2689
Whole Body Composition in Patients Living with HIV1Department of Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States, 2Department of Medicine, University of California San Francisco, San Francisco, CA, United States, 3Department of Veterans Affairs, University of California San Francisco, San Francisco, CA, United States
Synopsis
HIV infection is associated with loss of subcutaneous adipose tissue, and the initiation of effective antiretroviral therapy has been associated with increased visceral adipose tissue (VAT). To quantify these changes in the body, MRI was used to image and conduct whole-body composition analysis. VAT was significantly higher in men with HIV infection than control males; there was little difference in females. In general, VAT ratio, the ratio of VAT to subcutaneous adipose tissue, was higher in patients living with HIV (PLWH) than controls. MRI is a quick, radiation-free alternative to DXA and CT in measuring whole-body composition in PLWH.
Introduction
The use of antiretroviral therapy (ART) has significantly reduced mortality rates in PLWH. However, as PLWH continue to live longer due to ART, the cause of increasing visceral adiposity has become of increasing concern in the aging HIV population. In addition, HIV-associated subcutaneous fat loss persists, despite newer ART that have fewer toxicities. Changes in body composition can be assessed using anthropometry and dual x-ray absorptiometry (DXA) (1,2,3). MRI Dixon is a newer method to measure whole body composition (WBC) in 3D without radiation. Thus, goal of this research was to employ MRI to assess differences in WBC in patients living with HIV (PLWH) vs healthy controls with a focus on gender differences.Methods
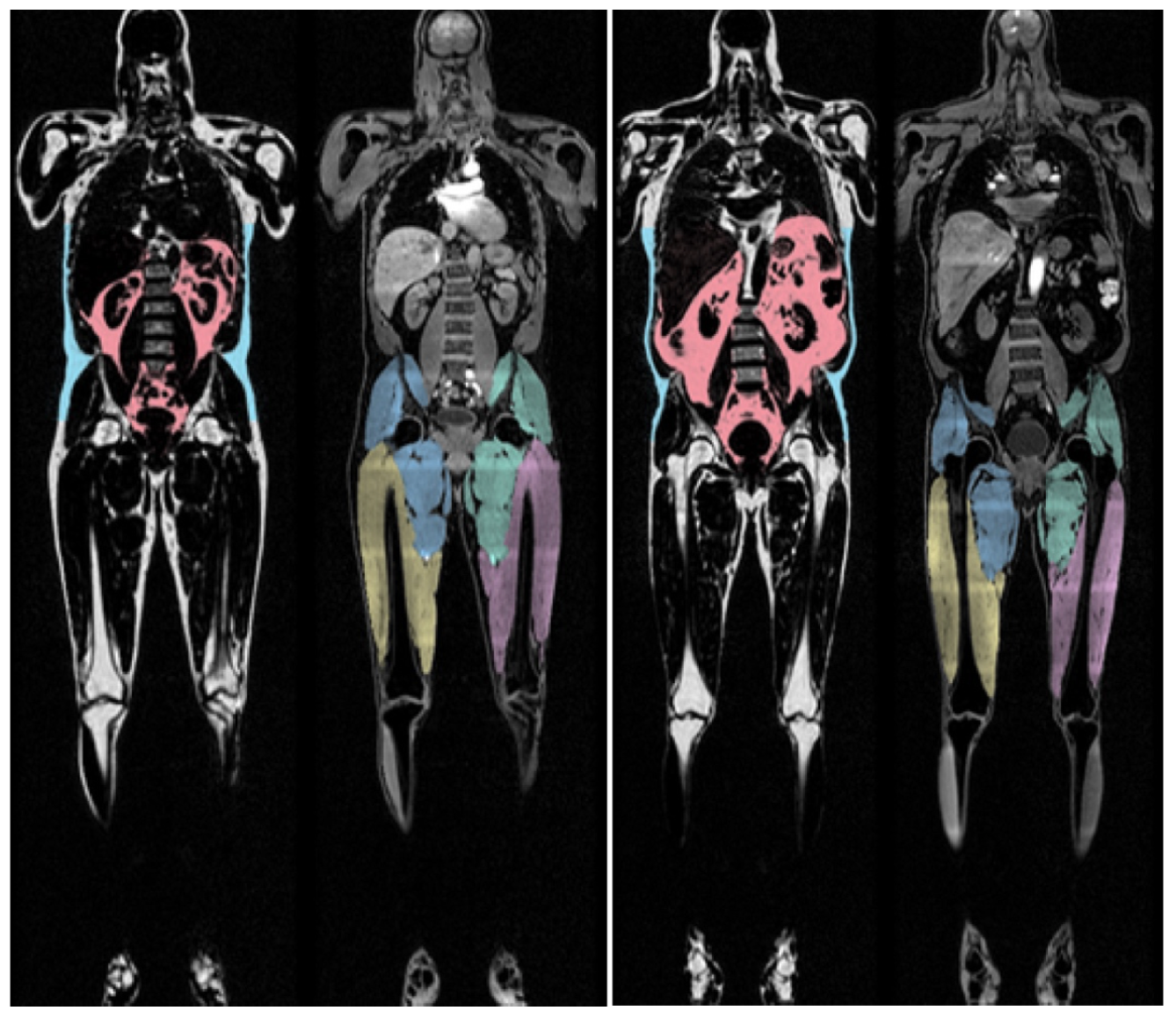
We enrolled 50 subjects (HIV=34, controls=16). Among the PLWH, we enrolled 25 men and 9 women. Among the controls, we enrolled 8 men and 8 women. We used a 3 Tesla MR wide bore system (MR750 GE Healthcare). The MRI protocol consisted of axial 2-point Dixon scans (LAVA-Flex) with FOV=50cm, Slice Thickness=3mm, matrix=160x160, flip angle=12, and 64 locations per slab. Each slab was acquired in 20 seconds and breath holding was performed in the abdominal area. Several slabs were acquired in order to cover the entire body from head to toe. The analysis was performed by AMRA Medical, Linköping, Sweden. Linear regression models (in all subjects and subdivided by gender) were used to assess the differences in VAT, ASAT, VAT ratio determined as VAT/(VAT+ASAT), total abdominal fat (VAT+ASAT), Fat index (total amount abdominal fat divided by height squared), thigh volume, and muscle ratio (body weight divided by thigh muscle volume). Regression models were adjusted for BMI and age.Results
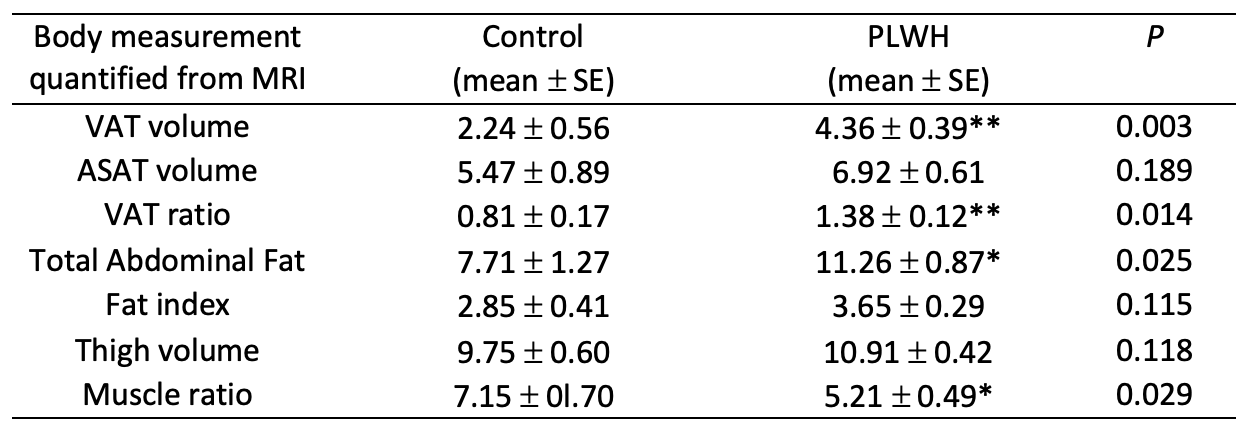
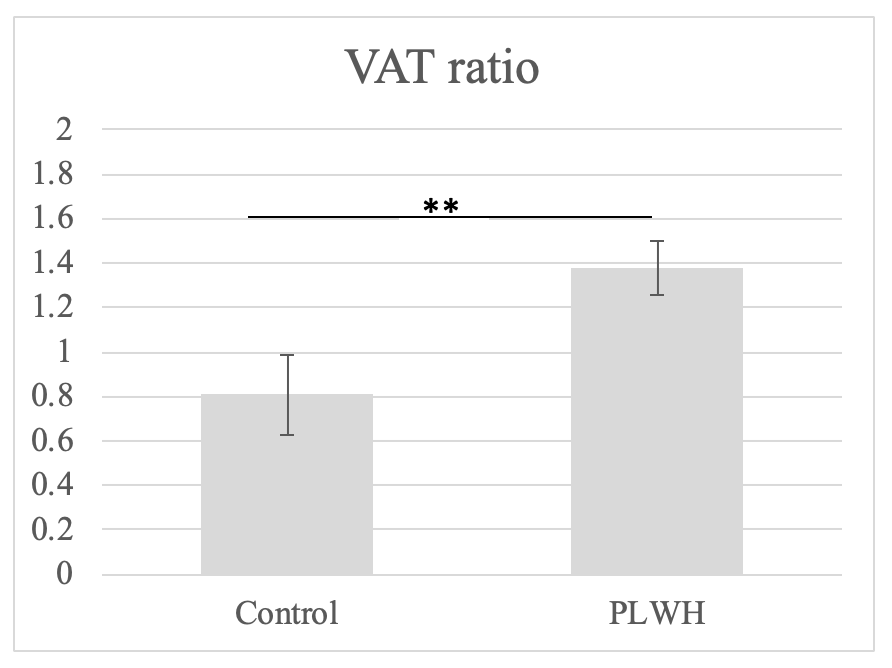
There were no significant differences between PLWH and controls in body mass index (BMI) or age (p>0.05). Referring to Table 1, PLWH had significantly higher VAT volume, VAT ratio, and total abdominal and significantly lower muscle ratio to control. Referring to Table 2, patients who were men had significantly higher VAT volume, total abdominal fat, and fat index than control men. Patients who were women had significantly higher thigh volume and significantly lower muscle ratio than control women (Table 2).Discussion
MRI has several advantages over DXA; it is a 3D method with high resolution and no radiation exposure. Furthermore, a whole-body MRI scan is very short (~5 minutes) and does not expose the patient to ionizing radiation can be added to any clinical exam; whole body composition by DXA takes 10 to 20 minutes and exposes the patient to radiation (4).In our contemporary cohort of PLWH and controls, we find that men with HIV have greater VAT than control men and little difference in ASAT, which is contrary to early HIV studies that found less ASAT in PLWH. In women, we did not observe this trend. Women had significantly higher thigh muscle volume instead which may be related to higher thigh muscle fat content. Differences in fat composition could be due to men’s fat storage being located in the abdomen whereas women’s primary fat storage is in gluteal-femoral tissues (5,6).
Future work will compare these MRI results with QCT, DXA and deuterated D3-creatine body composition assessments of the same cohort. Further, we will investigate changes in bone, muscle, and marrow adiposity in patients with HIV infection.
Conclusion
MRI based body composition scan is a non-invasive 3D assessment of the entire body in 5 minutes. Our results showed differences between PLWH and healthy controls as well as gender differences not previously reported. We are currently further increasing our enrollment.Acknowledgements
This research was funded by NIH/NIAID R01AI125080. The image analysis was done by AMRA Medical (Linköping, Sweden).References
1. Engelson ES, Kotler DP, Tan YX, et al. Fat distributtion in HIV-infected pateitns reporting truncal enlargment qunatified by whole-body magneitc resonance imaging. Am J Clin Nutr 1999:1162-9.
2. McDermott AY, Shevitz A, Knox T, Roubenoff R, et al. Effect of highly active antiretroviral therapy on fat, lean, and bone mass in HIV-seropositive men and women. Am J Clin Nutr. 2001;74(5):679-686.
3. Dinges, WL, Chen D, Snell PG, et al. Regional Body Fat Distribution in HIV-Infected Patients with Lipodystrophy. J Investig Med. 2005: 53(1):15-25.
4. Shepherd, J, Ng B, Sommer M, Heymsfield, SB. Body Composition by DXA. Bone. 2018: 104:101-105.
5. Blaak, E. Gender differences in fat metabolism. Curr Opin Clin Nutr Metab Care. 2001. 4(6):499-502.
6. Karastergiou K, Smith SR, Greenberg AS, Fried, SK. Sex differences in human adipose tissues- the biology of pear shape. Biol Sex Diff. 2012: 3: 13.
Figures