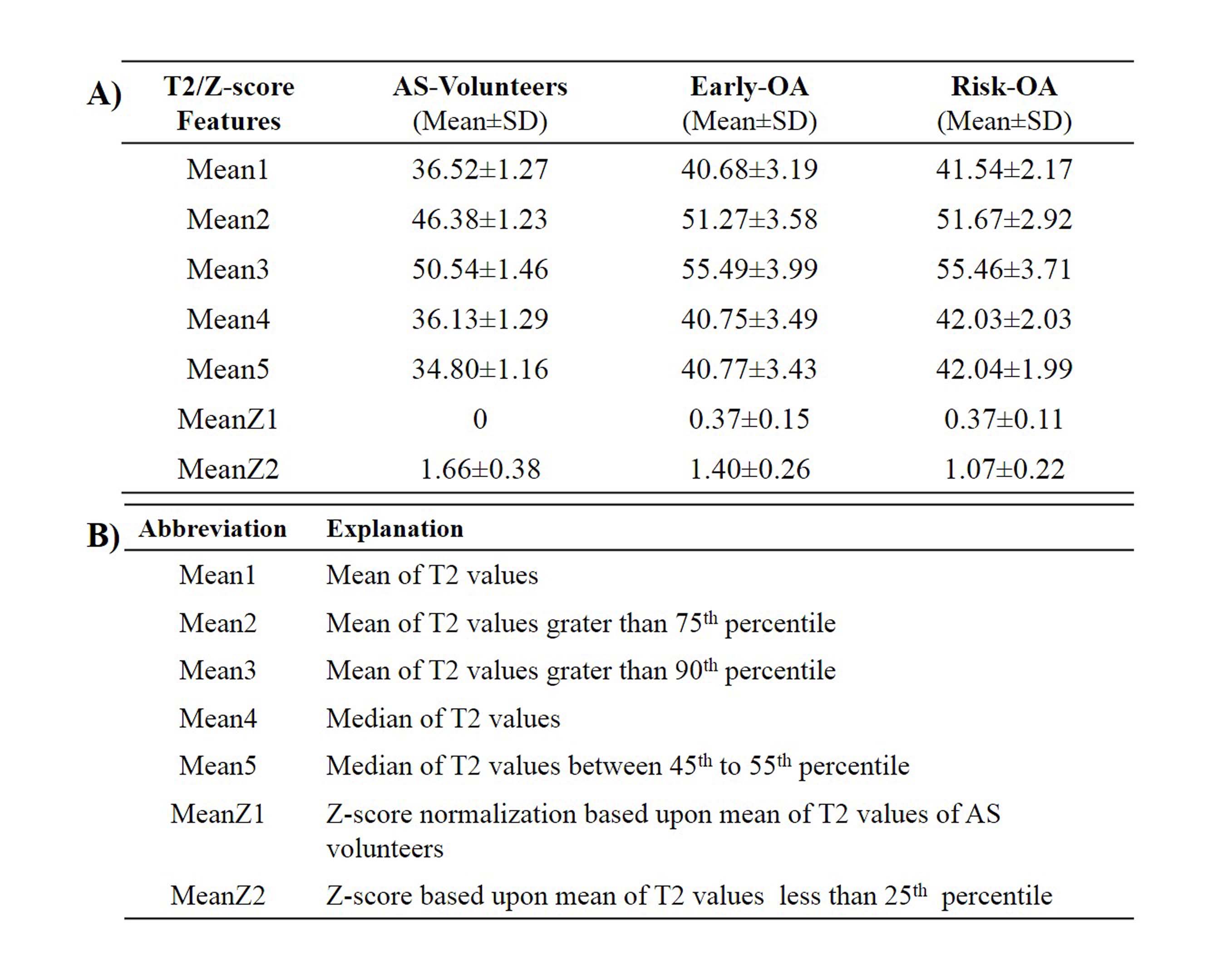
In this study, dataset of 4 asymptomatic(AS) male volunteers (mean age: 32±4 years) and 28 OA patients (mean age=45±23, sex(male%)=64) comprises of 20 Early-OA(Grade-I and Grade-II) and 8 Risk-OA(Grade-III)) were acquired using a 3.0T MRI scanner(GE Healthcare) with eight channel knee coil. MRI data at two repetitions were acquired for 4 asymptomatic(AS) subjects. The data was clinically evaluated using Outerbridge’s4 grading systems by an experienced radiologist with more than 15 years of experience in knee joint MRI. 39 lesions were found from 20 Early-OA subjects and 12 lesions from 8 Risk-OA subjects respectively. MRI protocol included acquisition of fat suppressed-proton density-fast spin echo (FS-PD-FSE) and T2 map sequence images of multiple slices. Acquisition parameters for FS-PD-FSE weighted images were: repetition time(TR)= 3000 ms, echo time(TE)= 27 ms, slice thickness= 4 mm, field of view(FOV)= 140×140 mm2, number of slices containing cartilage= 14-16. Acquisition parameters for T2-weighted FSE images were: TR= 1000 ms, TE= 6.4, 12.8, 19.2, 25.6, 32, 38.4, 44.8, 51.2 ms, slice thickness= 3 mm, FOV= 140×140 mm2, number of slices containing cartilage= 10-12. Articular cartilage from each slice was semi-automatically segmented using previously reported modified radial search algorithm5. From the segmented cartilage, a 2D-WearMap6,7 was generated for cartilage T2 values. Key steps of the methodology are illustrated in Figure 1(A). Mean(Mean1), median(Mean2), mean of values greater than 75th percentile(Mean3), mean of values greater than 90th percentile(Mean4) and mean of values between 45th percentile to 55th percentile(Mean5) was computed from T2 map(2D-WearMap) of cartilage tissue. Normalization of T2 map was performed using two different approaches: (i)Reported2 Z-score method (MeanZ1) with AS-volunteer mean T2 as reference (ii) Z-score normalization method(MeanZ2) based upon T2 mean of values less than 25th percentile of whole femur cartilage as reference. The statistical significance of the obtained results were calculated using unpaired two tail student’s t-test and the diagnostic performances were evaluated using Receiver-Operator-Characteristics(ROC) analysis.RESULTS
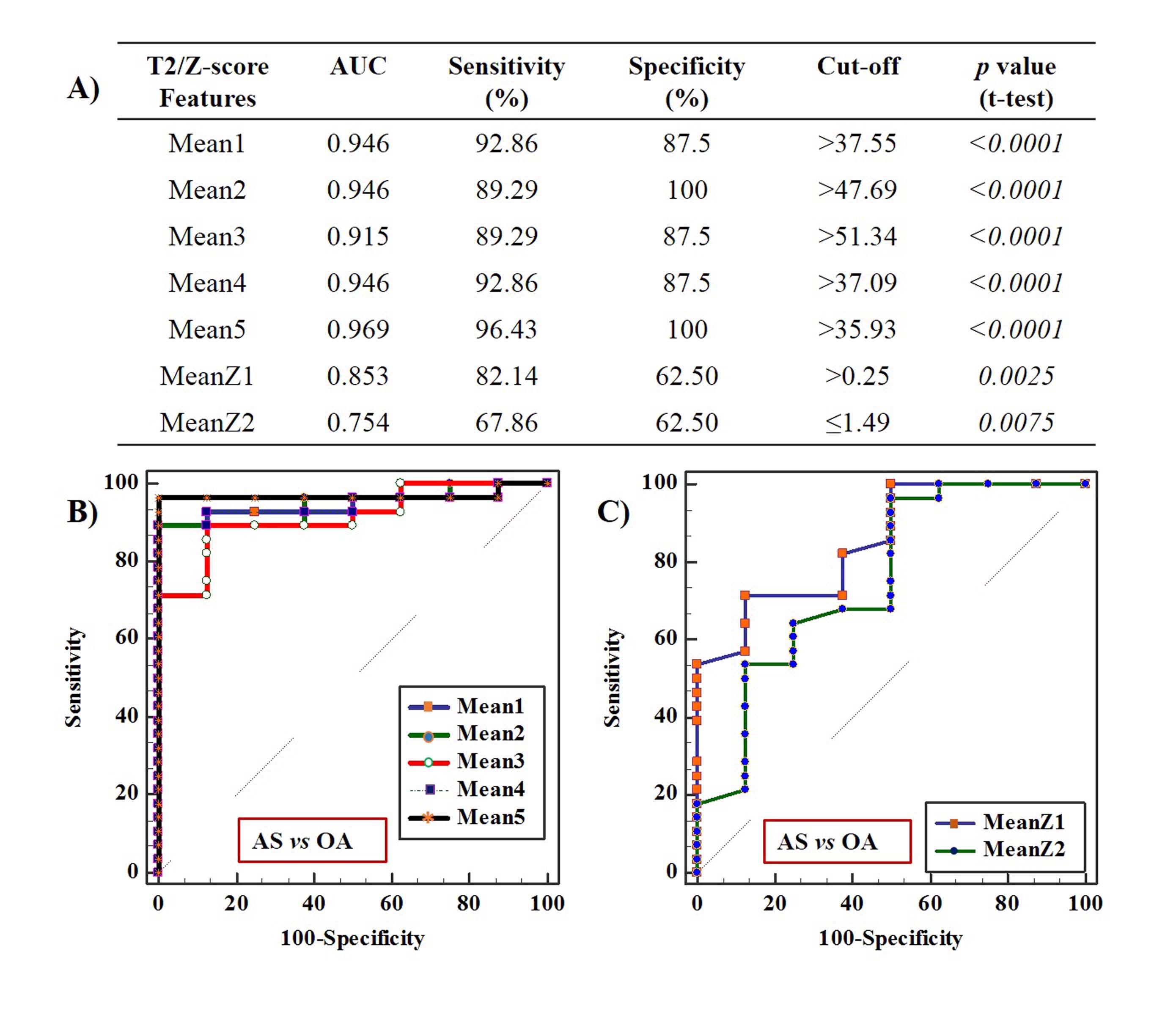
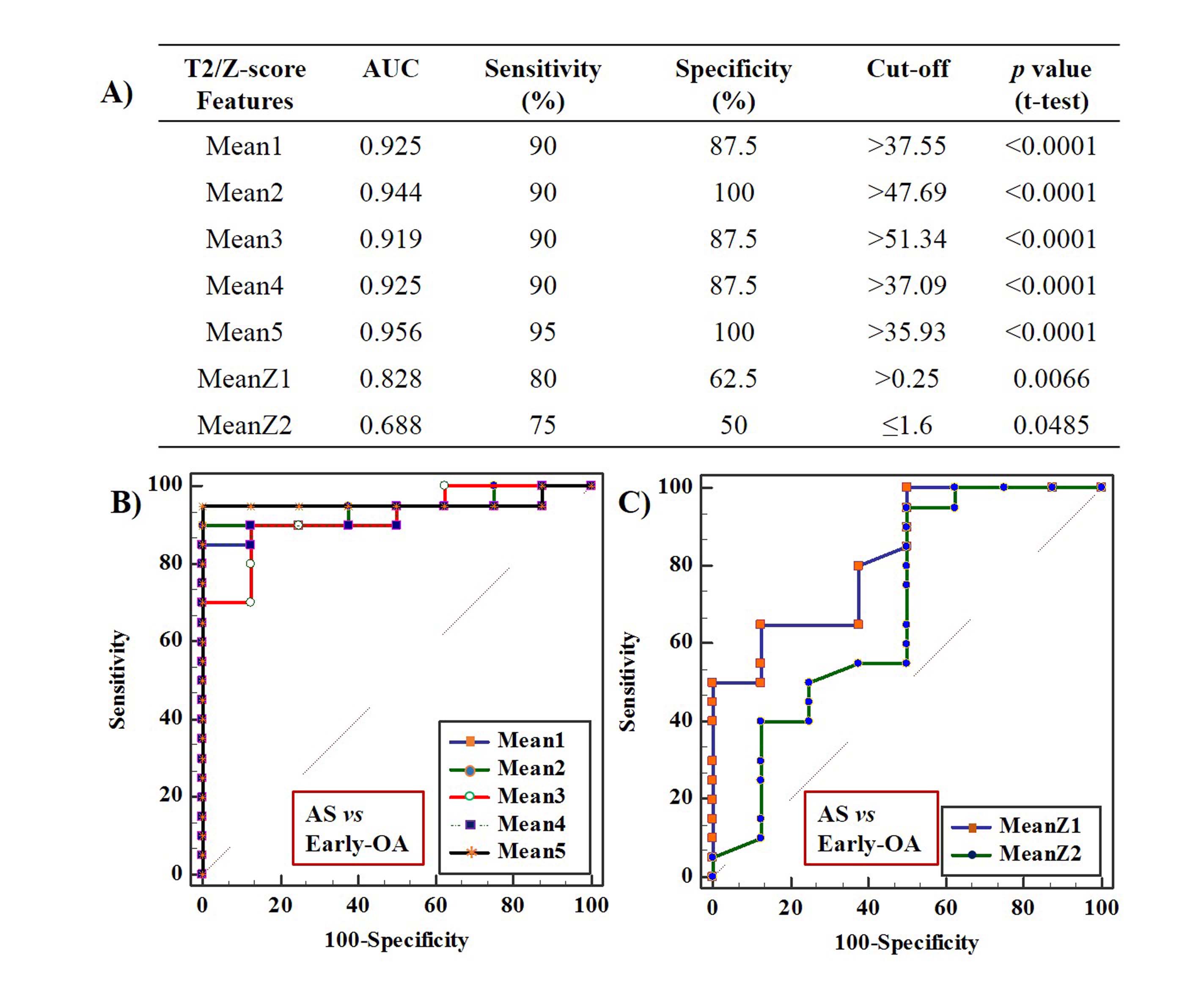
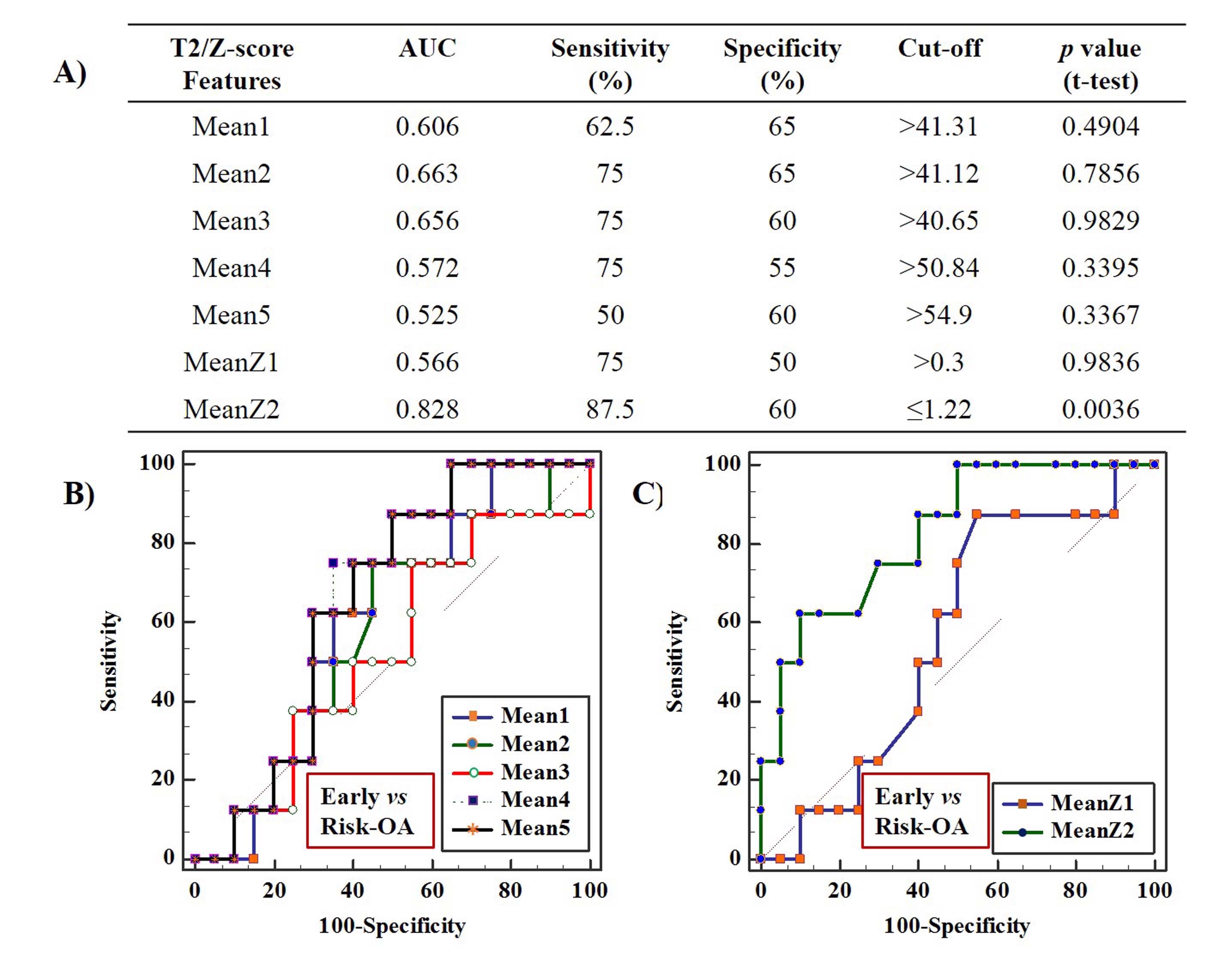
AS-volunteers and OA patient data analysis results were evaluated successfully using different statistics and normalization parameters of T2 values presented in Table 1(A). Figure 2 showed the ROC analysis results to distinguish AS-volunteers data from OA patient data. In this figure, Mean5 parameter showed comparatively highest AUC, sensitivity and specificity(0.97, 96.43% and 100 % respectively) at a cut-off value of 35.93 ms. Figure 3 showed the ROC analysis results to distinguish AS-volunteers data from Early-OA patient data. In this case, Mean5 parameter showed comparatively highest AUC, sensitivity and specificity(0.96, 95% and 100 % respectively) at a cut-off value of 35.93ms. Figure 4 showed the ROC analysis results to distinguish Early-OA data from Risk-OA patient data. In this, MeanZ2 normalized parameter showed comparatively highest AUC, sensitivity and specificity(0.83, 87.5% and 60 % respectively) at a cut-off value of 1.22.DISCUSSION
From ROC analysis, the Mean3 parameter performance was slightly low in distinguishing AS-volunteers vs OA group as well as AS-volunteers vs Early-OA group, due to the presence of small focal lesion with increased T2 value in AS-volunteers group. In ROC analysis of AS vs OA and AS vs Early-OA, Mean5 parameter showed the highest AUC, specificity and sensitivity compared to other features. It might be due to the Mean5 was removed the bias effect in focal lesion having lower T2 relaxation times reported previously3. The proposed z-score analysis(MeanZ2) based on a new reference showed a better diagnosis accuracy for differentiating of Early-OA and Risk-OA category. The reason might be due to the degradation changes in Early-OA grades appeared focally(Figure 1.B), compared to Risk-OA(Figure 1.C), however MeanZ2 performance was poor in AS-volunteers vs Early-OA analysis due to the presence of similar biochemical characteristic in both AS-volunteers in Early-OA patients atleast 25% area of the cartilage tissue. One of the limitation of the study is the study sample was small.CONCLUSION
The present study showed that T2 mean selected between 45th to 55th percentile value provide improved differentiation between healthy and OA patients as well as Z-score normalization using T2mean less than 25th percentile reference provide improved differentiation between Early-OA and Risk-OA patients.Acknowledgements
This study was supported by IIT Delhi and Mahajan Imaging Centre Delhi. Authors would like to thank Vidur Mahajan, Vasantha K Venugopal, Ms. Madhuri Barnwal and Harsh Mahajan from Mahajan Imaging Centre for providing the required data.References
1. Li Z, Wang H, Lu Y, et al. Medicine (Baltimore). 2019 Jan; 98(1): e13834. doi:10.1097/MD.0000000000013834
2. Dunn TC, Lu Y, Jin H, Ries MD, Francisco S. Radiology.2015;232(2):592-598. doi:10.1148/radiol.2322030976.T2
3. Kaneko Y, Nozaki T, Yu H, Schwarzkopf R, Hara T. Journal of cliniimag.2019;(714):201-207. doi:10.1016/j.clinimag.2018.03.017.
4. Outerbridge RE, Frcs C. The Etiology of Chondromalacia Patellae. 1990;(C):5-8.
5. Thaha R, Jogi SP, Rajan S, et al. Proc. Intl. Soc. Mag. Reson. Med. 27 ( 2019), 4719.
6. Akhtar S, Poh CL, Kitney RI. Osteoarthr Cartil. 2007;15(9):1070-1085. doi:10.1016/j.joca.2007.03.009
7. Monu UD, Jordan CD, Samuelson BL, Hargreaves BA, Gold GE, Mcwalter EJ. Osteoarthr Cartil. 2017;25(4):513-520. doi:10.1016/j.joca.2016.09.015
8. D DWP, D MKP, D YLP, et al. Osteoarthr Cartil.2004:177-190. doi:10.1016/j.joca.2003.11.003
Figures