2607
Effect of Continuous table movement (CTM) on fat saturation quality in T2 weighted imaging1Medical Imaging, University of Arizona, Tucson, AZ, United States, 2University of Arizona, Tucson, AZ, United States, 3University of Arziona, TUCSON, AZ, United States
Synopsis
Uniform fat suppression is critical for optimal MR assessment of lesions in the abdomen and pelvis. Recent advances using SPAIR sequencing have improved fat suppression and increased the signal-to-noise ratio versus older techniques. However, fat suppression still remains challenging in anatomical regions away from the magnetic isocenter due to field inhomogeneity. Here we demonstrate that continuous table movement (CTM) is superior to fixed table (FT) technology for SPAIR-mediated fat suppression across the entire image stack. As field inhomogeneity away from isocenter is a common challenge, CTM may provide a solution to many frequently encountered problems.
Abstract
Introduction: Effective and uniform fat suppression on axial T2-weighted single-shot imaging is critical for optimal assessment of lesions in the abdomen and pelvis. Advances in single shot fast spin echo (SSFSE) imaging, specifically the use of spectral adiabatic inversion recovery (SPAIR), have shown superior fat suppression and increased signal-to-noise ratio of liver lesions compared to older techniques such as inversion-recovery (IR) SSFSE. However, in slice locations far from the table isocenter, effective fat suppression remains challenging for all types of sequences including SPAIR. Recently, continuous table movement (CTM) technology has been introduced on the Siemens platform that enables every slice to be acquired at or near the isocenter. We investigated the effect of CTM on the quality of fat suppression compared to fixed table (FT) multi-station acquisitions .Methods: All patients were scanned on a Siemens 1.5T MRI scanner. A total of 92 patients were retrospectively analyzed : 43 female, age 16 – 87, average 62.5 and 49 male, age 35 – 87, average 62.2. Each patient was imaged with a SPAIR fat-saturated T2-weighted SSFSE sequence using both a CTM and a FT multi-slice acquisition mode. Acquisition scan parameters were kept identical between both techniques. For each abdominal exam, slices at three different locations (top, center, and bottom slices in the imaging slab) were selected, with the center location representing the slice closest to magnetic isocenter. Four ROIs (anterior, posterior, left, right) were then outlined within each slice. The mean signal intensity was recorded, and the ratio of mean intensity of FT to CTM was calculated for each of the ROIs for each slice. A t-test was used to evaluate statistical significance.
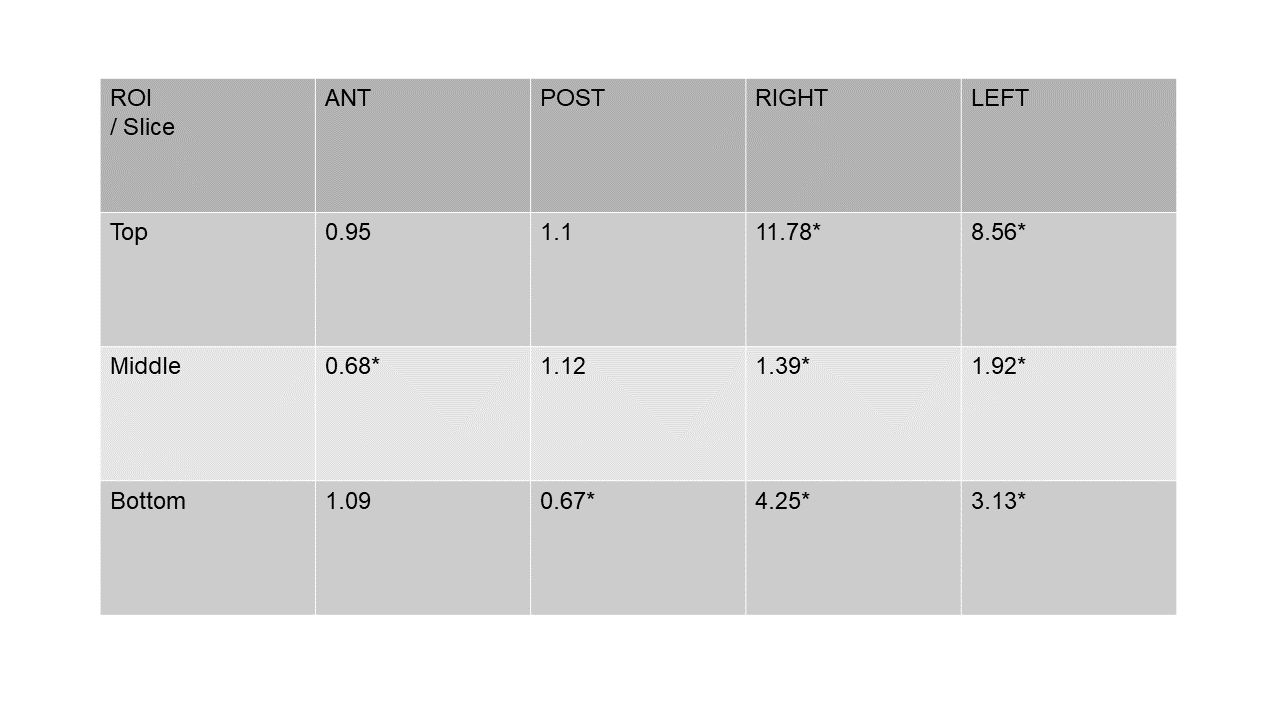
Results: Figure 1 shows representative images from FT (top) and CTM (bottom) SSFSE for top, center, and bottom slice locations in the slab. Note the significantly better fat suppression in CTM SSFSE especially for the outer slices (bottom left, bottom right). Figure 2 tabulates FT to CTM signal intensity ratios for the three slice locations for all 4 ROIs. The edge slices have significantly higher ratios (p<0.006) indicating significantly worse fat sat for FT in the left and right ROIs. The central location has comparable fat sat for both methods due to proximity to isocenter.
Discussion: Over the last decade, continuous table movement (CTM) technology has been developed and refined to allow acquisition of images while the patient is continuously moving through the magnet. In contrast to the conventional multi-station fixed table (FT) approach, CTM allows for every image to be acquired at or near the magnetic isocenter over large z-fields- of- view (FOV) with a consequent reduction in image artifact from field inhomogeneity and improved scan times. Sequential 2D and volumetric 3D techniques have been explored but not quantitatively in a clinical setting. MR angiography with peripheral run-off and whole-body cancer staging comprise the two major categories of clinical studies in which the potential benefits of CTM have been investigated. Fewer studies have been performed to demonstrate the utility of CTM technology in decreasing effects of field inhomogeneity on image quality in anatomic regions which are conventionally positioned distant from magnetic isocenter. CTM technology provides improved quality of fat suppression compared to fixed table (FT) multi-station acquisitions by allowing optimal slice homogeneity for spectral fat selection radiofrequency pulses. The results from our quantitative analysis show the greatest CTM gains in subcutaneous fat suppression and signal uniformity occur in the superior and inferior beginning and end slices, locations furthest from magnetic isocenter when acquiring conventional fixed-table multi-slice sequences. There were no significant gains in fat suppression or uniformity in the mid slices.
Conclusion: CTM technology affords consistent imaging at or near the magnetic isocenter while also reducing the time required for image acquisition. Our data reflects this by the improved fat suppression (recorded as reduced mean signal intensity) compared to conventional FT methodology, particularity at outer slice positions where field inhomogeneity interrupts fat-water frequency shift.
Legends
Figure 1. Representative images from FT SSFSE (top) and CTM SSFSE (bottom) shown for top, center, and bottom slice locations in the slab. Note the significantly uniform and efficient fat suppression in CTM SSFSE esp. for the edge slices (bottom left, bottom right) and comparable fat suppression for the near isocenter center slice (middle column).Figure 2. Table showing FT to CTM signal intensity ratio. The edge slices have higher ratios indicating significantly poor fat sat for FT in the left and right ROIs as also visualized in Figure 1. * indicates statistical significance of p<0.006.
Acknowledgements
No acknowledgement found.References
Lauenstein et al., Evaluation of optimized inversion-recovery fat-suppression techniques for T2-weighted abdominal MR imaging. J Magn Reson Imaging. 2008 Jun;27(6):1448-54.
Sengupta S, Smith DS, Welch EB. Continuously moving table MRI with golden angle radial sampling. Magn Reson Med. 2014 Dec 02; [doi: 10.1002/mrm.25531]
Figures
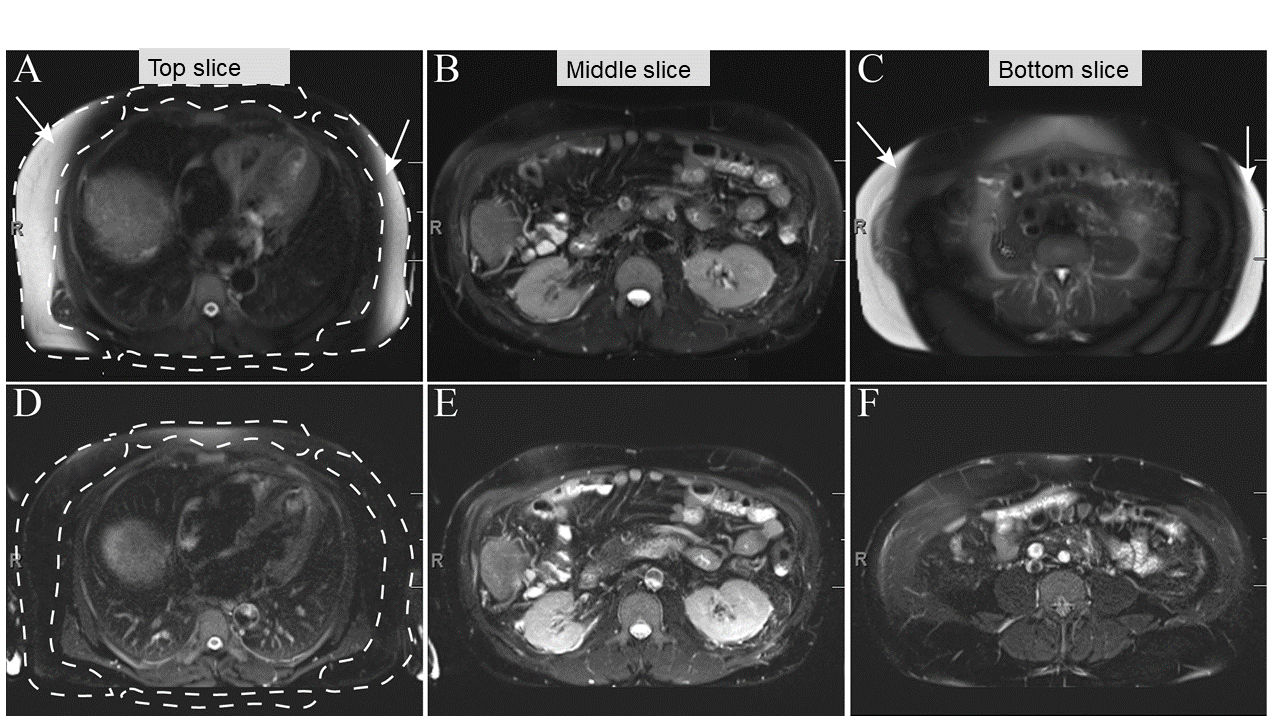
Figure 1. Representative images from FT SSFSE (top) and CTM SSFSE (bottom) shown for top, center, and bottom slice locations in the slab. Note the significantly uniform and efficient fat suppression in CTM SSFSE esp. for the edge slices (bottom left, bottom right) and comparable fat suppression for the near isocenter center slice (middle column).