2640
Second-order Motion Compensated Intravoxel Incoherent Motion Analysis of the Kidney1Radiology Division, Kanazawa University Hospital, Ishikawa, Japan, 2Faculty of Health Sciences, Institute of Medical, Pharmaceutical and Health Sciences, Kanazawa University, Ishikawa, Japan, 3Philips Japan, Tokyo, Japan, 4Department of Radiology, Kanazawa University Graduate School of Medical Sciences, Ishikawa, Japan
Synopsis
To investigate the potential benefit of second-order motion compensated (2nd-MC) diffusion encoding scheme on intravoxel incoherent motion (IVIM) analysis of the kidney, we compared the IVIM diffusion parameters and repeatability between the 2nd-MC and conventional diffusion gradients. Our results showed that the 2nd-MC diffusion gradients show better fitting accuracy and repeatability of IVIM diffusion parameters of the kidney compared with the conventional diffusion gradients. Therefore, the 2nd-MC diffusion encoding scheme could enable us to reduce the bulk motion effect mainly caused by cardiac and respiratory motion during diffusion sensitization.
INTRODUCTION
Intravoxel incoherent motion (IVIM) analysis of the kidney provides both perfusion and diffusion information and is useful to assess renal function and classify renal tumor.1,2 However, the clinical application of the IVIM analysis is still hampered by the low measurement accuracy and repeatability. One possible reason for this limitation is bulk motion mainly caused by cardiac and respiratory motion during diffusion sensitization, resulting in signal loss.3 Previous studies have reported that second-order motion compensated (2nd-MC) diffusion encoding scheme reduced the bulk motion sensitivity in cardiac diffusion MRI.4.5 Therefore, to investigate the potential benefit of the 2nd-MC diffusion encoding on IVIM analysis of the kidney, we compared the IVIM diffusion parameters and repeatability between 2nd-MC and conventional diffusion encoding schemes.METHODS
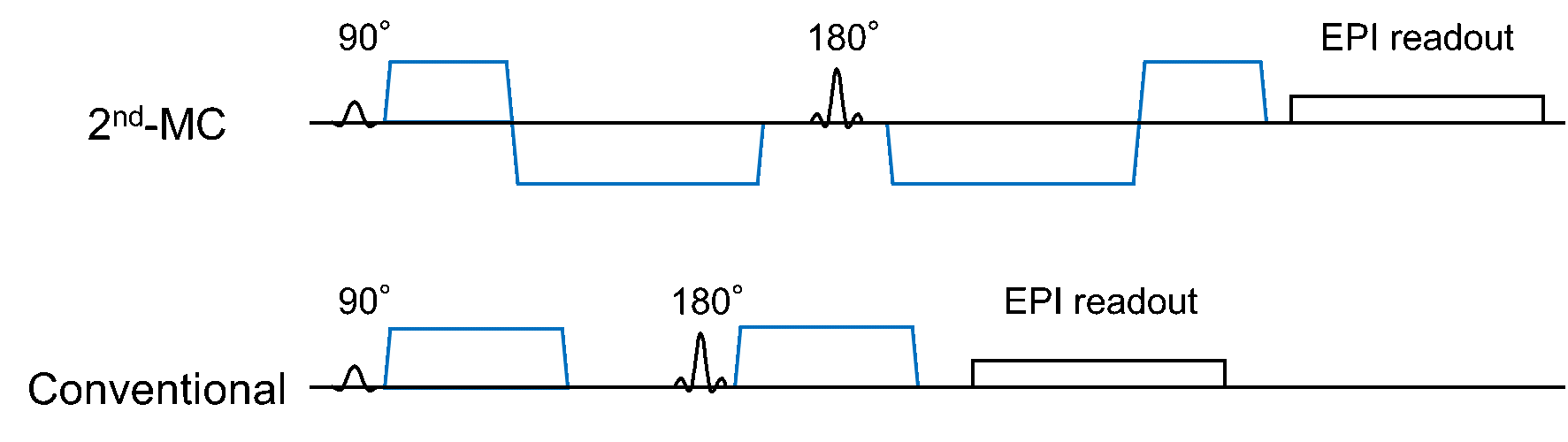
On a 3.0-T MRI, coronal diffusion-weighted images of the kidney were obtained in eight healthy volunteers (all men; mean age, 25.4 ± 3.8 years) using respiratory-synchronized single-shot diffusion echo-planar imaging with the 2nd-MC and conventional diffusion gradients (Fig. 1). The imaging parameters were as follows: repetition time, one respiration cycle; echo time, shortest (83-85 ms for 2nd-MC and 50-52 ms for conventional diffusion gradients); acquisition matrix, 96 × 119; b-values, 0, 10, 30, 50, 100, 200, 400, 600, and 800 s/mm2; field of view, 300 mm; slice thickness, 7 mm; number of signals averaged, 2; and sensitivity encoding factor, 2. All subjects were asked to fast for at least 6 hours before the scan. The same scan was repeated twice to assess the repeatability of the measurements. We determined mean signal intensities in the renal cortex and medulla at each b-value. Then, perfusion-related diffusion coefficient (D*), the fraction (F), and restricted diffusion coefficient (D) were calculated from biexponential fitting. Normalized root mean square errors (nRMSE) were obtained to assess the fitting quality.6 Repeatability coefficients (RC) were calculated from Bland-Altman plots to assess the repeatability of diffusion parameters. These values were compared between the 2nd-MC and conventional schemes.RESULTS AND DISCUSSION
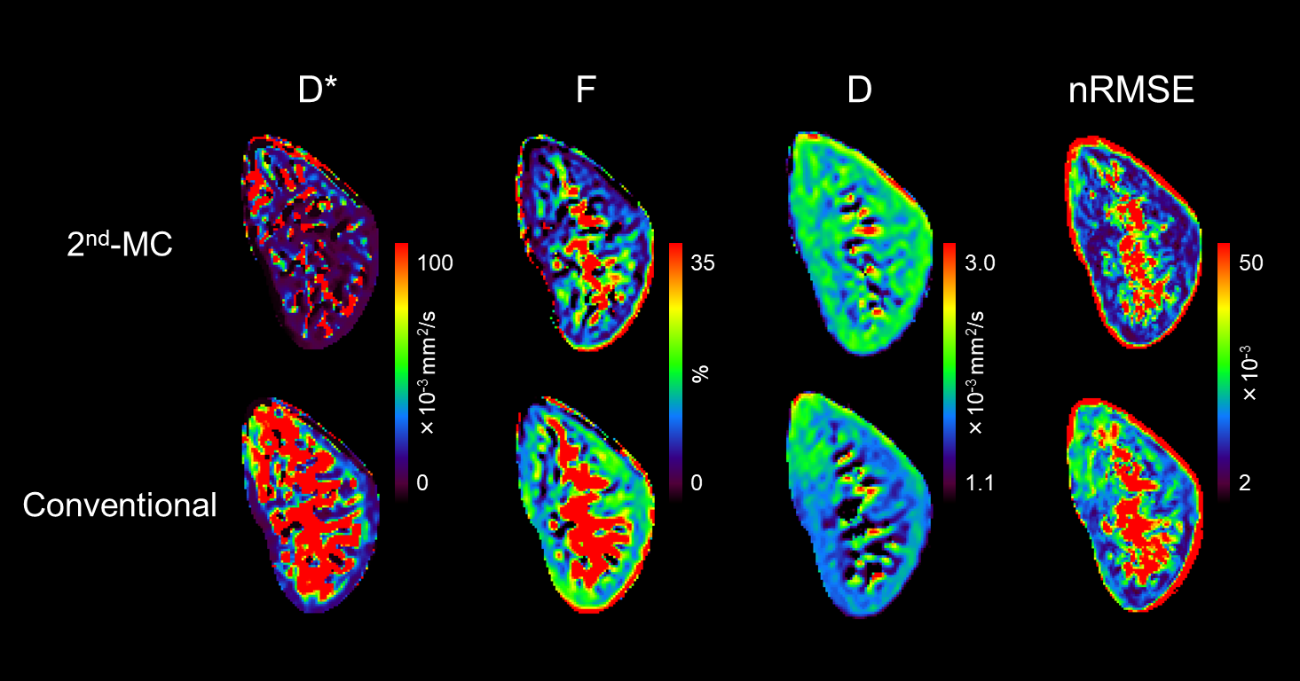
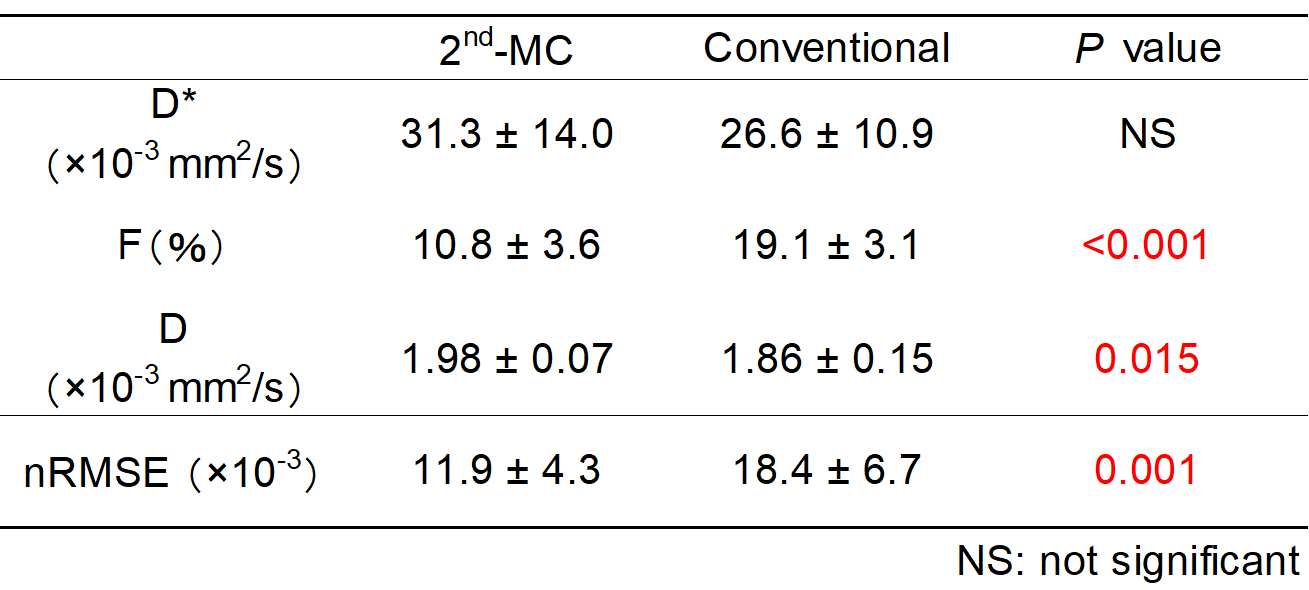
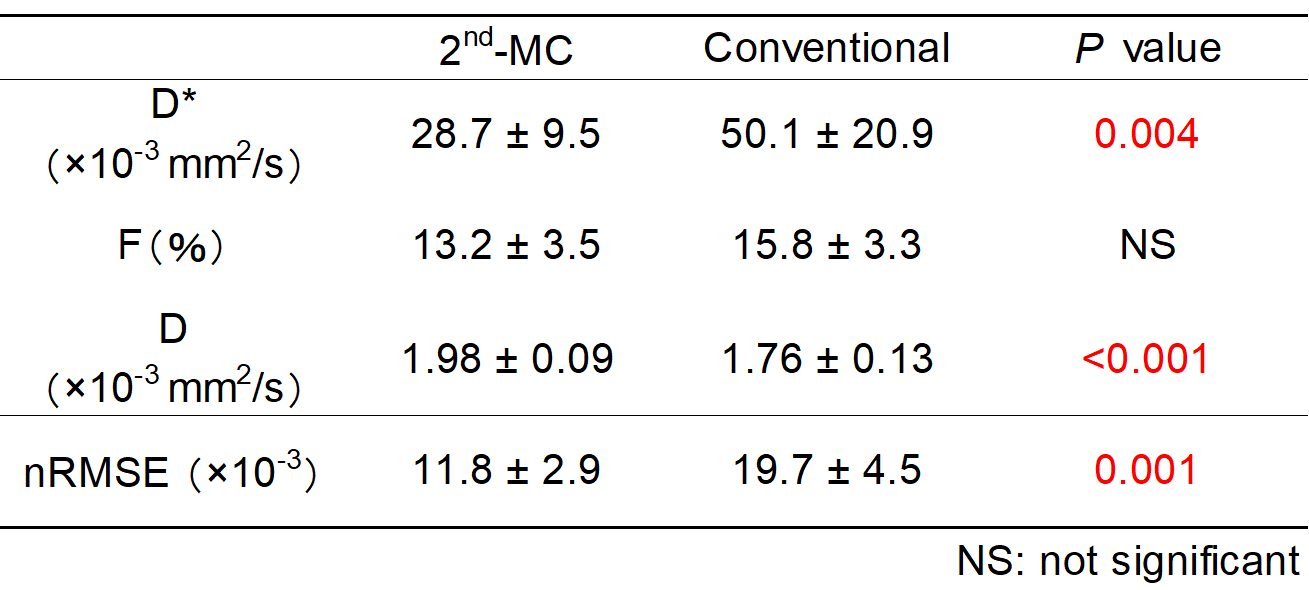
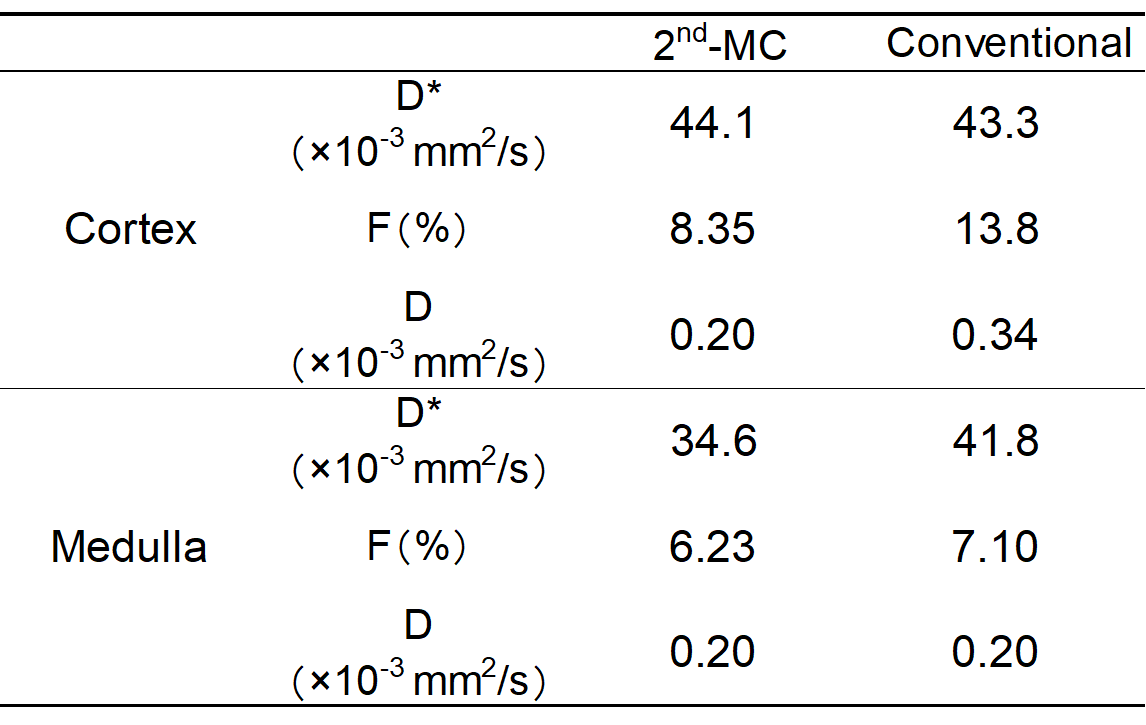
Tables 1 and 2 show the results of IVIM diffusion parameters and nRMSE with 2nd-MC and conventional diffusion gradients in the renal cortex and medulla, respectively. Representative images of diffusion parameters and nRMSE with both schemes are presented in Figure 2. The F in the cortex and D* in the medulla with the 2nd-MC were significantly lower than those with the conventional diffusion gradients. These results could be explained by the difference in signal attenuation caused by coherent motion and flow between the 2nd-MC and conventional diffusion gradients. The cortical and medullary D with the 2nd-MC were significantly higher than those with the conventional diffusion gradients. This may be due to the dependence of restricted diffusion on the difference in the diffusion encoding waveform between both schemes. Moreover, the nRMSE in the cortex and medulla significantly reduced when using the 2nd-MC diffusion gradients, suggesting improved fitting accuracy. Table 3 shows the RC of diffusion parameters with both schemes. The 2nd-MC diffusion gradients showed better repeatability for D and F in the cortex and D* and F in the medulla compared with the conventional diffusion gradients.CONCLUSION
The 2nd-MC diffusion gradients show better fitting accuracy and repeatability of IVIM diffusion parameters of the kidney compared with the conventional diffusion gradients.Acknowledgements
No acknowledgement found.References
1. Gaing B, et al. Subtype differentiation of renal tumors using voxel-based histogram analysis of intravoxel incoherent motion parameters. Invest Radiol. 2015; 50: 144-152.
2. Bane O, et al. Assessment of renal function using intravoxel incoherent motion diffusion-weighted imaging and dynamic contrast-enhanced MRI. J Magn Reson Imaging. 2016; 44: 317-326.
3. Jerome NP, et al. Comparison of free-breathing with navigator-controlled acquisition regimes in abdominal diffusion-weighted magnetic resonance images: Effect on ADC and IVIM statistics. J Magn Reson Imaging. 2014; 39: 235-240.
4. Nguyen C, et al. In vivo diffusion-tensor MRI of the human heart on a 3 tesla clinical scanner: An optimized second order (M2) motion compensated diffusion-preparation approach. Magn Reson Med. 2016; 76: 1354-1363.
5. Aliotta E, et al. Convex optimized diffusion encoding (CODE) gradient waveforms for minimum echo time and bulk motion-compensated diffusion-weighted MRI. Magn Reson Med. 2017; 77: 717-729.
6. Lv J, et al. Performance of U-net based pyramidal lucas-kanade registration on free-breathing multi-b-value diffusion MRI of the kidney. Br J Radiol. 2018; 91: 20170813.
Figures