2546
Better Background suppression with GRASE-MRCP using MSDE1Radiology, Seirei Mikatahara General Hospital, Hamamatsu, Japan, 2Nagoya University, Graduate School of Medicine, Nagoya, Japan, 3Seirei Mikatahara General Hospital, Hamamatsu, Japan, 4Philips Electronics Japan, Ltd., Tokyo, Japan, 5Hamamatsu University School of Medicine, Hamamatsu, Japan
Synopsis
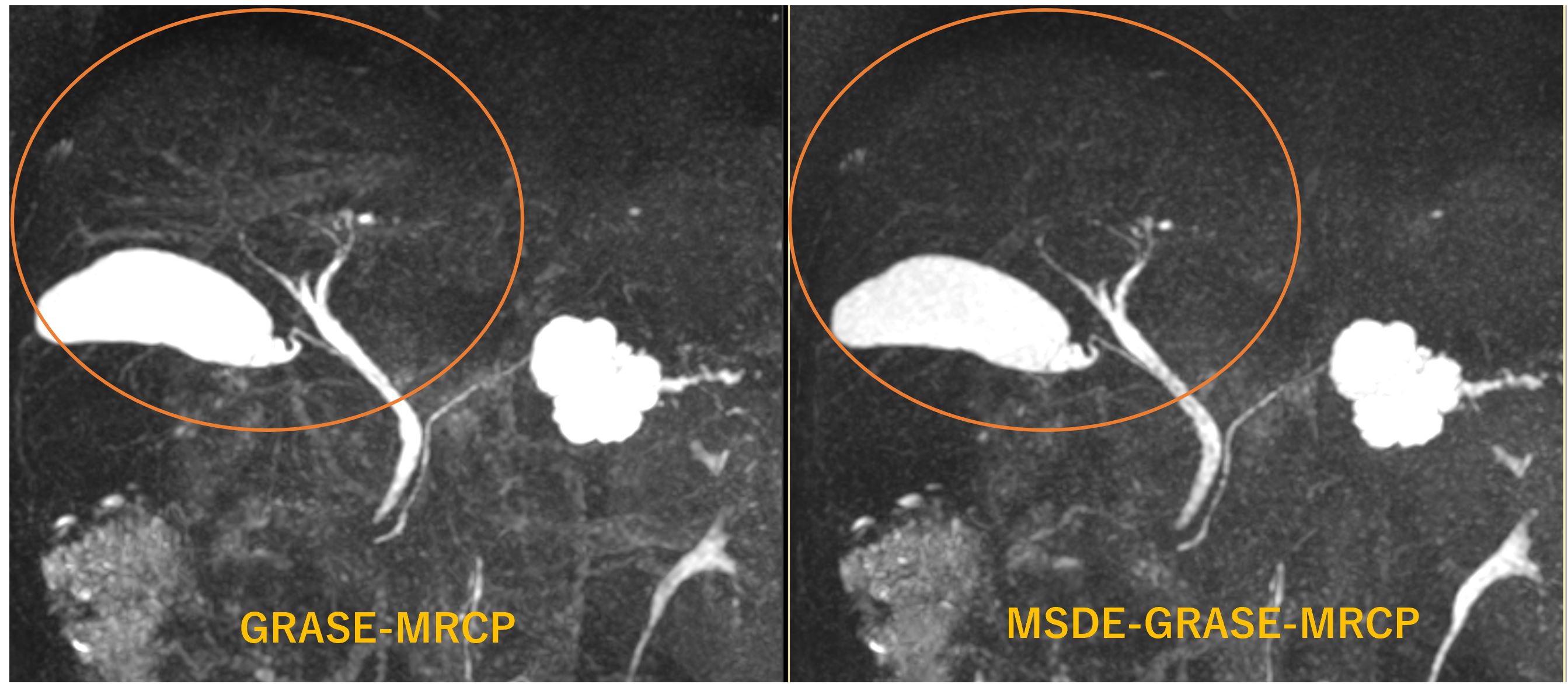
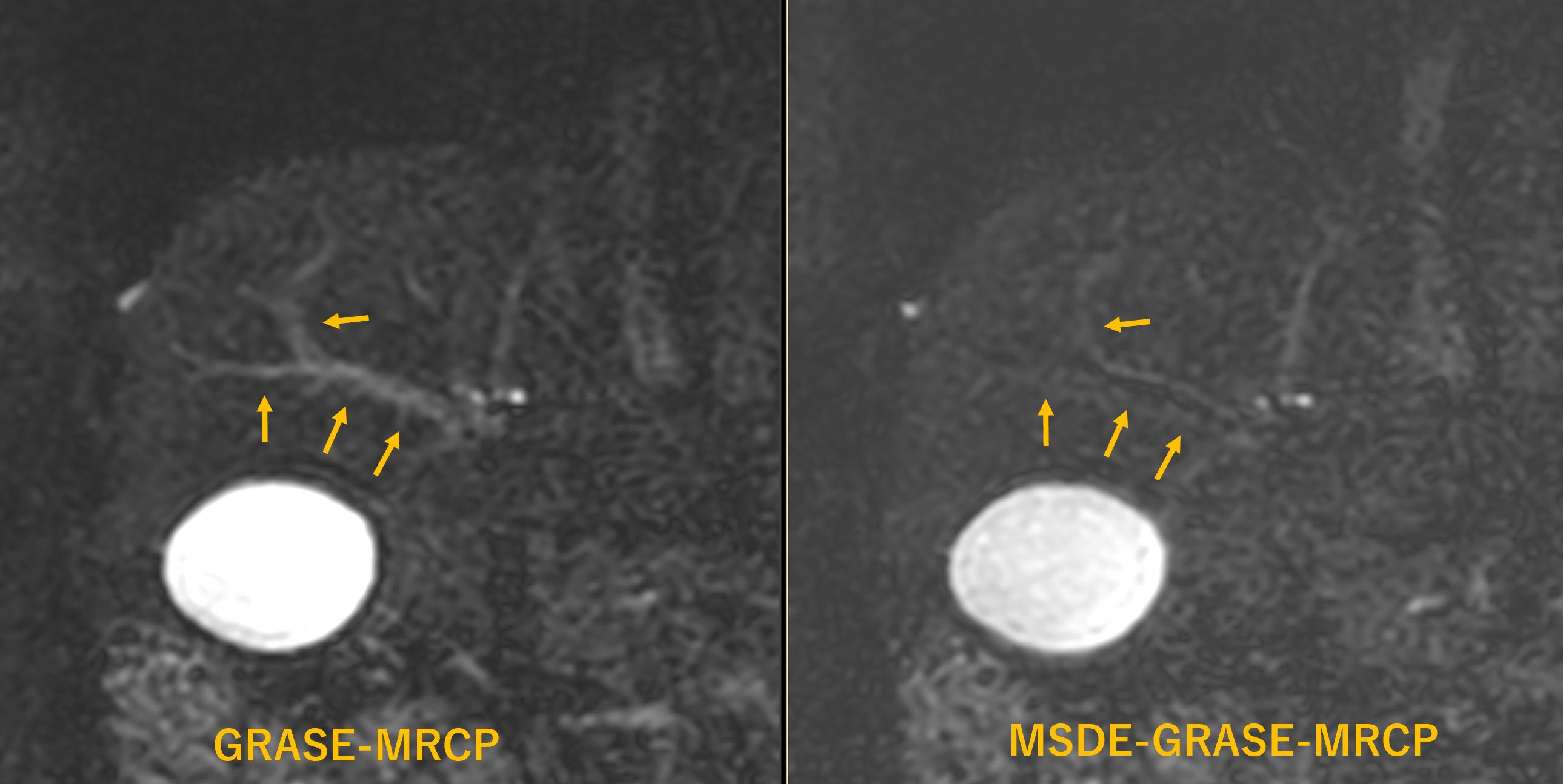
MRCP accelerated with GRASE (GRASE-MRCP) allowed single breath-holding 3D MRCP and better depiction of the cystic duct because of short TE. On the other side, background signal such as blood vessels sometimes remained. Incorporating MSDE into GRASE-MRCP made it possible to suppress the background signals without extending the image time and reducing the image quality.
INTRODUCTION
GRASE is a hybrid sequence that incorporates EPI readout into GRE. By incorporating GRASE into 3D MRCP, the imaging time became brief enough to allow a single breath-hold acquisition. Since TE utilized for GRASE is relatively short as compared to normal FSE-MRCP, even cystic duct filled with concentrated bile is clearly depicted. The drawback is the elevated background signals such as hepatic parenchyma and rephased blood in the vessels that overlap the bile signal. MSDE is one of the Black Blood methods using bipolar gradients to dephase moving protons, which has been used for vessel wall imaging.PURPOSE
In this study, GRASE-MRCP with or without MSDE were compared in terms of the ability to depict biliary tract with an advantage of background signal suppression.METHODS
Thirty-two consecutive patients suspected of having pancreatic or biliary disease were recruited. The patient population included 17 males and 15 females with ages ranging from 20 – 90 (median age of 71). All patients provided written informed consent. All study was performed on 1.5T MR scanner (Prodiva 1.5T CX, Phillips) with torso array coil. Both GRASE-MRCP and MSDE-GRASE-MRCP were operated with TR/TE/FA =330/102/90, slice thickness of 2.4mm (- 1.2mm gap), 67 slices and EPI factor of 7. The image qualites of the overall biliary trees were rated by the 4-point scale. (1, poor; 2, fair; 3, good; and 4, excellent) on the MIP images. The degree of background suppression was also assessed. The depictions of the cystic ducts were rated by 4-point scale. (1, no visualization; 2, <50% visualization; 3, incomplete but ≧ 50% visualization; 4, complete visualization ). The relative contrasts (RC) of the right biliary ducts, left biliary ducts, common biliary ducts and intrahepatic veins were measured. For statistical analysis, the paired t-test, the Wilcoxon signed rank test ere used. Values of p < 0.05 were considered statistically significant.RESULTS
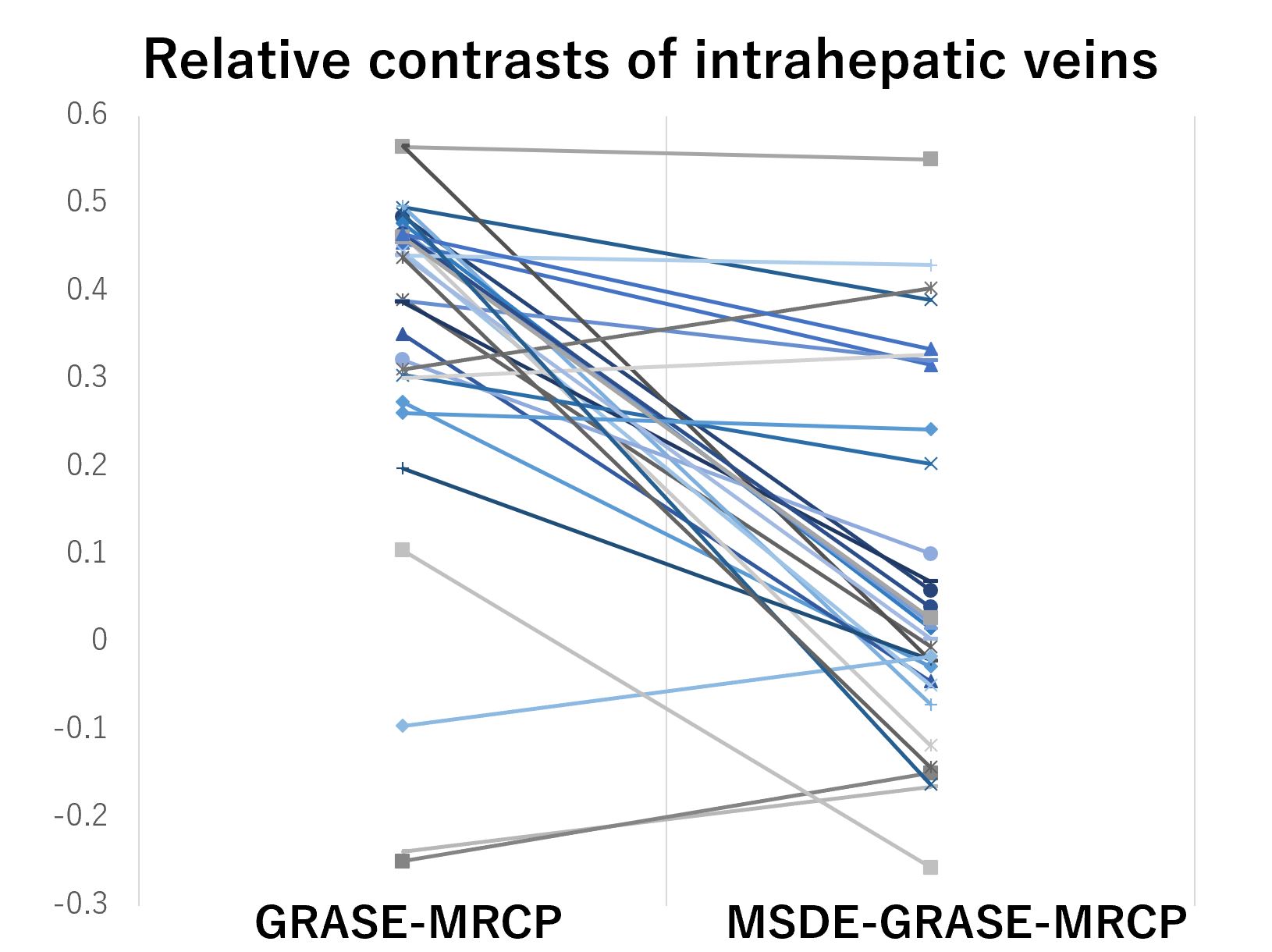
The scan time for both GRASE-MRCP and MSDE-GRASE-MRCP was 18.5 sec. The overall image quality was 3.68 +/- 0.53 for GRASE-MRCP vs. 3.47 +/- 0.62 for MSDE-GRASE-MRCP (p = 0.12). Background suppression was 2.81 +/- 0.78 vs. 3.63 +/- 0.62 (p < 0.01). The depiction of the cystic duct was 3.63 +/- 0.67 vs. 3.67 +/- 0.61 (p = 0.93 ). The RC of the right biliary ducts was 0.78 +/- 0.07 for GRASE-MRCP vs. 0.79 +/- 0.08 for MSDE-GRASE-MRCP (p = 0.77). The RC of the left biliary ducts was 0.80 +/- 0.07 vs. 0.80 +/- 0.07 (p = 0.83). The RC of the common biliary ducts was 0.81 +/- 0.05 vs. 0.82 +/- 0.05 (p = 0.87). The RC of the intrahepatic veins was 0.35 +/- 0.21 vs. 0.82 +/- 0.08 (p < 0.01)DISCUSSION
On MSDE-GRASE-MRCP images, intrahepatic portal vein and hepatic vein signals were actively suppressed compared to GRASE-MRCP, which made the background signals inconspicuous. There was no significant difference in image quality on visual evaluation, and there was no difference in the ability to depict the cystic duct. MSDE is a practical option for GRASE-MRCP with an added value of background suppression for no extended imaging time.CONCLUSION
MSDE is a practical option for GRASE-MRCP with an added value of background suppression and increased biliary duct conspicuity for no extended imaging time.Acknowledgements
No acknowledgement found.References
1. Nam JG, Lee JM, Kang HJ, et al. GRASE Revisited: breath-hold three-dimensional (3D) magnetic resonance cholangiopancreatography using a Gradient and Spin Echo (GRASE) technique at 3T. Eur Radiol. 2018 Sep;28(9):3721-3728.
2. Yoshida M, Nakaura T, Inoue T, Tanoue S, et al. Magnetic resonance cholangiopancreatography with GRASE sequence at 3.0T: does it improve image quality and acquisition time as compared with 3D TSE? Eur Radiol. 2018 Jun;28(6):2436-2443.
Figures