2683
Evaluation of Three Different Paradigms for Provoking Blood Oxygenation Level-Dependent MRI Signal Changes in Skeletal Muscles1Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China
Synopsis
Stress BOLD MRI allows for quantitative evaluation of blood flow reserve in skeletal muscles. In this study, we conducted a head-to-head comparison between three commonly used stressors including gas inhalation, cuff compression induced ischemia and postocclusive reactive hyperemia, and exercise. Results showed that different paradigms could produce different BOLD signal variation profiles. Both correlation and discrepancy can be noted regarding to the relationship between BOLD MRI and TcPO2 measurements. Ischemia and reactive hyperemia paradigm had better interobserver/interscan reproducibility, exercise had larger signal alterations, and both can reveal the age-dependent differences in BOLD signal and may be preferred in further applications.
INTRODUCTION
Stress blood oxygenation level-dependent (BOLD) MRI allows for quantitative evaluation of blood flow reserve in skeletal muscles. Several paradigms have been established as stressors including gas inhalation, cuff compression induced ischemia and postocclusive reactive hyperemia, and exercise.[1-4] To date, few studies have been performed to make direct comparisons among them. A recent investigation[5] showed better reproducibility for arterial spin labeling perfusion indices provoked by postocclusive reactive hyperemia when compared with exercise; however, the reported results for both paradigms were obtained in two separate subject cohorts. Therefore, the purpose of this study was to prospectively compare the three commonly used paradigms in skeletal BOLD MRI in healthy adults.METHODS
Twenty-two healthy volunteers including 12 young subjects (mean age, 22 years ± 0.9) and 10 elderly subjects (mean age, 58 years ± 5.0) were enrolled in the study from December 2017 to March 2018. None of the volunteers showed clinical manifestation of cardiovascular diseases. Three paradigms including gas inhalation, cuff compression induced ischemia and postocclusive reactive hyperemia, and exercise were sequentially performed, with a 15-min time interval between two neighboring protocols to avoid the interference from the preceding one.● In the gas inhalation paradigm, the inhalation of pure oxygen (100% O2) and a mixture of 5% CO2 and ambient air (5% CO2, 22% O2, and 73% N2) through an airtight mask with a gas reservoir and a one-way valve system was separately used to provoke BOLD signal alternations.
● Ischemia and postocclusive reactive hyperemia via arterial occlusion were induced in the lower extremity by a sphygmomanometer cuff tied around the middle of the thigh. Cuff compression was applied over 10 seconds to a pressure of 80 mm Hg above the individual systolic blood pressure and lasted for 300 seconds during the ischemic phase. Immediate cuff deflation was then performed within 5 seconds to record the postocclusive reactive hyperemic changes.
● A two-step supine plantar dorsiflexion exercise was used. First, the subjects were instructed to rhythmically dorsiflex the ankle by the maximum range of motion 60 times within one minute. Following that, plantar dorsiflexion was kept until exhaustion against the specific opposing resistance generated by a 4 kg sandbag attached to the subject’s upper foot with a string.
All subjects were imaged in the supine position on a 3-T MRI unit (HDxt; GE Healthcare, Waukesha, WI, USA) with an eight-channel cardiac coil. One 10-mm transverse section was positioned at the maximum calf diameter. BOLD MRI was performed using a multi-echo gradient-recalled echo sequence implementing the following parameters: repetition time/echo time, 51/(3.0–41.4) ms; 9 echoes with an echo spacing of 4.8 ms; flip angle, 15°; matrix, 288×192; field of view, 32×32 mm2; temporal resolution, 5 s/phase. Meanwhile, stress transcutaneous oxygen pressure (TcPO2) measurements were obtained and utilized as comparison to BOLD MRI.
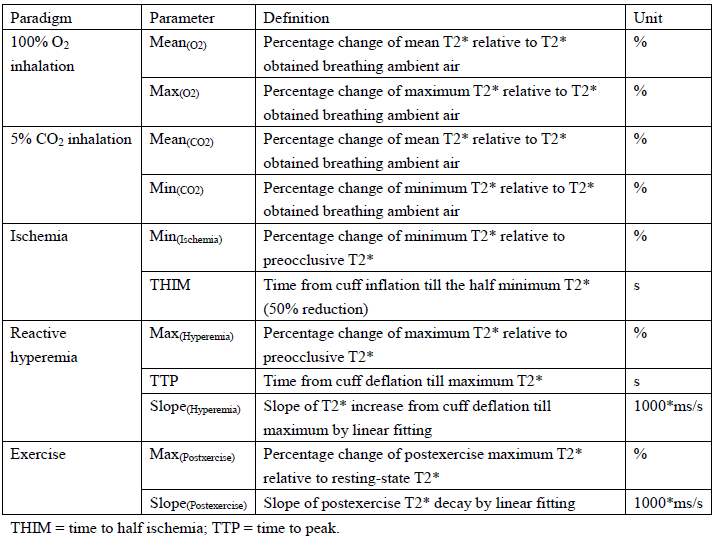
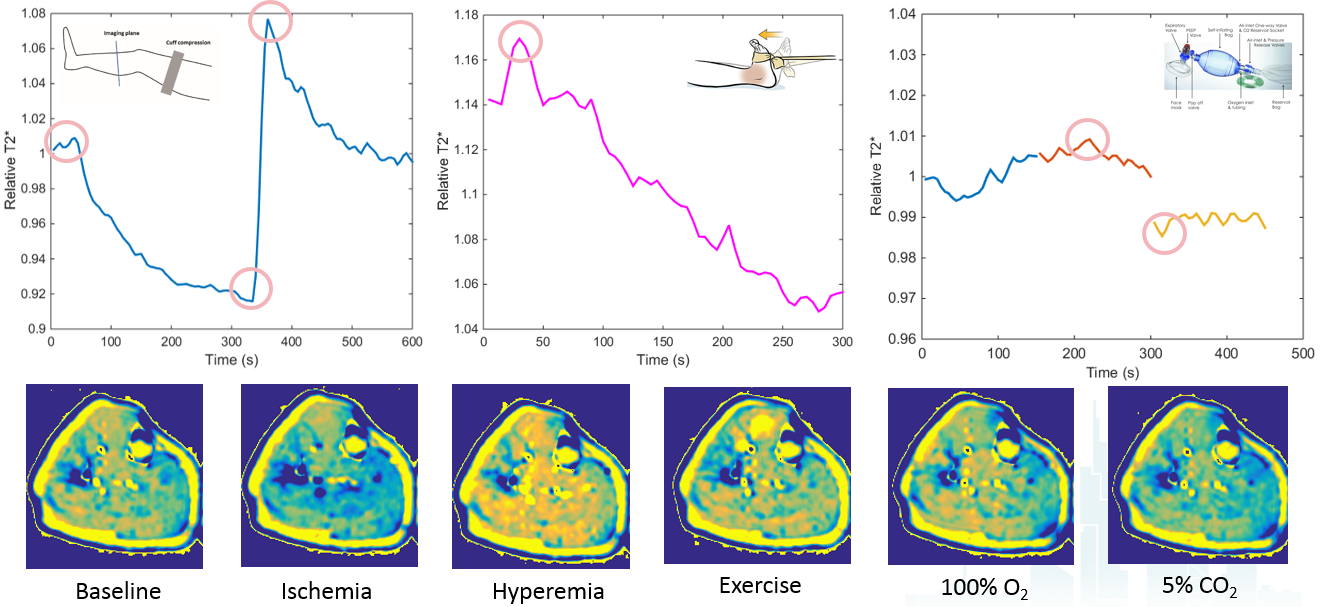
BOLD MRI T2* maps were generated and regions of interest (ROIs) were manually placed in five calf muscle compartments of each leg: anterior, lateral, deep posterior, soleus, and gastrocnemius. Signal intensity time curves were generated and quantitative parameters were calculated from the curves in each paradigm. Measurement reproducibility was assessed with intraclass correlation coefficients (ICCs). Differences in the maximal BOLD signal variation, the correlation with TcPO2, and the age-related change between paradigms were statistically analyzed.
RESULTS
Ischemia and reactive hyperemia paradigm derived Min(Ischemia) and Max(Hyperemia) showed the highest interobserver reproducibility (ICC, 0.993 and 0.985) and interscan reproducibility (ICC, 0.920 and 0.903). During O2 inhalation, a slightly lower BOLD T2* time course was observed compared with baseline though Max(O2)>1. During 5% CO2 inhalation, a much lower BOLD T2* time course was observed. In the occlusive ischemia period, BOLD T2* time course exhibited a steep initial decrease, typically followed by a less pronounced decrease until the end of the ischemic phase. After cuff deflation, BOLD T2* rapidly increased to the hyperemic peak value (generally higher than baseline) and subsequently decreased to a steady state gradually. After plantar dorsiflexion exercise, the BOLD T2* time course was attenuated from the peak value towards baseline in the anterior muscle group during the observation period.The Friedman test indicated significant differences in BOLD variation amplitudes of different paradigms in the anterior muscle group (P < 0.0001). The plantar dorsiflexion exercise paradigm elicited the largest BOLD T2* variation (15.48% ± 10.56%), followed by ischemia (8.30% ± 6.33%). Negligible to weak changes were observed during gas inhalation. Correlations with TcPO2 measurements were found in the ischemic phase (r = 0.966, P < 0.001) and in the postexercise phase (r = -0.936; P < 0.001). Min(Ischemia), Max(Hyperemia), Max(Postexercise) , and Slope(Postexercise) showed significant differences between young and elderly subject groups (all P < 0.01).DISCUSSION AND CONCLUSION
Different paradigms could produce different BOLD signal variation profiles. Specifically, the restimulated maximal BOLD signal changes and involved muscles vary among paradigms. Both correlation and discrepancy can be noted regarding to the relationship between BOLD MRI and TcPO2 measurements. Ischemia and reactive hyperemia and exercise paradigms can reveal the age-dependent differences in BOLD signal. Overall, Ischemia and reactive hyperemia or exercise paradigms may be preferred in further applications.Acknowledgements
This study was supported by the National Natural Science Foundation of China (grant No. 81701642) and Shanghai Science and Technology Committee (grant No. 18511102900/18511102901)References
1. Ledermann HP, Schulte AC, Heidecker HG, et al. Blood oxygenation level-dependent magnetic resonance imaging of the skeletal muscle in patients with peripheral arterial occlusive disease. Circulation. 2006;113:2929-2935.
2. Bajwa A, Wesolowski R, Patel A, et al. Blood Oxygenation Level-Dependent CMR-Derived Measures in Critical Limb Ischemia and Changes With Revascularization. J Am Coll Cardiol. 2016;67:420-431.
3. Noseworthy MD, Bulte DP, Alfonsi J. BOLD magnetic resonance imaging of skeletal muscle. Semin Musculoskelet Radiol. 2003;7:307-315.
4. Meyer RA, Towse TF, Reid RW, et al. BOLD MRI mapping of transient hyperemia in skeletal muscle after single contractions. NMR Biomed. 2004;17:392-398.
5. Lopez D, Pollak AW, Meyer CH, et al. Arterial spin labeling perfusion cardiovascular magnetic resonance of the calf in peripheral arterial disease: cuff occlusion hyperemia vs exercise. J Cardiovasc Magn Reson. 2015;17:23.
Figures