2682
Validation of a novel 64-channel coil for clinical high-resolution T2-weighted imaging of the upper leg1Department of Radiology and Nuclear Medicine, Amsterdam UMC, location AMC, Amsterdam, Netherlands, 2University of Twente, Enschede, Netherlands, 3Department of Biomedical Engineering and Physics, Amsterdam UMC, location AMC, Amsterdam, Netherlands, 4Academic Center for Evidence-based Sports medicine (ACES), Amsterdam UMC, location, Amsterdam, Netherlands, 5Magnetic Detection and Imaging (MD&I), University of Twente, Enschede, Netherlands
Synopsis
Hamstring strains are the most frequent injuries in elite football. Currently, it is not possible to accurately predict recovery or recurrence risk, which motivates the development of improved leg muscle imaging methods and hardware. A novel 64-channel upper leg coil was designed and compared to a conventional coil in healthy volunteers using two clinical high-resolution muscle T2-weighted sequences on 3T. The visibility of the anatomy and image quality were comparable to a conventional coil and scored clinically acceptable by experienced radiologists. The novel coil displayed an increased SNR of 31% which could be exploited to accelerate the imaging protocols.
Introduction
In elite football, hamstring injuries are the most frequent subtype of all injuries with a high incidence of 12% and a recurrence rate of 16% to 51%.1-3 Currently, hamstring strains are assessed by radiologists with ultrasonography (USG) or magnetic resonance imaging (MRI). However, neither USG nor conventional MRI are specific for the prediction of recovery and injury recurrence, which reveals the need for more advanced techniques.4 To address this limitation, an upper leg coil was designed to improve muscle fiber imaging. Before clinical application, at least a comparable performance in clinical MR imaging is required. Therefore, in this work the performance of the novel coil was compared to a conventional coil in clinical high resolution T2 sequences.Method
Eight healthy volunteers (four females, mean age 22.6 years, range: 21-24 years) were scanned in two sessions using the different coils within a 4-week period (mean of 8.1 days between sessions, range: 0-14 days).The scanning was performed at a 3T MRI scanner (Philips Ingenia, Best, The Netherlands). Participants were positioned feet first in a supine position and scanned once with a 16-element conventional receive coil in combination with 10 elements from a tabletop receive coil, and once with the 64-element upper leg receive coil (Figure 1). The scanning protocol included a coronal T2-weighed (T2W) Dixon (water, fat and in-phase) sequence, covering the hamstrings from knee to hip, and an axial T2W turbo spin-echo (TSE) sequence. The T2W TSE sequence was acquired in three multi-slice stacks to cover the whole upper legs, to account for the B0 inhomogeneity of the scanner in the axial direction.
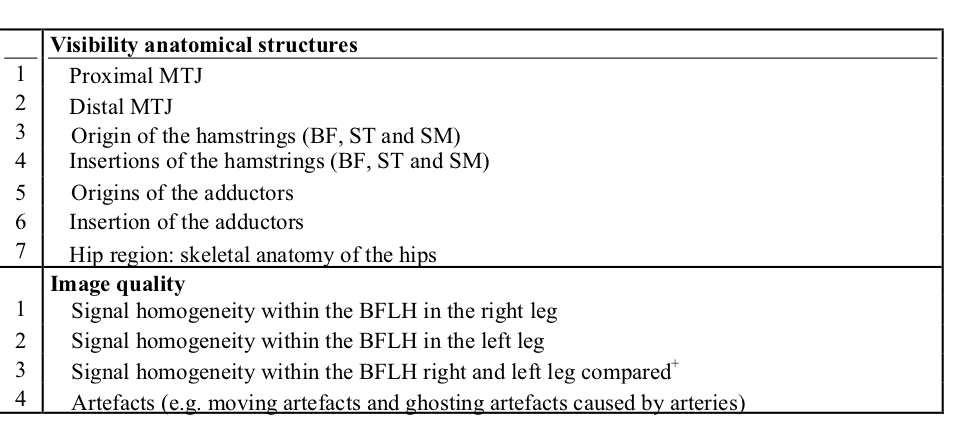
Two radiologists with experience in musculoskeletal imaging and sports radiology, separately evaluated the MR images from the two coils. Both the T2W Dixon images and the T2W TSE were used. Eleven parameters were divided in the visibility of anatomical structures (7) and the image quality (4), specified in Table 1. The visibility was scored with a 4-point Likert scale (1: not visible; 2: poorly visible; 3: moderately visible, but clinically acceptable, 4: visible and clinically acceptable), and the image quality with a 3-point Likert scale (1: low image quality, no clinical value; 2: clinically acceptable, 3: good image quality). The inter-rater agreement was calculated using Cohen’s kappa. Additionally, the percental agreement (P0) was calculated.
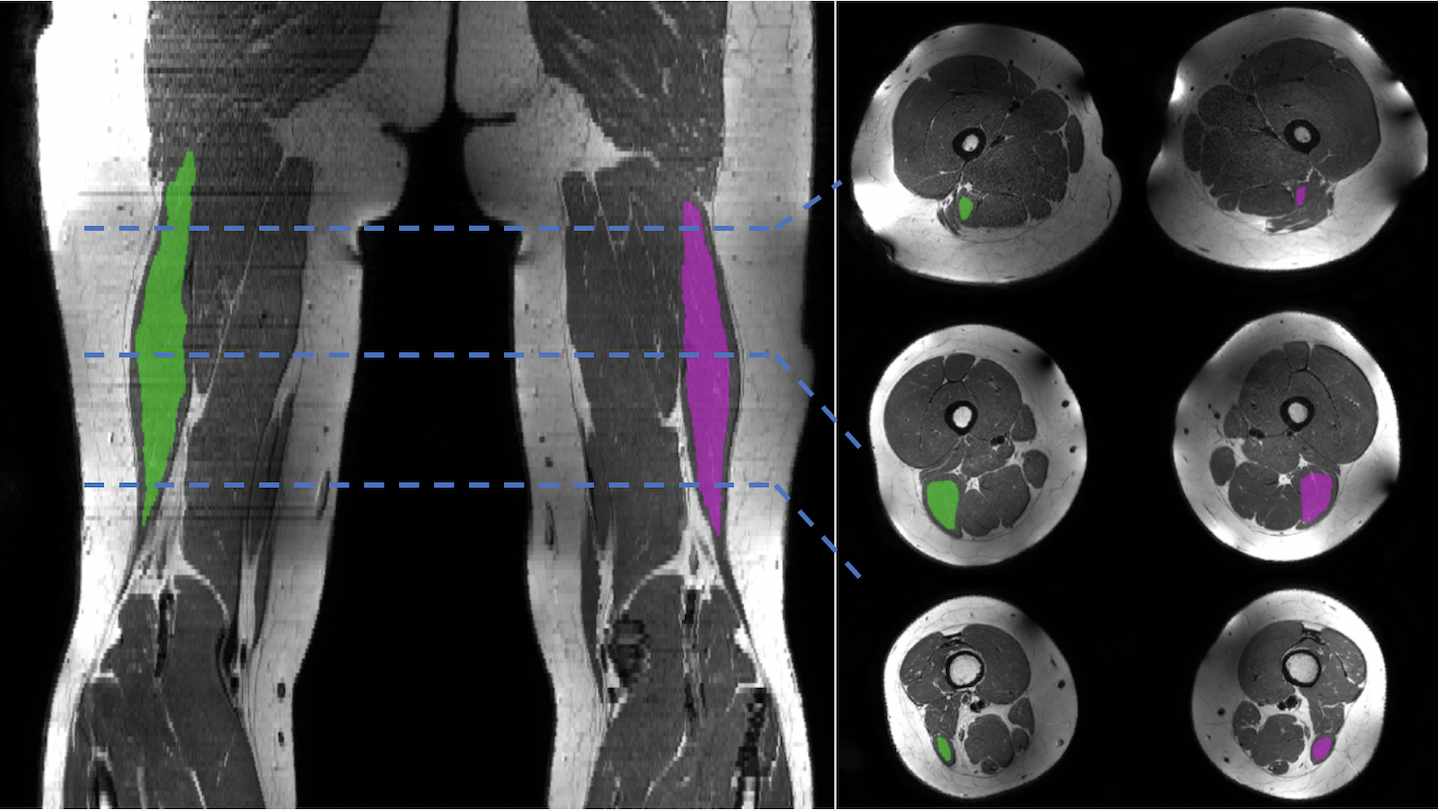
A 3D region of interest (ROI) of the biceps femoris long head (BFLH) was manually segmented on the T2W TSE images (see Figure 2). Within the segmentations the SNR of the T2W TSE images was calculated for each leg and coil. The SNR was calculated by dividing the mean muscle signal by the standard deviation (SD) of the muscle signal, assuming the signal within a muscle to be homogeneous. For comparison between the upper leg coil and the conventional coil, the Wilcoxon signed-ranked test was used (p < 0.05 was considered significant).
Results
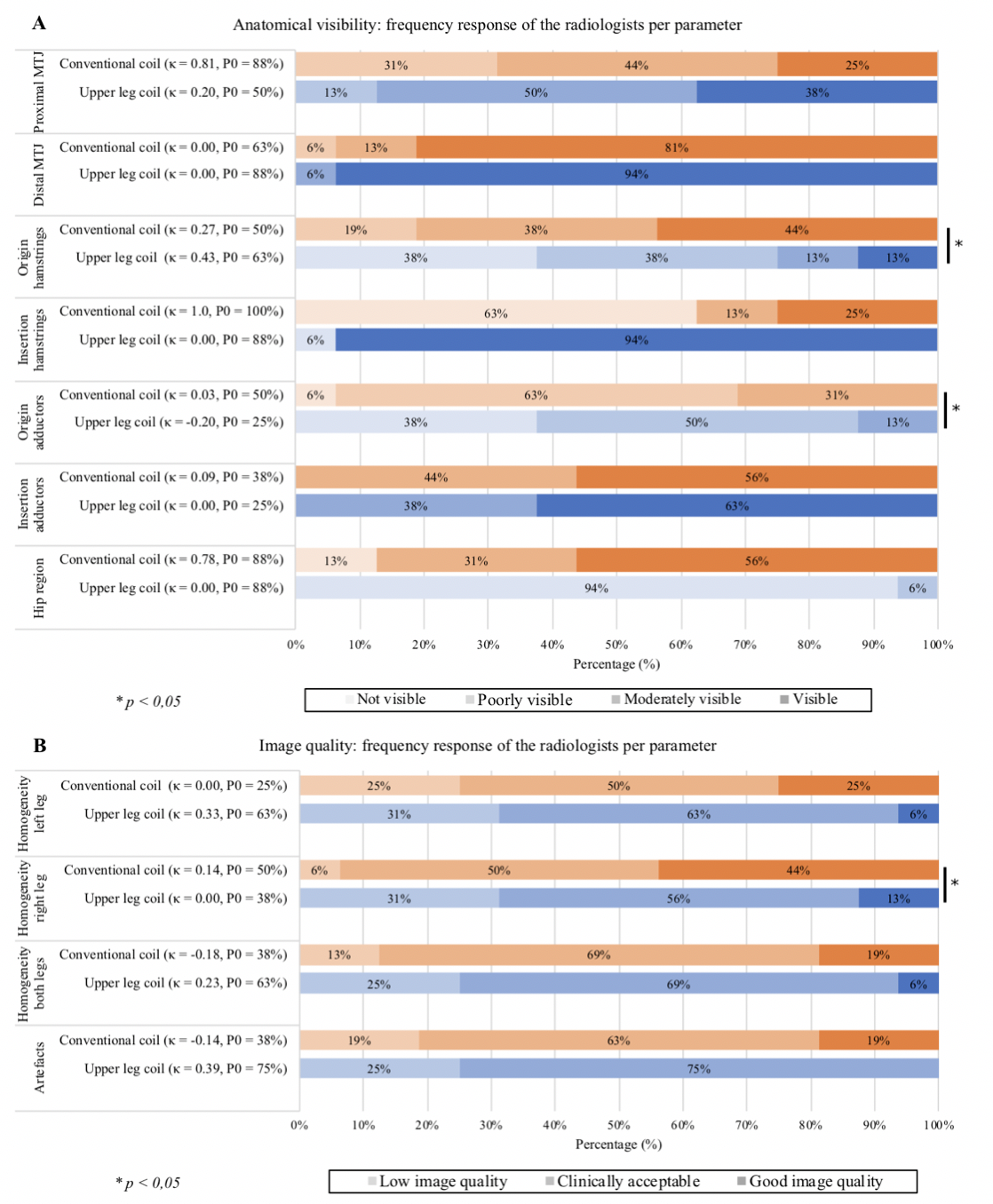
In Figure 3 the Likert scoring for each parameter is presented. The upper leg coil showed no difference (p = 0.244) between the scores in the proximal MTJ (88% upper leg coil vs. 69% was scored as 3 and 4, Figure 3a). The distal MTJ (p = 0.180) as well as in the insertion of the adductors (p = 0.655) showed equal results. For both the origin of the hamstrings (p = 0.002) and the origin of the adductors (p = 0.046), the conventional coil scored significantly higher. The insertion of the hamstrings in the conventional coil and the hip region in the novel coil had low scores.For the image quality a significantly higher homogeneity was found in the right BFLH with the conventional coil (p = 0.038, Figure 3B). The other three image quality parameters showed equal results between the two coils.
A significant increase of mean SNR (31%) was found in the left BFLH in the upper leg coil (p = 0.017). No significant increase (25%) was found in the right BFLH (p = 0.160).
Discussion
In the proximal and distal MTJ and the insertion of the adductors, the upper leg coil had a comparable performance in the clinical T2 sequences. However, the insertion of the hamstrings and the hip region were not fully imaged resulting in lower scores. The hip region was added for the completeness but is not the primary focus of the upper leg coil. The origins of the hamstrings and adductors were scored significantly higher in the conventional coil. Further post processing, such as image intensity homogenization, could be used to further improve the image quality in future research.The increased SNR in both the left (31%) and right BFLH (25%), proves an increased signal quality within the hamstring muscles that could result into improved trauma determination. This increased SNR can also be used to accelerate image acquisition with the upper leg coil, which would benefit clinical practice.
Conclusion
In high resolution T2 sequences, the novel upper leg coil shows comparable visibility to the conventional coil for 7 out of 11 parameters. Proximal imaging of the muscle origins would benefit from additional postprocessing. The upper leg coil displayed an increased SNR which could be exploited to accelerate the imaging protocols.Acknowledgements
No acknowledgement found.References
1. J. Ekstrand, M. Hagglund, and M. Walden, “Epidemiology of muscle injuries in professional football (soccer).,” Am. J. Sports Med., vol. 39, no. 6, pp. 1226–1232, Jun. 2011.
2. J. Ekstrand, J. C. Healy, M. Walden, J. C. Lee, B. English, and M. Hagglund, “Hamstring muscle injuries in professional football: the correlation of MRI findings with return to play.,” Br. J. Sports Med., vol. 46, no. 2, pp. 112–117, Feb. 2012.
3. C. Carling, F. Le Gall, and E. Orhant, “A Four-Season Prospective Study of Muscle Strain Reoccurrences in a Professional Football Club,” Res. Sport. Med., vol. 19, no. 2, pp. 92–102, Mar. 2011.
4. A. Guermazi, F. W. Roemer, P. Robinson, J. L. Tol, R. R. Regatte, and M. D. Crema, “Imaging of Muscle Injuries in Sports Medicine: Sports Imaging Series.,” Radiology, vol. 282, no. 3, pp. 646–663, Mar. 2017.
Figures