Renwang Pu1, Jiazheng Wang2, Liangjie Lin2, Jingjun Wu1, Qingwei Song1, Nan Zhang1, and Ailian Liu1
1Department of Radiology, the First Affiliated Hospital of Dalian Medical University, Dalian, dalian, China, 2Philips Healthcare, Beijing, China, beijing, China
Synopsis
The present
study aims to explore feasibility of three-dimensional(3D)breath-hold(BH)magnetic
resonance cholangiopancreatography (MRCP) through acceleration of the
combination of compressed sensing and sensitivity encoding(CS-SENSE),and choose
an optimal acceleration factor. 3D-MRCP scans on healthy volunteers were carried
out with different acceleration factors (conventional SENSE factor of 4, and CS-SENSE
factors of18, 24, and 32).The CS-SENSE acceleration factor of 24 was recommended
because of the favorable image quality and reasonable scan duration (15s).
Introduction
3Dmagnetic resonance cholangiopancreatography (MRCP)is a well-established tool for noninvasively anatomical evaluation of bile duct and pancreatic duct1.A major limitation of 3D MRCP lie in that it is usually implemented along with respiratory/navigator triggering due to the prolonged scan time2.The compressed sensing (CS) technique has now been widely used for acceleration of MR examinations by exploiting information redundancies in data sampling and image reconstruction3,4,5.The introduction of CS for fast3DMRCP within one breath-hold (3D-BH-MRCP)can be of great values for clinical applications6,7.The present study aims to explore the optimal acceleration factor for3D-BH-MRCP when a combination of compressed sensing and sensitivity encoding (CS-SENSE) is used8.Materials and methods
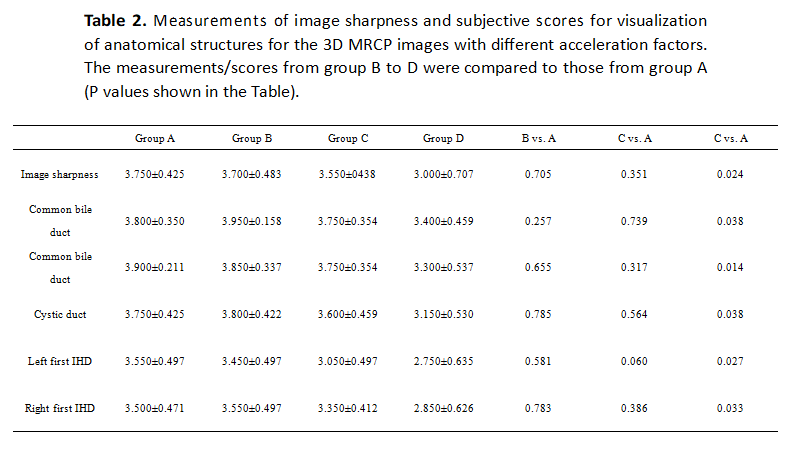
Twenty healthy subjects(mean age; (24.143± 1.98 years);12 women; 8 men) were recruited, and underwent scans on a 3.0T MR scanner(Ingenia CX, Philips Healthcare, Best, the Netherlands). The 3D-MRCP scans were carried out using different acceleration factors including the conventional SENSE factor of 4 in group A (respiratory-gate), and CS factors of 18, 24, and 32in groups B to D, with scan durations of 192, 20, 15, and 12.5s, respectively.The scan parameters are summarized in Table 1.After image reconstruction, two radiologists performed the subjective independent scoring based on considerations of the image clearness, image sharpness,and branch visualization of the common bile, common hepatic, cystic,pancreatic, and left and right hepatic ducts. Four-point scoring criteria of image quality was used, and the score more than 3 or equal to 3 was considered in line with clinical requirements.Inter-observer agreements were evaluated using intraclass correlation coefficients (ICC). The subjective independent scores(mean value of scores by the two observers) for groups B to D were compared with those of group A by the Wilcoxon test.Results
The obtained subjective image-quality scores by two observers show good inter-observer agreements with ICC values of 0.789, 0.912, 0.712, and 0.867, respectively for the 4 groups.For comparisons of the subjective independent scores, there was no significant difference observed for groups B and C in comparison to group A(p>0.05). However, scores for group D (CS factor = 32)was statistically lower than that for group A (p<0.05).The results of image quality analysis are summarized in Table 2, while representative images for different acceleration factors were demonstrated in Figurer1. Besides, the pancreatic duct can be visible in 6 cases in groups A to C, but only in 4 cases in group D.Discussion and Conclusions
Based on results of this study, the CS acceleration factor of 24 is recommended that can provide images with favorable quality within a reasonable scan time (15 s). Higher acceleration factor resulted in limited time benefit (16% time reduction from 24-fold acceleration to 32-fold) but significantly degraded image quality.Acknowledgements
No acknowledgement found.References
1. Katabathina VS,Dasyam AK,Dasyam N, et al.Adult bile duct
strictures role of MR imaging and MR cholangiopancreatography in
characterization.Radiographics.2014;34(4):565-586.
2. Zhu L, Xue H, Sun Z, el al.Modified breath-hold compressed-sensing
3D MR cholangiopancreatography with a small field-of-view and high resolution
acquisition: Clinical feasibility in biliary and pancreatic disorders. Magn
Reson Imaging. 2018;48(5):1389-1399.
3. Candes E, Romberg J,Tao T. Robust uncertainty principles:
Exact signal reconstruction from highly incomplete fourier information. IEEE
Trans Inf Theory. 2006;52(8):489–509.
4. Feng L, Benkert T, Bblock K,et al. Compressed sensing for
body MRI.Magn Reson Imaging. 2017;45(4):966–87.
5. Vranic J, Cross N, Wang Y, et
al.Compressed sensing–sensitivity encoding (CSSENSE) accelerated brain imaging:
reduced scan time without reduced image quality.
AJNR Am J Neuroradiol. 2019;40(1):92–98.
6. Suh C,Jung S,Lee H, et al.High-resolution magnetic
imagine using compressed sensing.Invest Radiol. 2019;20(1):487-497.
7. Yi J, LeeY,
HahnS,et al. Fast isotropic volumetric magnetic resonance imaging of the ankle:
acceleration of the three-dimensional fast spin echo sequence using compressed
sensing combined with parallel imaging. Eur J Radiol.2019;112(1):52–58.
8. He M, Xu J, Sun
Z, et al. Comparison and evaluation of the efficacy of compressed SENSE (CS)
and gradient- and spin-echo (GRASE) in breath-hold (BH) magnetic resonance
cholangiopancreatography (MRCP). J Magn Reson Imaging 2019; DOI:
10.1002/jmri.26863.