2606
Compressed Sensing and Parallel Imaging on 3D Uterus Imaging1The First Affiliated Hospital of Dalian Medical University, Dalian Medical University, Da Lian, China, 2Philips Healthcare, Beijing, China, Beijing, China
Synopsis
Acquisition time is one of the main limiting factors in MRI. Compressed sensing is an emerging technology proven to effectively shorten scan time in several clinical scenarios. Here we propose to apply a combination of compressed sensing and sensitivity encoding in 3D uterus imaging that yields 1x1x2 mm3 resolution and uncompromised image quality with 5-fold acquisition acceleration.
Introduction
Compared to the statistics in developed countries, prevalence of uterine cancer in China tend to increase especially in the younger population [1]. 3D pelvic imaging is expected to capture more image information for uterine cancer diagnosis due to the improved spatial resolution and arbitrary plane reconstruction in contrast to the regular 2D imaging techniques. relatively Traditional 3D MR is sometimes corrupted by motion artifacts due to the relatively scan time, and compressed sensing [2] is proven to help through shortening the imaging time. In this study, the aim was to explore the optimal acceleration factor of the combined use of compressed sensing and sensitivity encoding (CS-SENSE) [3] in T2-weighted 3D uterus imaging.PURPOSE
To explore the effects of different CS-SENSE acceleration factors on the image quality of T2-weighted 3D uterus imaging.METHOD AND MATERIALS
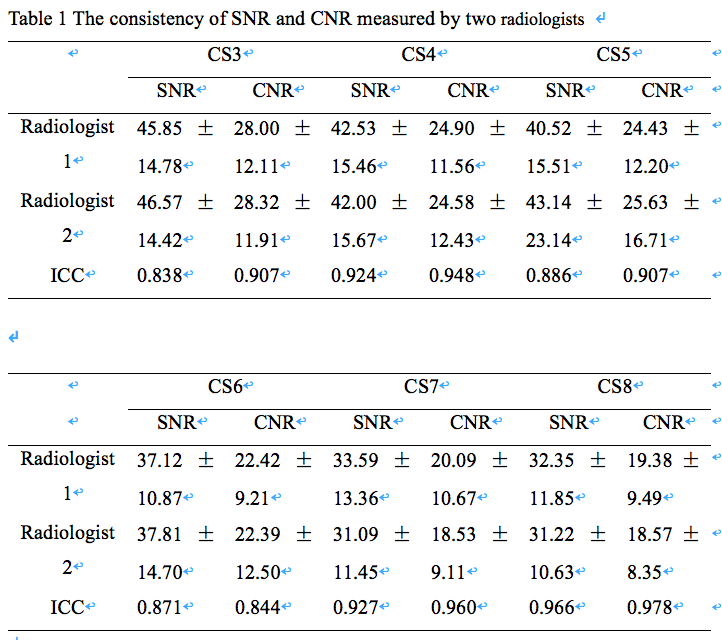
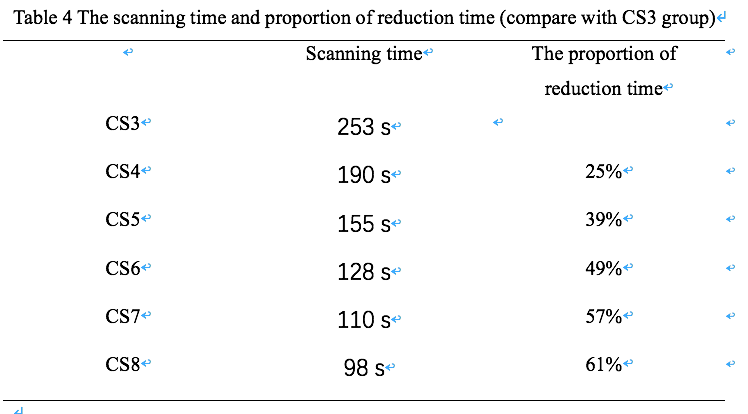
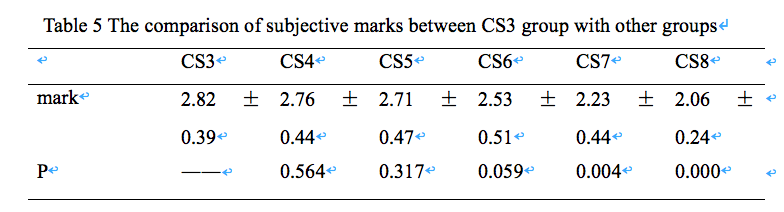
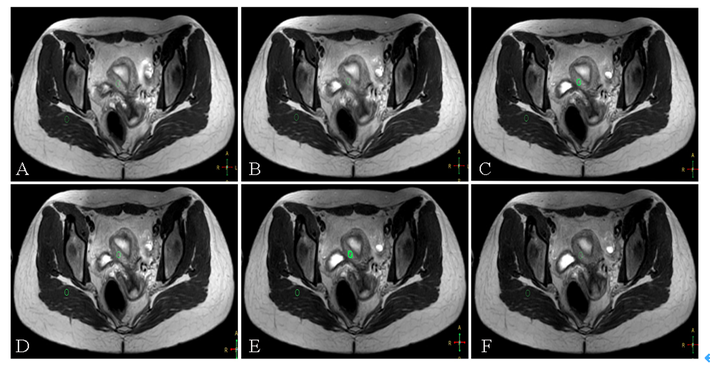
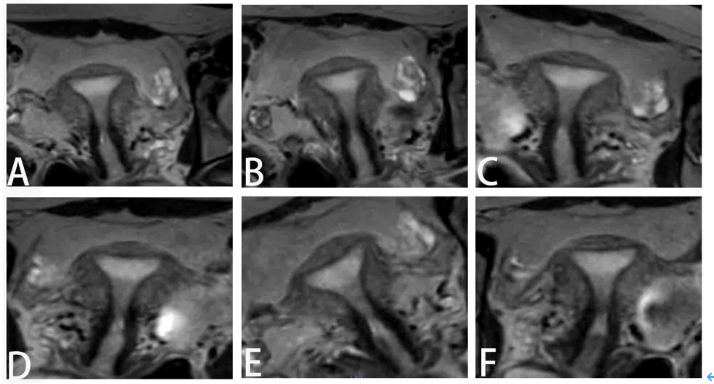
Seventeen healthy young volunteers (mean age 25.24±1.68 years) underwent 3.0T MR scan (Ingenia CX, Philips Healthcare, Best, the Netherlands) including the T2-weighted 3D Turbo-Spin-Echo sequence (3D Pelvic View). The parameters: axial orientation, TR/TE=1300/125 ms, Flip Angle 90°, FOV=350×400×120 mm3, and ACQ Voxel Size 1.1x1.3x2 mm3. The sequence was repeated 6 times for each volunteer with CS-SENSE acceleration factors 3, 4, 5, 6, 7 and 8. The scan time was 253s, 190s, 155s, 128s, 110s, 98s, respectively. Two radiologists (with 5 years and 2 years' work experience respectively) made subjective evaluation on images reconstructed by curved planar reformationusing a 3-point scale. Circular ROIs were manually placed by two radiologists on the outer myometrium and gluteus at the maximum slice. The measurement data included signal intensity (SIm) of the outer myometrium and signal intensity (SIg) and standard deviation (SDg) of the gluteus maximus. The signal-to-noise ratio (SNR) and contrast-to-noise (CNR) of the images were calculated. The intraclass correlation coefficients (ICC) for each measurement between the two radiologists was tested. Paired sample t test was used to compare the differences of SNR and CNR between CS3 group and other groups. Wilcoxon test was used to compare subjective scores between groups.RESULTS
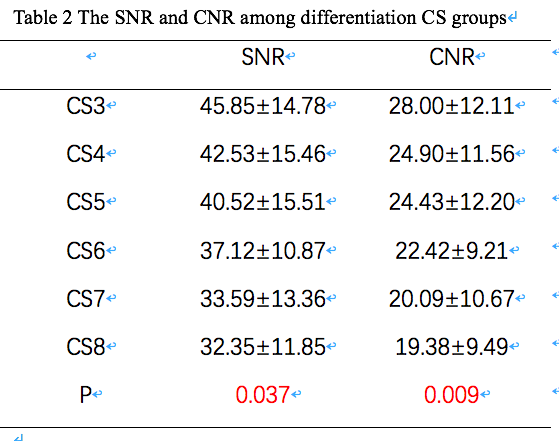
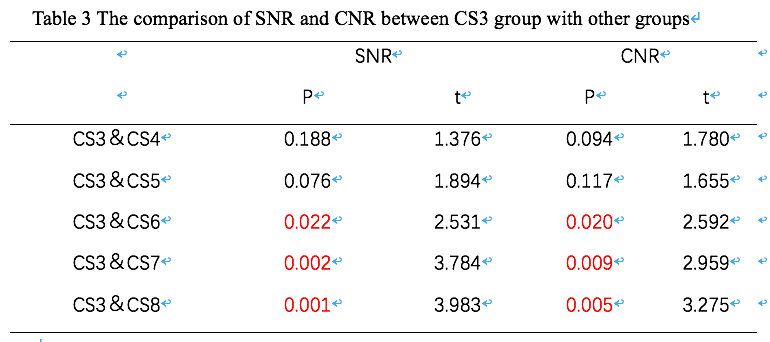
The consistency of the measurements obtained by the two observers were good (ICC value > 0.8, Table 1). Compared with CS-SENSE3 group, the imaging time was reduced by 25%, 39%, 49%, 57% and 61% for CS-SENSE4, 5, 6, 7, and 8 groups, respectively. SNR and CNR of the 6 groups decreased gradually with the increase of acceleration factor, and SNR and CNR of CS3 group were the highest in 6 groups (Table 2). There was statistically significant difference of SNR and CNR of myometrium among all groups (P<0.05). However, there was no significant difference of SNR and CNR between group CS3 and CS4 (P=0.188, 0.094), which was also observed between group CS3 and CS5 (P=0.076, 0.177). While, there was statistically significant difference of SNR and CNR between group CS3 and CS6 (P<0.05), which was also observed between group CS3 and CS7, group CS3 and CS8(Table 3). With the increase of acceleration factor, the image quality scores of each group decreased. There was no significant difference of subjective scores between group CS3 and CS4, which was also observed between group CS3 and CS5, group CS3 and CS6 (Table 5). However, there was significant difference of subjective scores between group CS3 and CS7, which was also observed between group CS3 and CS8.Discussion and conclusion
CS-SENSE acceleration factor of 6 resulted in images with similar SNR, CNR, and subjective score as measured for CS-SENSE3 images, while the scan time was halved. When compared to the CS-SENSE6, higher acceleration factors (7 and 8) cut the scan time by only 14% and 23% at the cost of compromised image quality. These observations were consistent in both regular imaging results and the curve planar reformatted images. In practice, the reduced scan time will help to avoid motion artifacts that would otherwise disturb the presentation of fine structures that are important for the high-resolution 3D images, and this would be particularly valuable for uterine cancer patients with poor coordination. CS-SENSE acceleration factor 6 is hence recommended for clinical routine T2w 3D pelvic imaging, and a study with more participants suspected with uterine diseases is under planning to verify this point.Acknowledgements
No acknowledgement.References
[1] Feng RM, Zong YN, Cao SM, et al. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics? [J]. Cancer Commun (Lond). 2019 Apr 29; 39(1): 22.doi: 10.1186/s40880-019-0368-6.
[2] Lustig M, Donoho D Pauly J M. Sparse MRI: The application of compressed sensing for rapid MR imaging[J]. Magnetic Resonance in Medicine, 2007, 58(6):1182-1195.
[3] Bratke G, et al. Accelerated MRI of the Lumbar Spine Using Compressed Sensing: Quality and Efficiency. J Magn Reson Imaging 2018; 49: e164-e175.
Figures