2577
MRE for the detection of inflammatory diseases of the juvenile Crohn’s disease: quantifying the inflammatory activity.
zheng xian ying1 and Zhang Zhong shuai2
1First affiliated Hospital of Fujian Medical University, fuzhou, China, 2MR , Siemens Healthcare, Shanghai, China
1First affiliated Hospital of Fujian Medical University, fuzhou, China, 2MR , Siemens Healthcare, Shanghai, China
Synopsis
This study aimed to demonstrate that Magnetic resonance enterography global score (MEGS) shows equally values in pediatric crohn's patients and had comparable diagnostic efficacy comparing with other MRE scores. 52 juvenile Crohn patients were included, and MEGS, SES-CD and eAIS of the terminal ileum were calculated. The results show that for both endoscopically defined and histologically defined active inflammation and ulcerative lesions MEGS have high diagnostic accuracy, are consisting with other studies. The results provided in the current study suggest that MR may be considered as an alternative to endoscopy.
Introduction
Crohn’s disease (CD) is a chronic inflammatory bowel disease (IBD) characterized by transmural bowel wall inflammation which lasts throughout the patient’s life with childhood onset in 10% to 25% among all the CD patients[1]. The assessment of disease extension and activity is crucial in juvenile with CD to determine optimal treatment strategies and thereafter monitor response to treatment. This assessment usually relies on endoscopy. However, endoscopy cannot always be performed completely, and there are several drawbacks related to the invasiveness, procedure related discomfort, risk of bowel perforation and relatively poor patient acceptance. Especially for children, enteroscopy is a more painful and terrible experience. Magnetic resonance imaging (MRI) is characterized by a very high soft tissue contrast, lack of ionizing radiation and lower incidence of adverse events related to the intravenous contrast employed compared with CT. Recently, some study compared between MRE and colonoscopy in assessing CD inflammatory lesions and related complications for adult patients . Only a few studieshave tested the accuracy of MR enterography in localizing and evaluating CD intestinal lesions in children, with preliminary satisfactory results. However, there are no reports of its use in adolescents. The aim of this study is to evaluate the accuracy of MRE in the diagnosis of active lesions and ulcers in juvenile CD against endoscopic and histopathology reference standard.Method
Data were collected on two different 3T MRI scanners (MAGNETOM Skyra /Verio, Siemens Healthcare, Erlangen ,Germany) with a 16-channel body coil. For this retrospective study, fifty-two adolescent CD patients (28 women, 24 men; mean age, 12 years old; range, 6-17 years) were included, who underwent ileocolonoscopy and MR enterography within 7days and the terminal ileum biopsy was available. T2-weighted and pre- and postcontrast enhanced T1-weighted and DWI sequence were acquired. The Simplified Endoscopic Activity Score for Crohn’s Disease ( SES-CD) , histopathologic endoscopic acute inflammation score[eAIS]) and Magnetic resonance enterography global score (MEGS) [2] were scored in the terminal ileum; sensitivity and specificity of MEGS for disease activity and ulceration against SES-CD and eAIS were compared by using the McNemar test. The correlation between MEGS and the reference standard (SES-CD and eAIS) was assessed by Spearman rank estimation. The diagnostic accuracy of MER for active disease and ulceration defined by endoscopic or histopathologic were calculated. Receiver operating characteristic curves (ROC) were constructed.Results
An example of MR alterations associated with the presence of active inflammation is shown in Fig 1. There was no significant difference in the detection of terminal ileum active lesions and ulcerative lesions among MRE and colonoscopy and histopathology. MEGS showed strong correlation to SES-CD (r =0.698) and weak correlation to eAIS(r= 0.21) (Fig 2). With endoscopy as the reference standard, receiver operating characteristic curves of detected lesions, active lesions (SES-CD ≥2) and ulcer lesions are shown in figure 3A. With histopathologic as the reference standard, receiver operating characteristic curves of detected active lesions (eAIS ≥2) and ulcer lesions are shown in figure 3B. Against SES-CD, the AUC obtained by magnetic resonance score of inflammatory and active diseases and ulcer lesions were 0.87, 0.87 and 0.85, respectively. Against eAIS, for evaluation of active disease and ulcer lesions MEGS score generated AUC are 0.60 and 0.60, respectively. The corresponding receiver operating characteristic curves were not significantly different.Discussion and Conclusion
In this study, we retrospectively examined the accuracy of MEGS in diagnosing terminal ileum inflammation in juvenile crohn's disease with both SES-CD and eAIS as the reference standard. We found that for both endoscopically defined and histologically defined active inflammation and ulcerative lesions MEGS have high diagnostic accuracy (85–87% and 60%, respectively), these results are consistent with other studies of MRE versus colonoscopy and histopathology in adult crohn patients.[3,4,5]. Results of this study suggest that MEGS score is also suitable for Crohn patients in children, and has considerable diagnostic accuracy compared with other MRI scores in judging the activity of lesions and the presence or absence of ulcers. Overall, the results of this study suggest that MR may be considered as an alternative to endoscopy in cases with an established diagnosis of juvenile CD in which biopsy samples are not necessary.Acknowledgements
No acknowledgement found.References
1. Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, VanLimbergen J, Griffiths AM (2011) Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis 17:423–439.2. Maccioni F, Bencardino D, Buonocore V et al (2019) MRI reveals different Crohn’s disease phenotypes in children and adults. Eur Radiol 29(9):5082-5092 .3. Rimola J , Alvarez-Cofiño A, Pérez-Jeldres T , et al.Comparison of three magnetic resonance enterography indices for grading activity in Crohn’s disease. J Gastroenterol. 2017 ;52:585-593.4. Hordonneau C, Buisson A, Scanzi J, et al. Diffusion-weighted magnetic resonance imaging in ileocolonic Crohn’s disease: validation of quantitative index of activity. Am J Gastroenterol 2014; 109:89–98.5. Garcı´a-Bosch O, Orda´s I, Aceituno M, et al. Comparison of diagnostic accuracy and impact of MRI and colonoscopy for the management of Crohn’s disease. J Crohns Colitis. 2016;. doi:10. 1093/ecco-jcc/jjw015.Figures
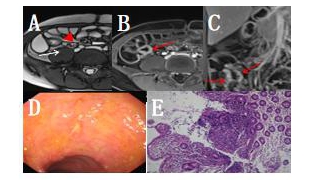
Magnetic resonance axial T2WI depicts mild wall thickening of the terminal ileum (arrowheads) that also has a hypersignal relative to the psoas muscle (arrow) indicating the presence of oedema. (B) Axial and Coronal (C)T1-VIBE after intravenous contrast administration. Marked enhancement of the terminal ileum (arrows) relative to the remaining ascend colon can be seen. Also note the presence of the irregularity of the mucosal surface showing ulcers and inflammatory pseudopolyps. colonoscopy of the same segment shows the presence of superficial ulcers in the mucosa (D).
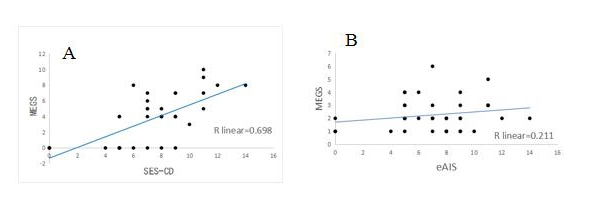
Fig2.Correlation among the Crohn’s Disease Magnetic resonance enterography global score(MEGS) and Simplified Endoscopic Activity Score for Crohn’s Disease (SES-CD) (A) and endoscopic biopsy acute histologic inflammatory score(eAIS) (B).
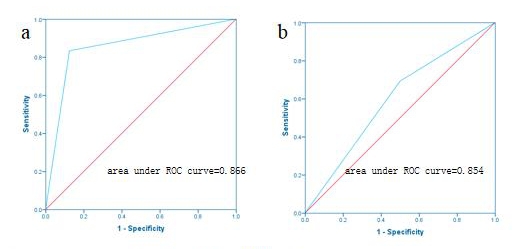
Fig 3A. Receiver operating characteristic (ROC) curves, of amagnetic resonance-based index to predict presence of active disease (a) and presence of ulcerative lesions (b) in Crohn’s disease using endoscopy as a reference.
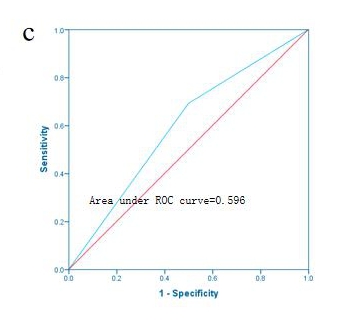
Fig 3B. Receiver operating characteristic (ROC) curves, of a magnetic resonance-based index to predict presence of active disease (c) and presence of ulcerative lesions (c) in Crohn’s disease using histopathology as a reference.