2611
Body Diffusion MR Imaging with Compressed SENSE Based on Single-Shot EPI at 3T and 1.5T: Technical Feasibility and Initial Clinical Experience1Faculty of Medicine, RWTH Aachen University, Aachen, Germany, 2Diagnostic and Interventional Radiology, University Hospital RWTH Aachen, Aachen, Germany, 3Kumamoto University Hospital, Kumamoto, Japan, 4Graduate School of Medical Sciences, Kumamoto University, Kumamoto, Japan, 5Philips Japan, Tokyo, Japan, 6Philips GmbH DACH, Hamburg, Germany
Synopsis
Compressed sensing technologies have recently become commercially available that serve the purpose to shorten the image acquisition time for morphological imaging. Here we explore the reconstruction algorithm that allows the combination of wavelet transformation of compressed sensing with coil information of sensitivity encoding (SENSE) in body diffusion MRI based on 2D single-shot EPI and uniform undersampling, and report our results in both healthy volunteers and patients on both 3T and 1.5T, in comparison to the conventional SENSE parallel imaging technique.
Introduction
Compressed sensing is a new and promising technique to accelerate the imaging process by reconstruction of a magnetic resonance (MR) image from non-uniformly undersampled k-space data 1. The clinical benefit in morphological imaging with combination of sensitivity encoding coil information has been recently described 2. We aimed to investigate the technical feasibility and clinical utility of employing compressed sensing reconstruction in two-dimensional (2D) single-shot echo-planar imaging (EPI) with a uniform k-space undersampling strategy in body diffusion MR imaging on both 3T and 1.5T, with comparison to the conventional parallel imaging reconstruction.Methods
All human subjects underwent MRI on a 3T and 1.5T systems (Ingenia, Philips, Best, the Netherlands). Body diffusion MRI was performed using 2D multi-slice single-shot echo-planer imaging (EPI) sequences in the liver, prostate and breast. Conventional parallel imaging was done using sensitivity encoding (SENSE). For compressed sensing, uniform k-space undersampling was applied and the subsampled data were reconstructed with a combination of wavelet transformation and SENSE coil information (compressed SENSE or C-SENSE) 2. While spatial resolution and b-value were adapted for each anatomy, most imaging parameters were kept the same between conventional SENSE and compressed SENSE. Detailed imaging parameters were summarized in Table 1.For image analysis, visual assessment was performed for all anatomies. In addition, quantitative assessment was done for comparison of the signal-to-noise ratio (SNR) and apparent diffusion coefficient (ADC) in liver diffusion-weighted EPI (DW-EPI) of healthy volunteers on 1.5T. For SNR measurement additional noise maps were acquired without radio frequency (RF) excitation for each DW-EPI scan. Regions of interest (ROIs) were selected in the liver parenchyma with uniform signal without vessels or artifacts as well as in the corresponding noise map. The same criteria of ROI selection also applied to ADC quantification. Values were reported in mean and standard deviation (SD). For statistics paired t-test was used and a p value <0.001 was considered significant.
Results and Discussion
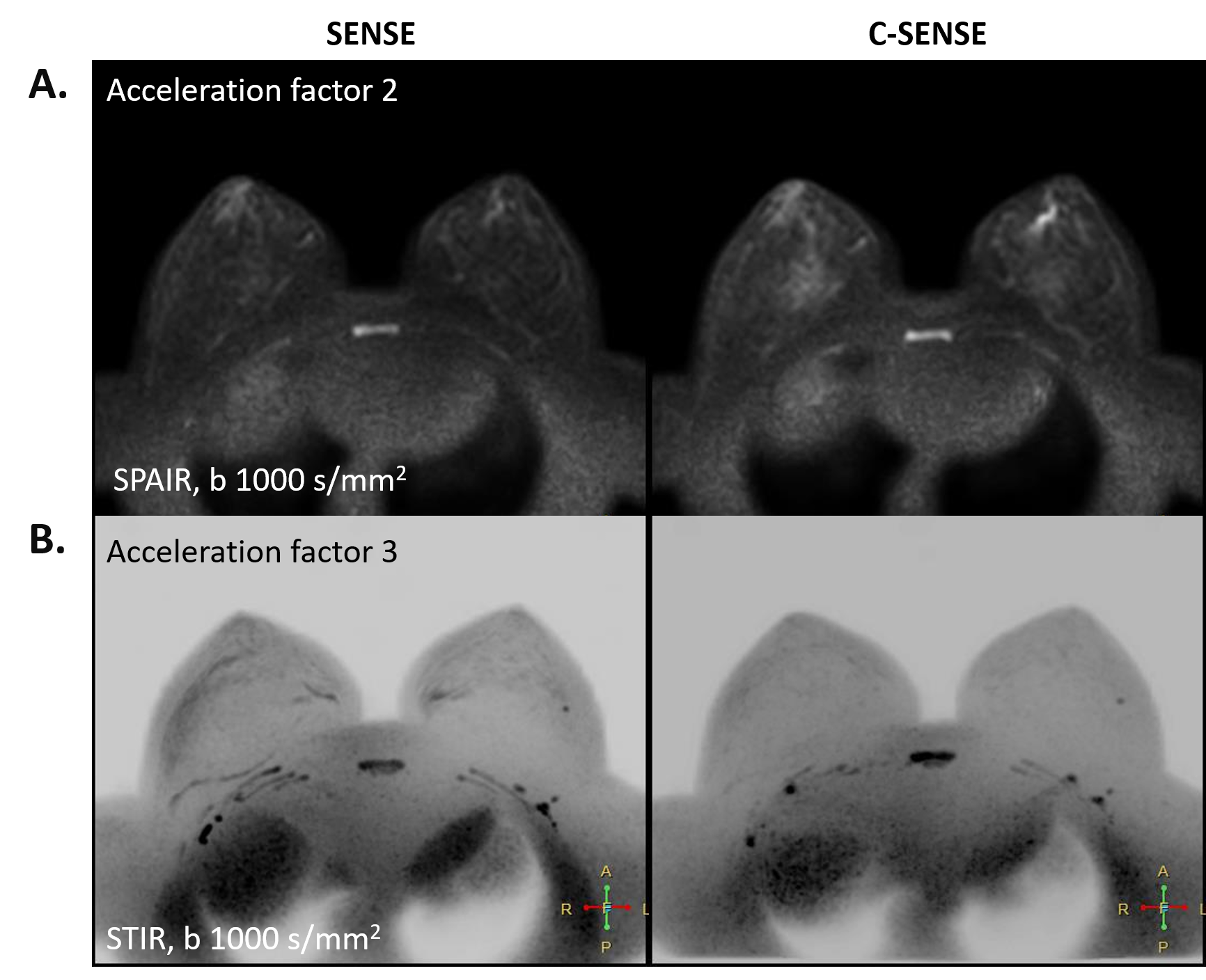
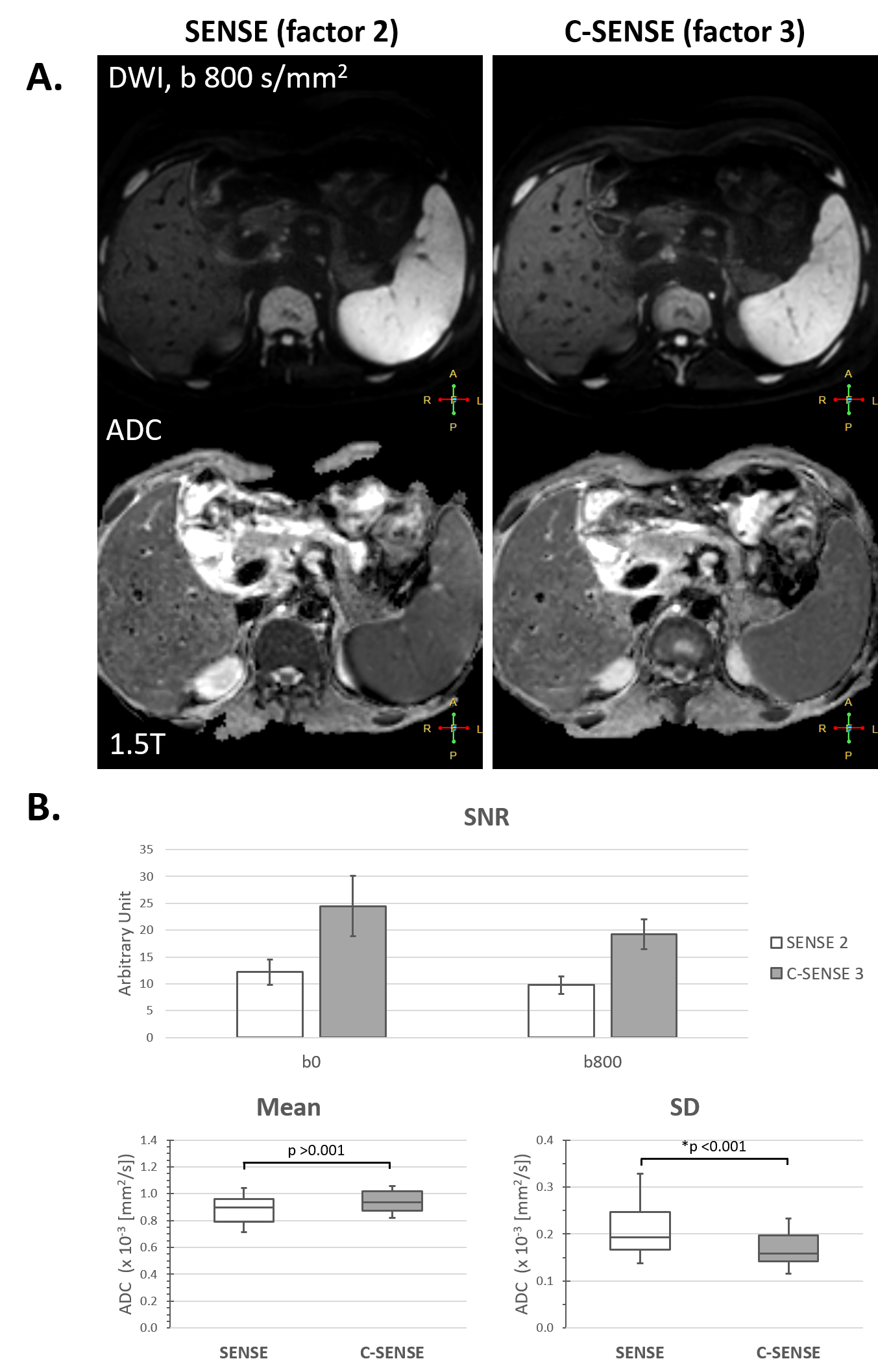
12 healthy volunteers (32 ± 7 years [mean ± SD], 6 female) and 10 patients (54 ± 14 years, 3 female) were included. In general, reduced background noise and clearer structural delineation can be visualized with C-SENSE reconstruction, compared to conventional SENSE. This applied to all three anatomies on both field strengths. Selected examples are presented in Figure 1 to 3. In particular, C-SENSE clearly reduced the noise in the center of the SENSE-based DWI (arrows in Figure 1 and 2), which was associated with g-factor penalties and thus obscured an accurate lesion detection and cancer interpretation. This improvement most likely benefits from the iterative de-noising process in the wavelet domain, in which the noise patterns are sparsely represented.For liver DW-EPI, imaging with different C-SENSE acceleration factors was conducted. Typical results with a C-SENSE factor of 3 were shown in Figure 4A. In comparison to conventional SENSE with a factor of 2, SNR measurement showed almost a two-fold benefit for both b values of 0 and 800 s/mm2. On the other hand, while ADC quantification revealed similar values between C-SENSE and conventional SENSE (p = 0.006), the former presented a significantly lower SD than that of the latter (p < 0.001) (Figure 4B). This lower variability may again attribute to a higher signal in the C-SENSE images and may indicate a higher precision and reproducibility in ADC assessment. Such quantitative findings were in consistency with the qualitative observation above and were also in accordance to the previous reports 3,4. While further studies of its clinical performance are warranted, a systematic investigation in different undersampling variants, noise behaviors and image quality characteristics may help to identify standardized approaches for determining optimal imaging parameters in clinical routine exams 5.
Conclusion
2D multi-slice single-shot EPI can be combined with the recently introduced compressed SENSE technology for body diffusion MRI. Though uniformly undersampled, the results have shown that an iterative de-noising process in the wavelet domain in combination with coil sensitivity may help not only in shortening image acquisition but also in image quality improvement, compared to the conventional SENSE reconstruction. The achieved better SNR and less variable ADC may benefit lesion detection in various applications, and this needs to be further investigated in clinical studies with larger cohorts.Acknowledgements
The authors thank Stephanie Tackenberg, Lucia Noël und Dega Abdi for their helps in image acquisition.References
- Lustig M, et al. Magn Reson Med (2007) 58:1182
- Sartoretti E et al. Plos One (2019) 14:e0214887.
- Yoneyama M, et al. ISMRM, Montreal (2019) 27:1634.
- Morita K, et al. ISMRM, Montreal (2019) 27:3355.
- Zijlstra F et al. Invest Radiol (2016) 51:410.
Figures
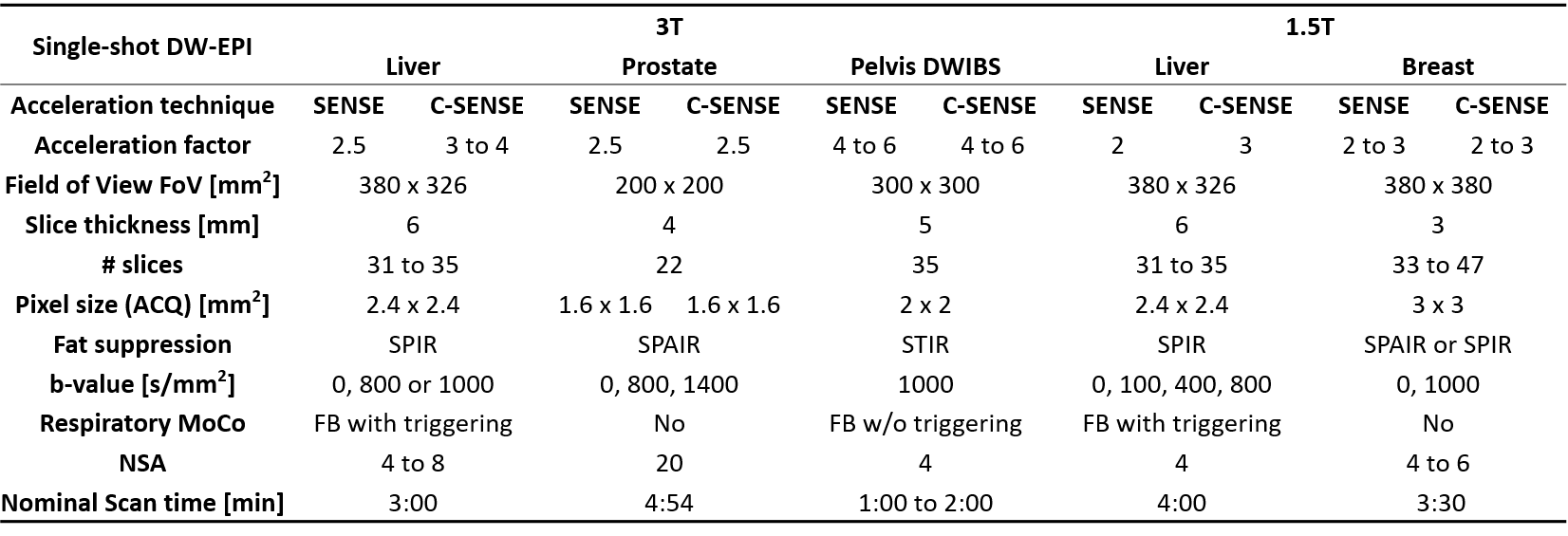
Table 1. Imaging parameters of body DW-EPI on 3T and 1.5T.
EPI = echo planner imaging; FB = free breathing; NSA = number of signal averaging; ACQ = acquired; MoCo = motion compensation
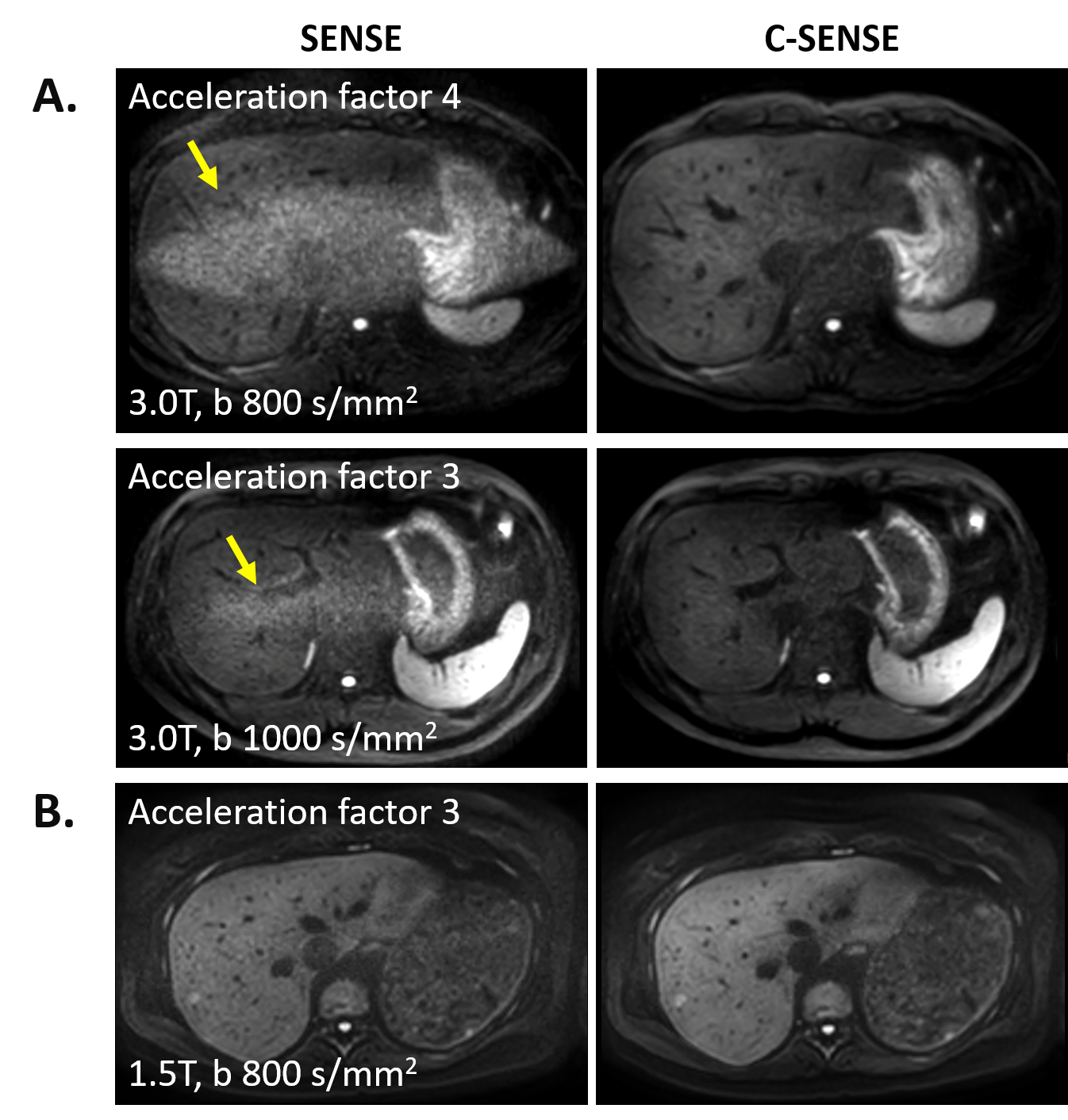
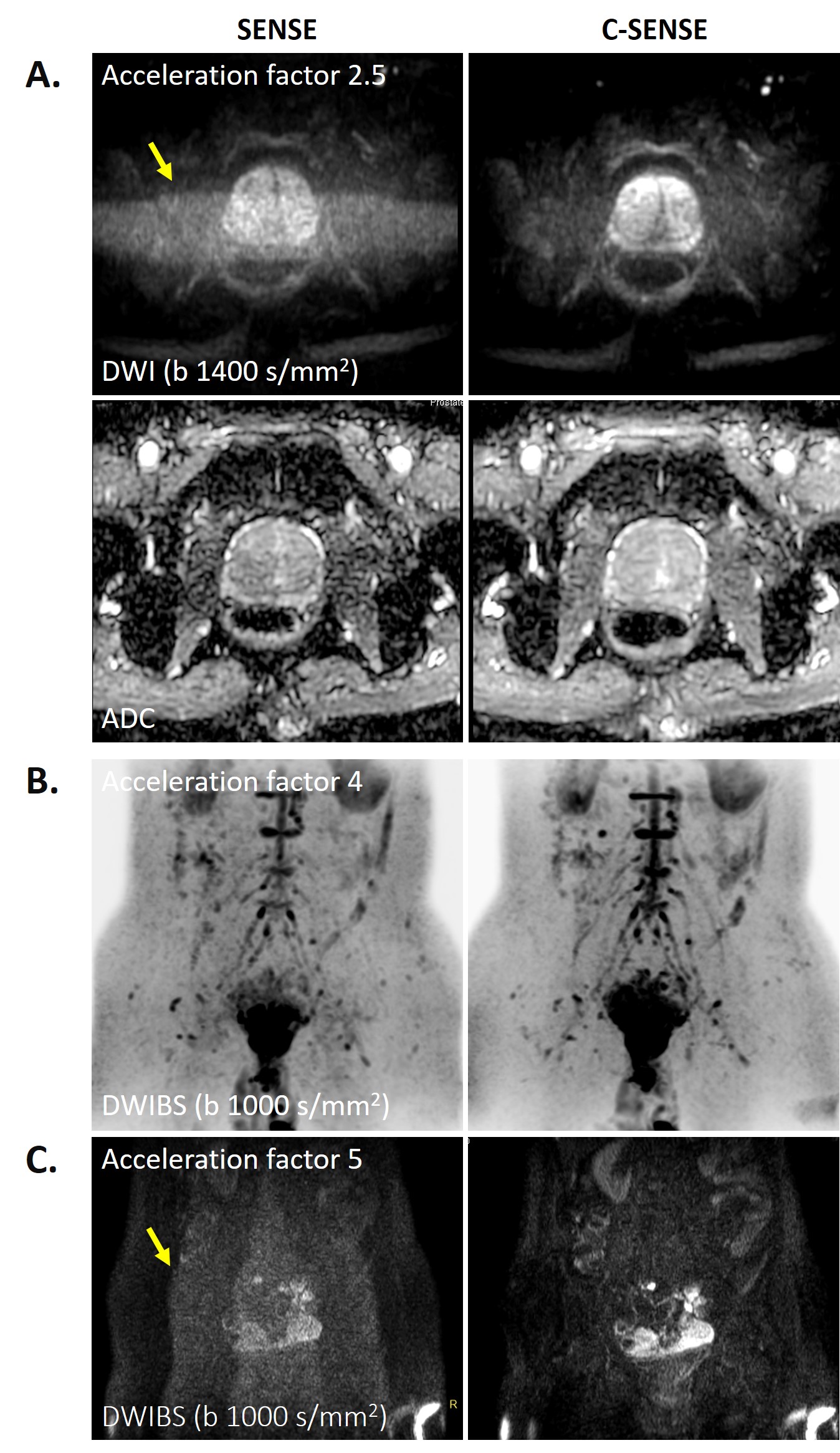
Figure 2. DW-EPI of prostate and pelvis with conventional SENSE (left) vs C-SENSE (right) on 3T. (A) DWI and ADC map in a patient with benign prostatic hyperplasia. Parameters: acquired voxel size 1.5 x 1.5 x 4 mm3, b 1400 s/mm2, SENSE and C-SENSE factor 2.5, scan time 4:50 min. (B) DWIBS in a healthy volunteer with inverted contrast. Parameters: 2 x 2 x 5 mm3, b 1000 s/mm2, SENSE and C-SENSE factor 4, scan time 2 min. (C) DWIBS in a patient with fallopian tube tumor confirmed from findings in DCE-MRI (now shown here). Same parameters as in (B) except for: SENSE and C-SENSE factor 5, scan time 1:05 min.