2619
Retrospective respiratory and cardiac gating in abdominal diffusion-weighted imaging1Department of Diagnostic and Interventional Radiology, Technical University of Munich, Munich, Germany, 2Philips Healthcare, Best, Netherlands
Synopsis
Diffusion-weighted imaging (DWI) remains a valuable tool in abdominal lesion detection. However, respiratory and cardiac motion remain major effects confounding the robustness of abdominal DWI. Respiratory triggering and prospective gating techniques are typically employed to reduce the effect of respiratory motion on abdominal DWI. However, these techniques can become either inefficient or result in artifacts in patients with irregular breathing patterns. In addition, cardiac triggering further reduces the SNR efficiency of a respiratory triggered acquisition. The purpose of the present work is to develop an algorithm for combined retrospective gating of abdominal DWI based on recorded respiratory and cardiac signals.
Purpose
Diffusion-weighted imaging (DWI) remains a valuable tool in abdominal lesion detection and there is an ongoing interest in ADC mapping for tumor staging and therapy monitoring1. However, respiratory and cardiac motion remain major effects confounding the robustness of abdominal DWI. Respiratory triggering and prospective gating techniques are typically employed to reduce the effect of respiratory motion on abdominal DWI. However, respiratory triggering and prospectively gated techniques can become either inefficient or result in artifacts in patients with irregular breathing patterns. In addition, cardiac triggering further reduces the SNR efficiency of a respiratory triggered acquisition2. Retrospective respiratory and cardiac gating techniques would enable the sorting of DW images based on where the image was acquired on the respiratory and cardiac cycle3,4. However, combined retrospective respiratory and cardiac gating has not been yet thoroughly explored in abdominal diffusion imaging using recorded physiology signals. The purpose of the present work is to develop an algorithm for combined retrospective gating of abdominal DWI based on recorded respiratory and cardiac signals.Methods
MR MeasurementIn-vivo experiments were carried out in 5 healthy subjects by using the traditional Stejskal-Tanner diffusion encoding waveform. Imaging parameters included: acquisition voxel size = 3.3 x 3.3 x 3.3 mm3; 52 slices placed over the liver; 3 orthogonal diffusion encoding directions at b-values of [0, 500] s/mm2 and averages of [6, 20]; TE/TR = 58/4385 ms. The scans were performed in free breathing and had a scan time of 4 minutes and 53 seconds for all subjects. All experiments were performed on a 3T scanner (Philips Ingenia Elition, Best, The Netherlands).
Retrospective Respiratory and Cardiac Gating Pipeline
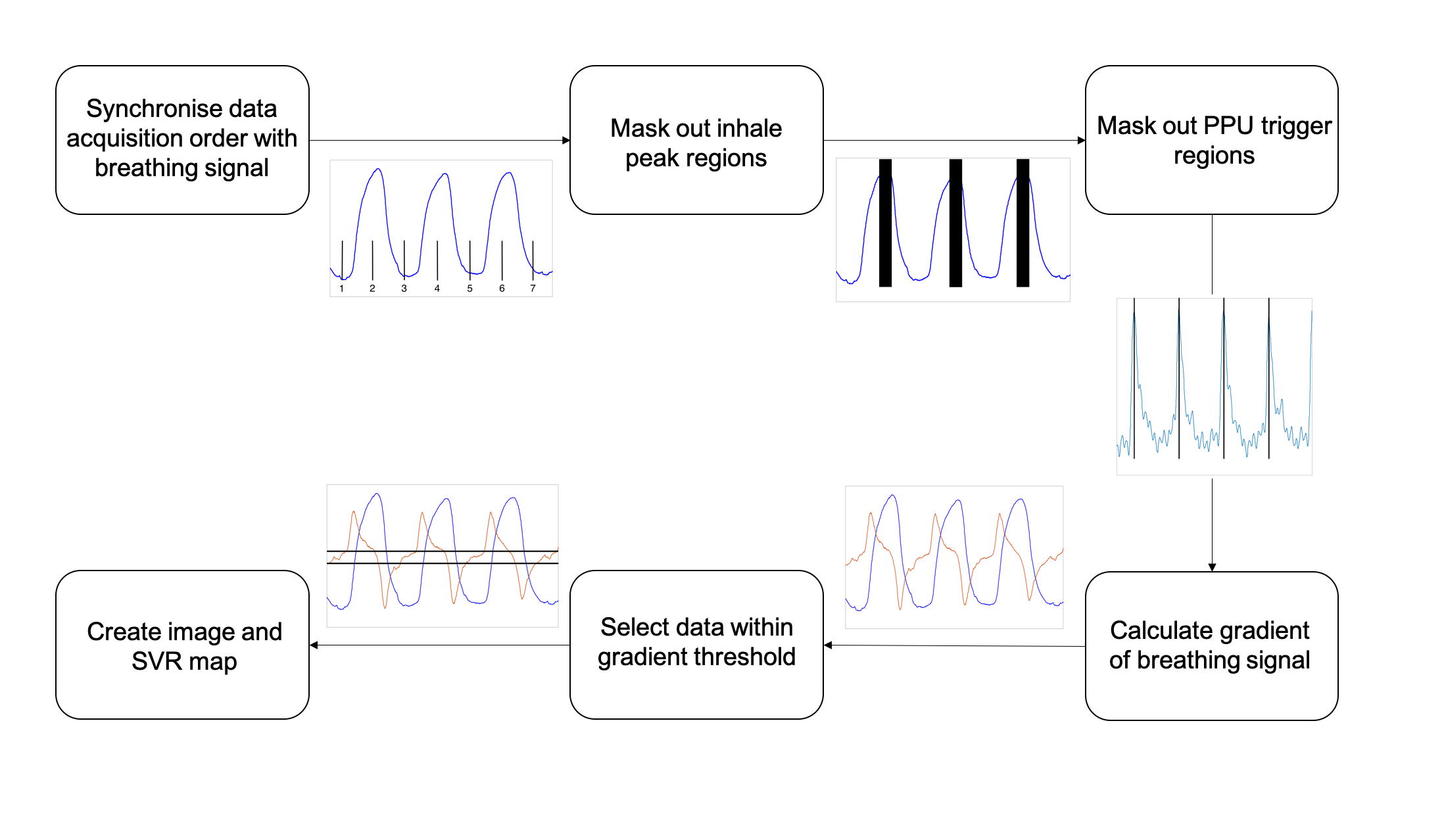
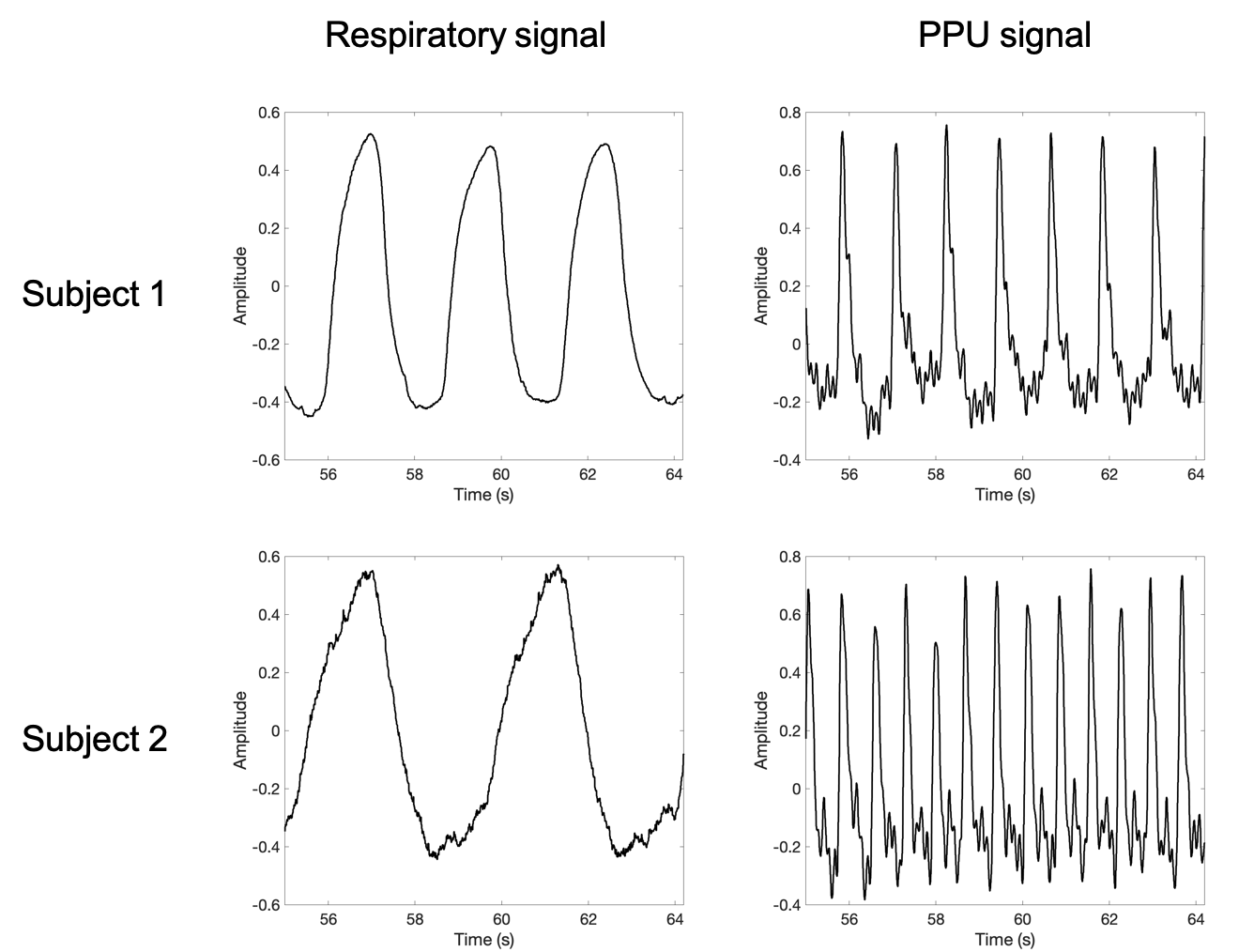
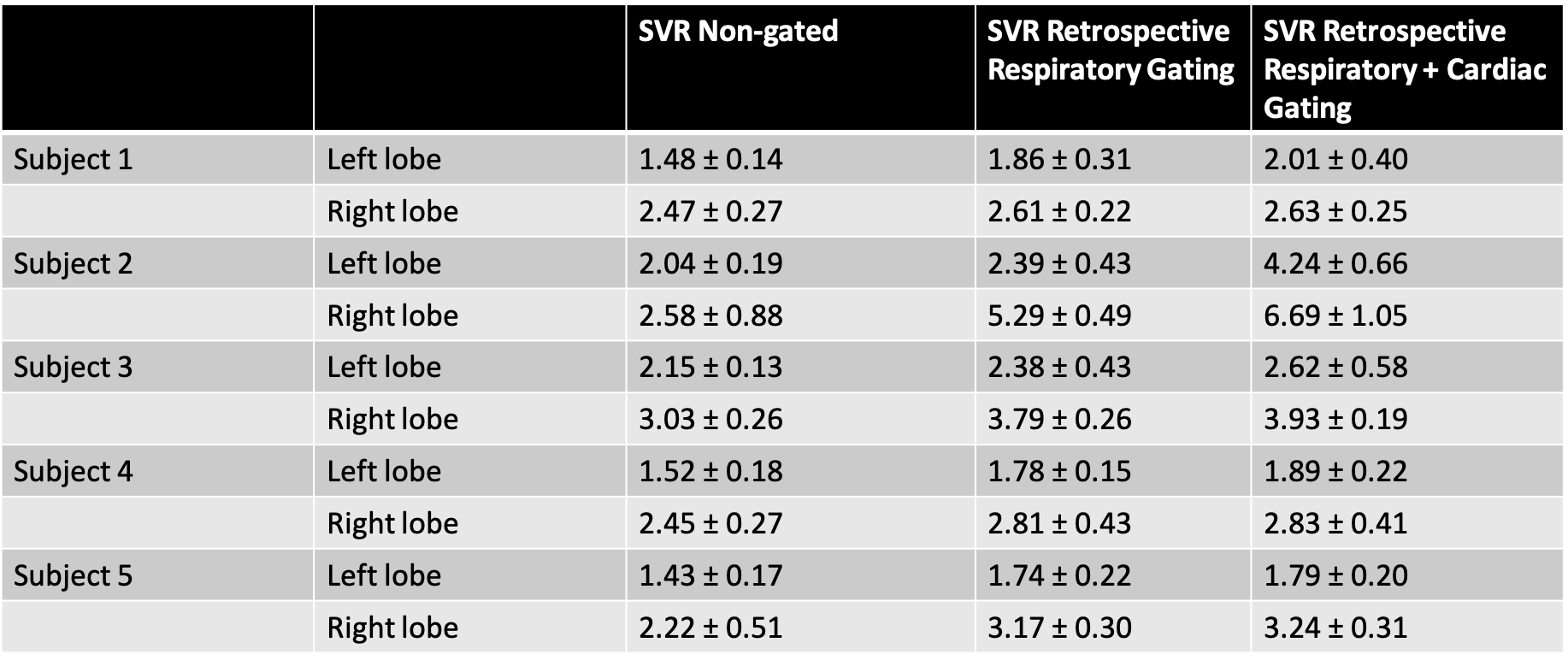
Figure 1 shows the retrospective respiratory and cardiac gating pipeline. The signals from the respiratory belt and peripheral pulse unit (PPU) were recorded and synchronised with the order in which the data was acquired. The time intervals around the peaks of the inhale periods and around the PPU triggers were masked out. The PPU trigger mask interval was estimated empirically from the data, and also took into account the delay between the actual heartbeat and the detection of the pulse from the PPU. Breathing curves from two subjects are shown in Figure 2 along with the corresponding PPU signal. Since a typical breathing curve has a sinusoidal like shape, the gradient of the recorded respiratory motion signal should be close to zero at the bottom of the exhale period and at a maximum during inhalation or exhalation. Therefore, a minimum threshold was set for the magnitude of the gradient of the respiratory motion signal and data was filtered out based on the computed gradient values. DW-images were then averaged based on the qualifying data, and signal variation ratio (SVR) maps were computed by dividing the image intensity by the standard deviation of the data used to form the image on a pixel by pixel basis. Two ROIs per slice in 3 adjacent slices in both the left and right liver lobes were drawn in order to calculate the mean SVR, as shown in Figure 5.
Results
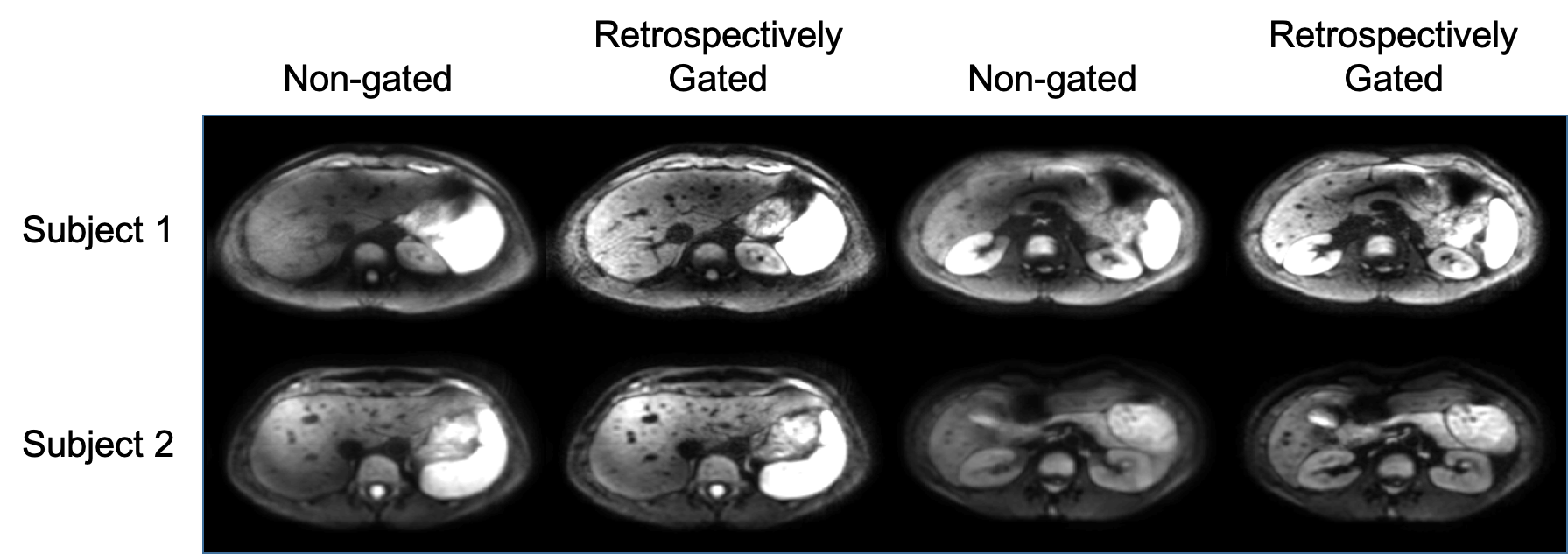
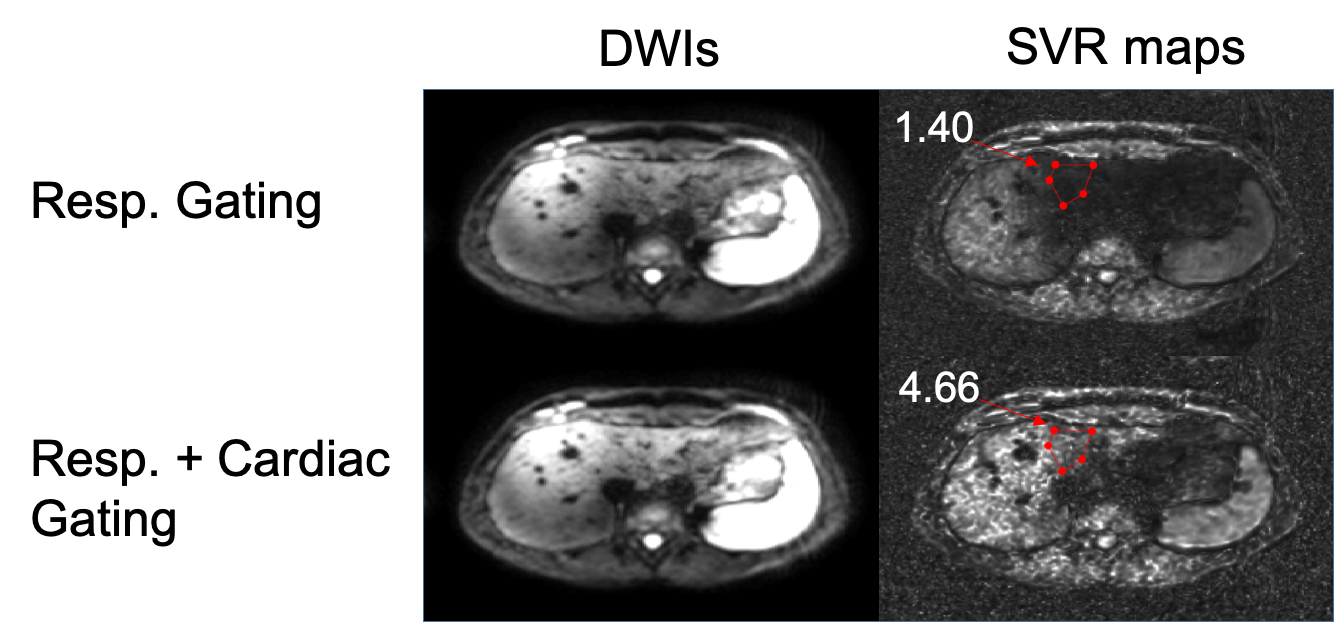
Figure 3 shows a comparison between non-gated and retrospectively gated DWIs at b=500s/mm2 for 2 subjects. In both cases, the non-gated images were blurry and the retrospectively gated images were much sharper, especially when looking at vessels in the liver and the borders of the pancreas. Figure 4 shows the effect of taking the PPU signal into account when compared with only respiratory gating. The cardiac and respiratory gated image was brighter overall, especially in areas which are typically affected by cardiac pulsation, like the left liver lobe. The SVR over the drawn ROI was lower when using only respiratory gating compared to when using both respiratory and cardiac gating. Figure 5 shows the mean SVR over ROIs drawn in the left and right liver lobes for 5 subjects. The respiratory and cardiac gated images typically showed the highest SVR in both regions, the non-gated images showed the lowest SVR and the images that were only respiratory gated showed values in between those of the other two methods.Discussion & Conclusion
The proposed combined retrospective respiratory and cardiac gating method can improve the image quality and the SVR of diffusion weighted images when compared to non-gated methods, and could be a viable alternative to prospectively triggered scans. However, if the quality of the recorded respiratory signal is low, the ability of the proposed method to select the appropriate data can be compromised. Retrospective respiratory gating could be improved by using alternative methods to record the respiratory motion signals, for example by using optical sensors5-7.Acknowledgements
The present research was supported by Philips Healthcare and the German Research Foundation (DFG824/A9).References
1. Irina Heid, Katja Steiger, Marija Trajkovic-Arsic, et al. Co-clinical Assessment of Tumor Cellularity in Pancreatic Cancer, Clin Cancer Res March 15 2017 (23) (6) 1461-1470; DOI: 10.1158/1078-0432.CCR-15-2432
2. Metens T, Absil J, Denolin V, Bali MA, Matos C. Liver apparent diffusion coefficient repeatability with individually predetermined optimal cardiac timing and artifact elimination by signal filtering, J Magn Reson Imaging. 2016 May;43(5):1100-10. doi: 10.1002/jmri.25089. Epub 2015 Nov 13.
3. Murphy P, Wolfson T, Gamst A, Sirlin C, Bydder M. Error model for reduction of cardiac and respiratory motion effects in quantitative liver DW-MRI. Magn Reson Med. 2013 Nov;70(5):1460-9. doi: 10.1002/mrm.24563. Epub 2012 Dec 27.
4. Christian Dávid, Thomas Vahle, Robert Grimm, Peter Bachert and Marc Kachelrieß. Motion Compensation for Free-Breathing Diffusion-Weighted Imaging (MoCo DWI), Proc. Intl. Soc. Mag. Reson. Med. 27 (2019) Abstract 3397
5. Sascha Krueger, Julien Sénégas, Daniel Wirtz, Marek Bartula, Vincent Jeanne, Thiru Kanagasabapathi, and Ger Kersten. Optical unobtrusive physiology sensor for respiratory-triggered MRI acquisitions, Proc. Intl. Soc. Mag. Reson. Med. 26 (2018) Abstract 2529
6. Joseph Y. Cheng, Jonathan Lu, Grieg Scott, and Shreyas S. Vasanawala. Optical Motion Monitoring for Abdominal and Lung Imaging, Proc. Intl. Soc. Mag. Reson. Med. 25 (2017) Abstract 3936
7. Julien Sénégas, Sascha Krueger, Daniel Wirtz, Ger Kersten, Mukul Rocque, Ivan E. Dimitrov, Andrea J. Wiethoff, Keith Hulsey, Ivan Pedrosa, and Ananth J. Madhuranthakam. Comparison of liver motion measured by dynamic MRI and respiration signals obtained by an optical sensor. Proc. Intl. Soc. Mag. Reson. Med. 26 (2018) Abstract 2528
Figures