2548
MR cholangiopancreatography in a single breath-hold: comparative effectiveness between 3D GRASE and 2D thick-slab SSFSE1Graduate Institute of Biomedical Electronics and Bioinformatics, National Taiwan University, Taipei, Taiwan, 2Taipei Beitou Health Management Hospital, Taipei, Taiwan, 3Philips Healthcare, Taipei, Taiwan
Synopsis
3D MR cholangiopancreatography (MRCP) based on gradient- and spin-echo (GRASE) and 2D thick-slab MRCP using fast spin-echo (FSE), both acquired within single breath-hold, were compared using a 4-point score at 3T on 95 healthy subjects (age range = 25-75) in eight different segments of hepatic and pancreatic ducts. 3D GRASE outperformed 2D thick-slab FSE in the common bile duct and common hepatic duct, but compared inferiorly in right anterior hepatic duct (p < 0.001), with insignificant difference (p > 0.05) for the other five ducts. It is concluded that 2D thick-slab FSE MRCP complements 3D GRASE MRCP if performed additionally.
Introduction
The gradient- and spin-echo (GRASE) technique 1 has recently been employed for 3D MR cholangiopancreatography (MRCP) at 3T and demonstrated successful breath-hold acquisition in 9-20 seconds with image quality compared favorably to respiratory-triggered 3D FSE MRCP 2,3. However, the requirement of single breath-hold results in limited scan time which may trade off spatial resolution. The purpose of our study is therefore to compare the depiction conspicuity of 3D GRASE MRCP with 2D thick-slab fast spin-echo (FSE) MRCP, another very fast MRCP sequence capable of acquisition within single breath-hold, in eight different segments of hepatic and pancreatic ducts on a large cohort of subjects.Methods
Both coronal 3D GRASE (TR/TE = 262/107, voxel volume 1.51x1.53x1.20 mm3, 13.1 seconds) and 2D thick-slab FSE MRCP (TR/TE = 5759/800, voxel volume of 0.8x1.0x70 mm3, 5.8 seconds), with scanning parameters adjusted under the constraints of specific absorption rate and scan time within single breath-hold, were performed for a total of 95 subjects (M/F = 49:46, age range = 25-75) at 3T (Philips Ingenia, Best, The Netherlands). Spectral adiabatic inversion recovery was used for fat suppression. Fasting for at least four hours was requested for all subjects before the imaging examinations. Conspicuity of the common bile duct (CBD), common hepatic duct (CHD), right hepatic duct (RHD), right anterior hepatic duct (RAD), right posterior hepatic duct (RPD), left hepatic duct (LHD), pancreatic duct proximal (PDP), and pancreatic duct distal (PDD) was graded on freely rotating maximal projection views using a 4-point score (0 for not visible, 1 for visible but not diagnostic, 2 for visible and diagnostic, and 3 for excellent, respectively).Results
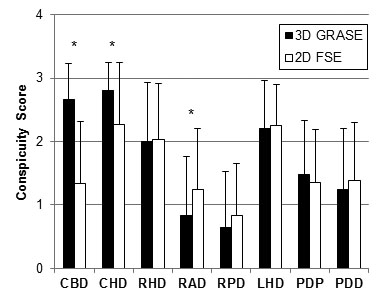
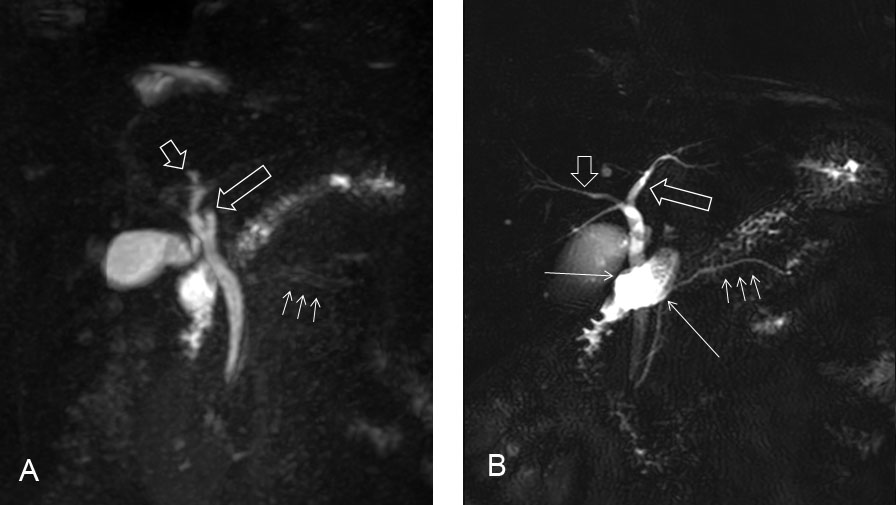
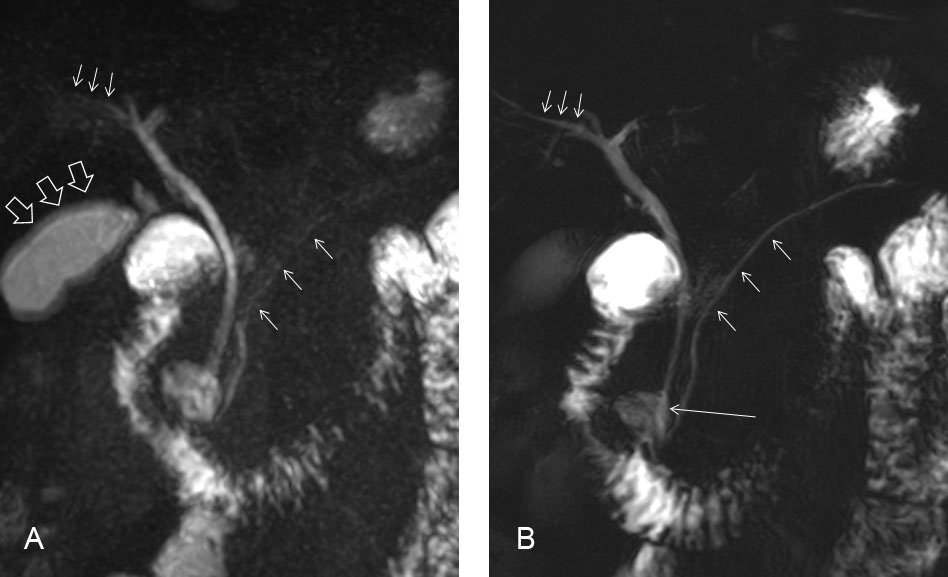
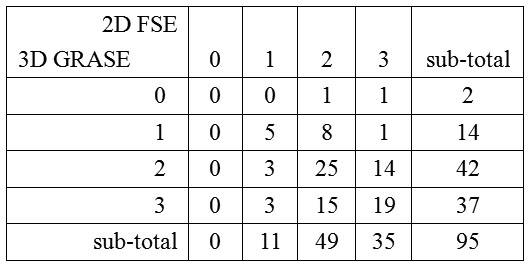
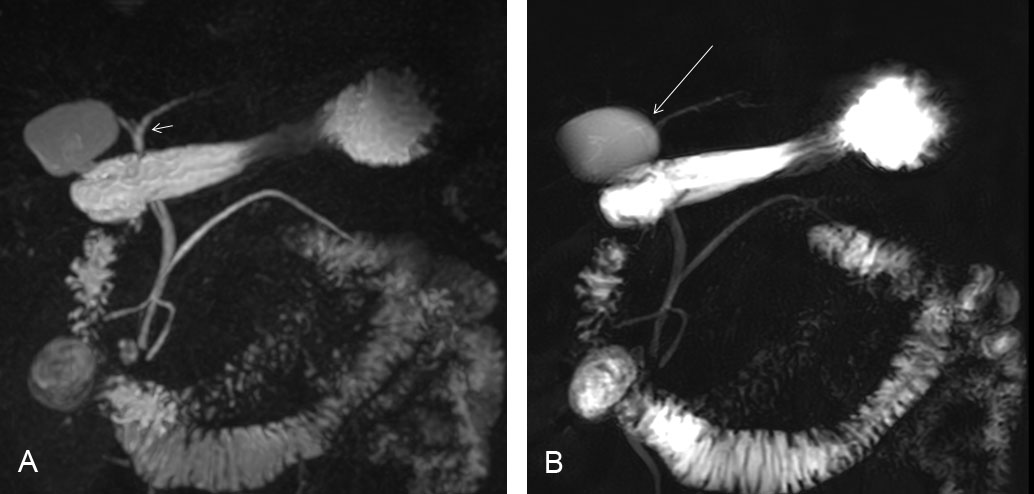
Figure 1 summarizes the conspicuity scores. 3D GRASE MRCP was found to be diagnostically useful for most subjects (mean scores > 2) for CBD (2.67±0.55), CHD (2.80±0.45), RHD (2.00±0.93), and LHD (2.20±0.77), whereas 2D thick-slab FSE MRCP showed similar findings except that it failed to provide diagnostic value for the majority of subjects for CBD (mean scores 1.34±0.97). For RAD, RPD, PDP, and PDD, neither MRCP methods investigated in this study were diagnostically helpful in most of the recruited subjects (mean scores < 2). 3D GRASE MRCP outperformed 2D thick-slab FSE MRCP in CBD and CHD (both with p < 0.001; Figs.2 and 3), but compared inferiorly in RAD (p < 0.001; Fig.2). For the other five ducts, differences between the two MRCP techniques were statistically insignificant (p > 0.05).Comparisons of conspicuity on an individual basis are also listed in tabular form in Fig.4 for LHD as an example. Note the presence of nonzero numbers in off-diagonal entries (46 out of 95; 48.4%), suggesting mutually complementary value of 3D GRASE and 2D thick-slab FSE for MRCP. 3D GRASE alone would miss reliable diagnosis (score = 0 or 1) in 16 subjects (16.8%) (Fig.2), whereas 2D thick-slab FSE would miss 11 (11.6%) (Fig.5). Performing both 3D and 2D acquisitions would reduce the non-diagnostic cases to only 5 remaining (5.3%), suggesting that ideally 3D GRASE and 2D thick-slab MRCP should both be used to increase successful depiction, if LHD is of diagnostic concern.
Discussion
Our results suggest that, due likely to overlapping with residual fluid in the duodenum in 2D thick-slab MRCP 4, 3D GRASE is favorable for MRCP in CBD and CHD, the two major biliary ducts where most pathologies such as stone or obstruction are found 5. However, under the constraint of limited scan time for single breath-hold, settings of scanning parameters in 3D GRASE MRCP resulted in trade-off in various aspects 3. Hence, inferiority of 3D GRASE to 2D thick-slab FSE MRCP in RAD is attributed to difference in in-plane spatial resolution because of the small size of RAD 3,4. For LHD, the two MRCP methods investigated in our study provided complementary value and should thus ideally be both performed.Conclusion
We conclude that although 3D GRASE MRCP is the preferential choice to depict CBD and CHD, the complementary role of 2D thick-slab FSE MRCP in other smaller hepatic and pancreatic ducts makes it a useful adjunct if performed additionally during routine examinations. Both methods allow MRCP to be acquired within one single breath-hold to reduce negative impact from subject motions.Acknowledgements
H.W.C. receives support from the Ministry of Science and Technology under grant MOST 105-2221-E-002-142-MY3.
References
1. Oshio K, Feinberg DA. GRASE (Gradient- and spin-echo) imaging: a novel fast MRI technique. Magn Reson Med 191;20:344-349.
2. Yoshida M, Nakaura T, Inoue T, et al. Magnetic resonance cholangiopancreatography with GRASE sequence at 3.0T: does it improve image quality and acquisition time as compared with 3D TSE? Eur Radiol 2018;28:2436-2443.
3. Nam JG, Lee JM, Kang HJ, et al. GRASE Revisited: breath-hold three-dimensional (3D) magnetic resonance cholangiopancreatography using a Gradient and Spin Echo (GRASE) technique at 3T. Eur Radiol 2018;28:3721-3728.
4. Irie H, Honda H, Kuroiwa T, et al. Pitfalls in MR cholangiopancreatographic interpretation. Radiographics 2001;21:23-37.
5. Fulcher AS, Turner MA, Capps GW, et al. Half-Fourier RARE MR cholangiopancreatography: experience in 300 subjects. Radiology 1998;207:21-32.
Figures