2610
Integration of novel respiratory navigation techniques into routine abdominal MR examinations1Fairfax Radiological Consultants, Arlington, VA, United States, 2General Electric, Houston, TX, United States
Synopsis
Breath-held acquisitions have long been a staple of body MRI to cope with respiratory motion. While this strategy works for many patients, it is challenging for some. Change in breath-hold capacity from one patient to the next requires frequent parameter tweaking, thus operator skillset becomes a key factor in image quality and consistency. Recent advances in novel motion robust acquisition methods and improved hardware such as Air coils have opened the possibility to perform complete free breathing exams. In this study, we report the feasibility results of free breathing integration into our routine abdominal MRI practice.
INTRODUCTION
Many patients are unable to breath-hold for a multitude of reasons including: imaging under anesthesia/sedation, shortness of breath, illness, claustrophobia, language barriers, or even hearing difficulties. In addition, these issues can also cause significant variability between breath holds that can lead to additional artifact. Traditionally, respiratory navigation has been inefficient, adding significant scan time, limiting usability for the entire exam. Development of faster respiratory navigation techniques, such as DISCO LAVA [1], with more rapid post contrast sequence acquisition, has afforded the ability to perform a free breathing dynamic acquisition. Successful application of radial approaches to free breathing are reported [2]. However, these methods suffer from streak artifacts, inflexible FOV prescription, long reconstruction time and could generate substantially more images putting more pressure on radiologists. Utilizing Cartesian acquisition across the board allowed us to link the coverages and field of FOV across different sequences and make the transition easier as we replaced a breath-hold LAVA with a free breathing DISCO LAVA for about the same duration per phase.
METHODS
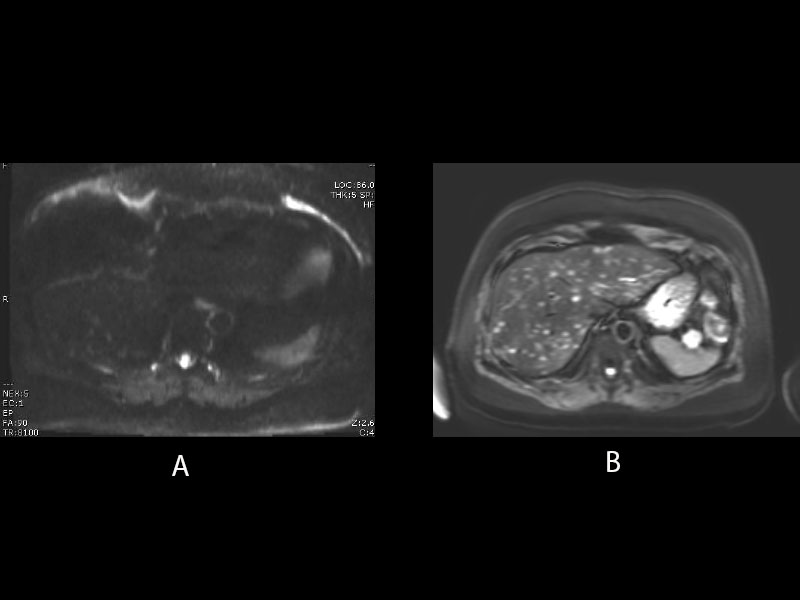
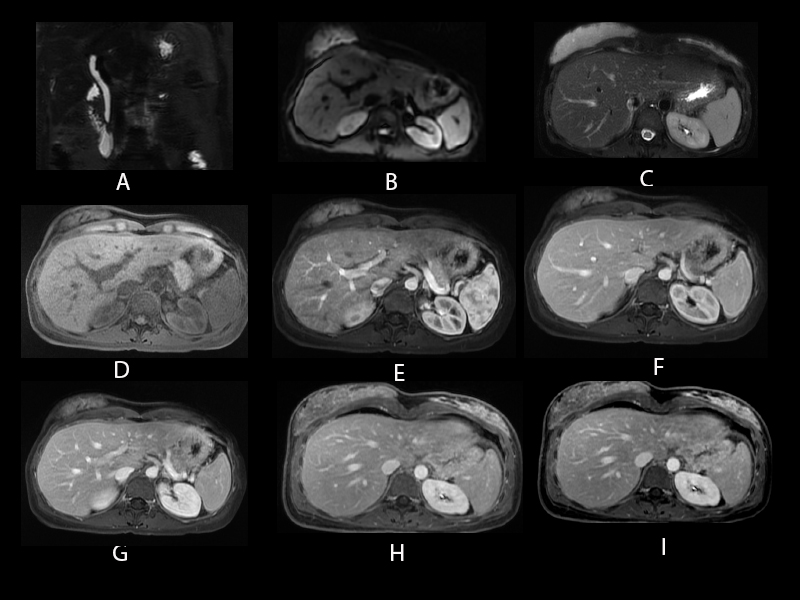
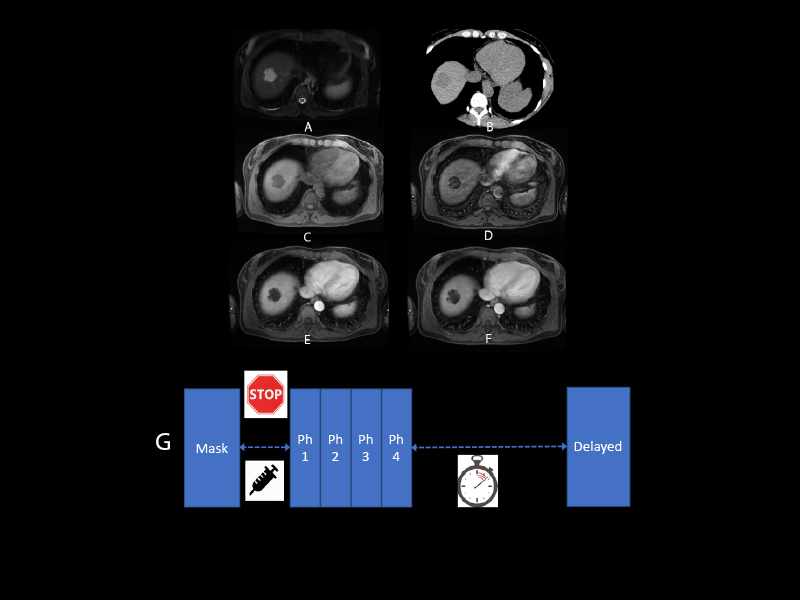
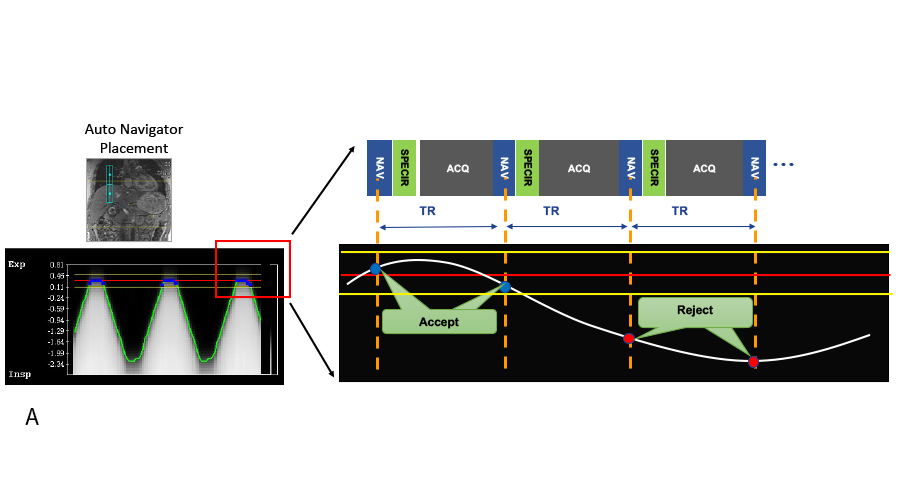
Full free breathing abdominal MR examinations were performed on a GE Signa Premier 3T Magnet utilizing the Air coil taking advantage of the higher acceleration factors to cope with the scan time impact of respiratory motion navigated scans. Integrated auto-navigation was utilized for auto placement of navigator tracker [3]. Liver mass protocol MRI includes the following navigated sequences: Axial fat suppressed Single shot T2, Axial multi-shot DWI, Axial in/out phase, and Axial Dynamic T1. The DISCO LAVA is the critical component in our free breathing exam strategy as it allows us to acquire dynamic T1 with excellent temporal resolution. With this sequence, we moved to a fixed delay (10s) without bolus tracking, thus further simplifying the complexity of the dynamic acquisition. Abdominal MRI/MRCP examination includes the same sequences as the Liver mass protocol with additional 3D MRCP acquired in a coronal plane and an axial 2D MRCP sequence.RESULTS
We were able to integrate a complete free breathing examination into our routine abdominal MR protocols. A total of 17 patients underwent this new free breathing exam. Total scan time for this free breathing protocol has ranged from 17 to 28 minutes, which is well within our standard 45 minute time slot. One patient was sent to our facility for a repeat free breathing examination due to a non-diagnostic prior exam. This exam was completed in 22 minutes with excellent image quality. An MRI/MRCP examination in another patient was performed in 26 minutes fully navigated.DISCUSSION
Development of novel respiratory navigation techniques with integration of newer hardware capabilities has allowed us to transition to full free breathing abdominal MRI protocol. Initial feasibility results on 17 patients demonstrated good image quality with improved patient comfort. In addition, the need for repeat sequences has decreased due to improvements in respiratory motion. Residual motion artifacts were seen in some of the images, but these did not hinder the diagnostic performance. We will continue to monitor the performance especially in more challenging cases such as ascites, irregular breathers, and sleep apnea patients.CONCLUSION
Free breathing abdominal MR examination is an unmet clinical need both in the inpatient and outpatient setting. Our initial feasibility results show that there is potential for a complete free breathing exam. Future developments in respiratory navigation and available sequences are needed to improve options for free breathing abdominal MR examinations. Although auto-navigation techniques have improved, it will likely fail in some patients. Therefore, additional research is necessary to refine motion robust acquisition schemes for these instances.Acknowledgements
No acknowledgement found.References
1. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med. 2016;75(2):775-88.
2. Saranathan M, Rettmann DW, Hargreaves BA, Clarke SE, Vasanawala SS. Differential subsampling with cartesian ordering (DISCO): a high spatio-temporal resolution dixon imaging sequence for multiphasic contrast enhanced abdominal imaging. J Magn Reson Imaging 2012;35:1484–1492
3. Goto, Takao, & Kabasawa, Hiroyuki (2010). Automated positioning of scan plane and navigator tracker in MRI liver scan. Medical Imaging Technology, (suppl), 8.
Figures