2576
Quantitative evaluation of ileal crohn’s disease with intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI)1Department of Radiology, Shanghai Tenth People’s Hospital of Tongji University, School of Medicine, Shanghai, China, 2Clinical Science, Philips Healthcare, Shanghai, China
Synopsis
Crohn’s disease (CD) is a chronic inflammatory bowel disorder that can occur in any section of the gastrointestinal tract, commonly affecting the small intestine, especially the ileum. Colonoscopy used as the gold standard for assessing disease activity, but its invasiveness limits the use. We aimed to assess inflammatory activity of CD patients by using Intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI), and found IVIM-DWI may serve as a promising method for noninvasive detecting and monitoring the activity of CD.
Introduction
Intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI) acquires both perfusion and diffusion information without injection of contrast medium, which is promising in Crohn’s disease (CD) activity assessment[1,2]. This study aimed to assess the accuracy of IVIM-DWI for detecting the inflammatory activity in normal and abnormal ileal segments, to investigate the reproducibility of IVIM-MRI parameters, and also to analyze the correlation between IVIM-DWI parameters with clinical and MRI-based data.Methods
44 CD patients who underwent Magnetic resonance enterography (MRE) with IVIM-DWI from October 2018 through May 2019 were included (31 male, 13 female; mean age: 33.66 ± 13.87 years; age range: 13-62 years). IVIM-DWI parameters: diffusion coefficient (D), pseudo-diffusion coefficient (D*), perfusion fraction (f), the multiplication of the two parameters (f·D*), apparent diffusion coefficient (ADC), exponential ADC (eADC) and computed diffusion-weighted imaging (cDWI) were evaluated in abnormal ileal segment and the adjacent normal segment, so were the conventional MRI parameters. Comparison of IVIM-DWI parameters between normal and abnormal bowel segments were performed using Wilcoxon signed-rank tests. The receiver operating characteristics (ROC) analysis was performed to determine the sensitivity, specificity, and diagnostic accuracy for the detection of the abnormal bowel segments. Correlation among IVIM-DWI parameters in inflamed bowel segments, clinical parameters (CRP, ESR, CDAI), conventional MRI measurement (wall thickness), and MRE score (Clermont score) were assessed using Spearman’s rank correlation analysis.Results
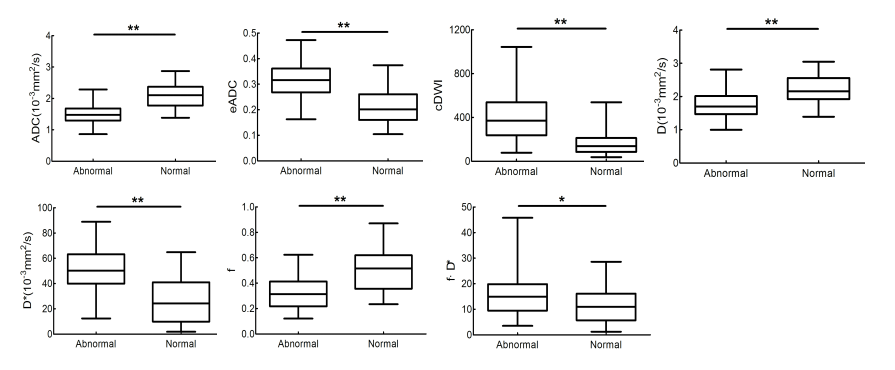
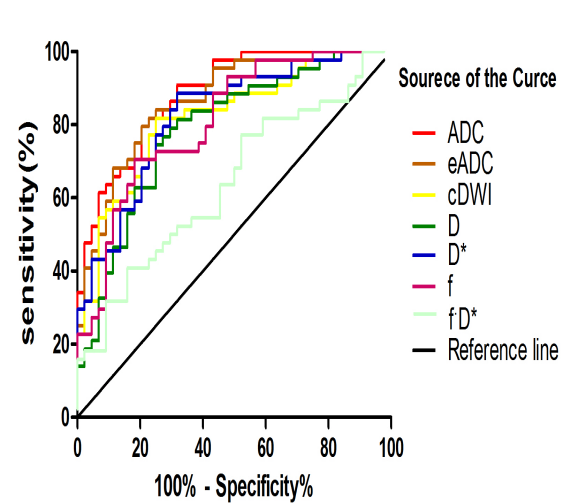
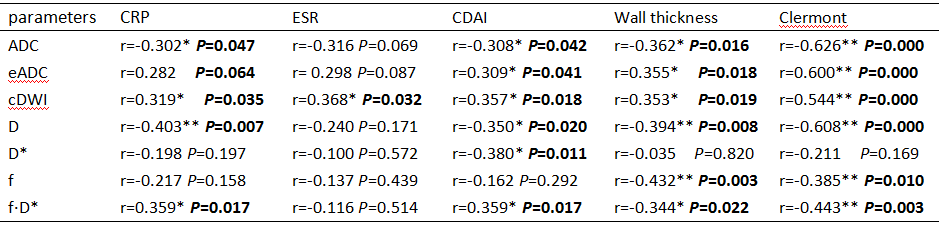
The mean values of eADC, cDWI, D*and f·D* were significantly higher in abnormal segments (p˂0.001, p˂0.001, p˂0.001 and p=0.011, respectively), and the mean values of ADC, D and f were significantly lower in abnormal segments(p˂0.001, p˂0.001, and p˂0.001, respectively)(Fig. 2). Except f·D*, the AUCs of IVIM-DWI parameters ranged from 0.774 to 0.882, and the sensitivity and specificity of IVIM-DWI parameters were in the range of 68.2% - 81.8% and 70.5% - 88.6%, respectively(Fig. 3). ADC values showed the highest diagnostic accuracy for prediction of inflamed bowel, using cutoff value of 1.69 ×10-3 mm2/s, the sensitivity and specificity of ADC were 81.8% and 77.3%, respectively. An indicator combining ADC and D* had a higher diagnostic efficiency, with AUC of 0.923, 84.1% sensitivity, and 84.1% specificity. All IVIM-DWI parameters had good to excellent interobserver repeatability in inflamed bowel, 0.891 (95% CI, 0.801–0.941) for ADC, 0.883 (95% CI, 0.785–0.936) for eADC, 0.913 (95% CI, 0.841-0.953) for cDWI, 0.840 (95% CI, 0.707-0.913) for D, 0.784 (95% CI, 0.604-0.882) for D*, 0.934 (95% CI, 0.878-0.964) for f, 0.788 (95% CI, 0.612-0.885) for f·D*. The correlation between IVIM-DWI parameters and clinical data (CRP, ESR, CDAI) was none or fair. ADC, eADC, cDWI, D, f and f·D* showed significant fair-to-moderate correlations with clermont score, but fair correlations with wall thickness(Table 1).Conclusions
In conclusion, for MRE, ADC, eADC, cDWI, D, D*, f and f·D* of IVIM-DWI showed significantly accuracy to reflect the activity of ileum inflammation for CD as quantitative parameters, especially the indicator combining ADC and D* indicated the best potential for assessment of CD inflammation. Thus, IVIM-DWI may serve as a promising noninvasive imaging method for detecting and monitoring CD.Acknowledgements
No acknowledgement found.References
[1] Freiman M, Perez-Rossello JM, Callahan MJ, el al. Characterization of Fast and Slow Diffusion From Diffusion-Weighted MRI of Pediatric Crohn’s Disease[J]. J Magn Reson Imaging. 2013 Jan;37(1):156-163.
[2] Hectors SJ, Gordic S, Semaan S, el al. Diffusion and perfusion MRI quantification in ileal Crohn’s disease[J]. Eur Radiol. 2019 Feb;29(2):993-1002.
Figures