2507
DCE-MRI with a free-breathing compressed sensing VIBE for pancreatic ductal adenocarcinoma: correlation with ECV fraction1Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan, 2Siemens Healthcare K.K., Tokyo, Japan, 3Siemens Healthcare, Erlangen, Germany
Synopsis
This study focused on the feasibility of dynamic contrast-enhanced MRI (DCE-MRI) with compressed sensing T1-weighted volumetric interpolated breath-hold examination (csVIBE) for pancreatic ductal adenocarcinoma (PDAC) and correlation with extracellular volume fraction (ECV). Our results indicated that DCE-MRI obtained with csVIBE is feasible for the assessment of PDACs and the ECV fraction can be used in place of DCE-MRI parameters for predicting treatment response or survival in patients with PDAC.
Introduction
Recently, a prototype of the T1-weighted volumetric interpolated breath-hold examination (VIBE) sequence has been developed, which supports compressed sensing (csVIBE) and free-breathing acquisitions. However, the feasibility of a free-breathing csVIBE with motion-resolved reconstruction for dynamic contrast-enhanced MRI (DCE-MRI) has not been elucidated.The extracellular volume fraction (ECV) fraction and DCE-MRI has been used for prognostic biomarkers of pancreatic ductal adenocarcinoma (PDAC) [1-3]. Compared with DCE-MRI, the oncological assessment using ECV fraction as determined by unenhanced and equilibrium contrast-enhanced MRI is easier to calculate without significant post-processing time. To our knowledge, however, no study regarding the relationship between ECV fraction within PDACs and pharmacokinetic parameters obtained with DCE-MRI has yet been performed.
Purpose
The purpose of this study was to assess the feasibility of DCE-MRI with a free-breathing csVIBE and motion-resolved reconstruction for PDAC and the correlation with ECV fraction.Methods
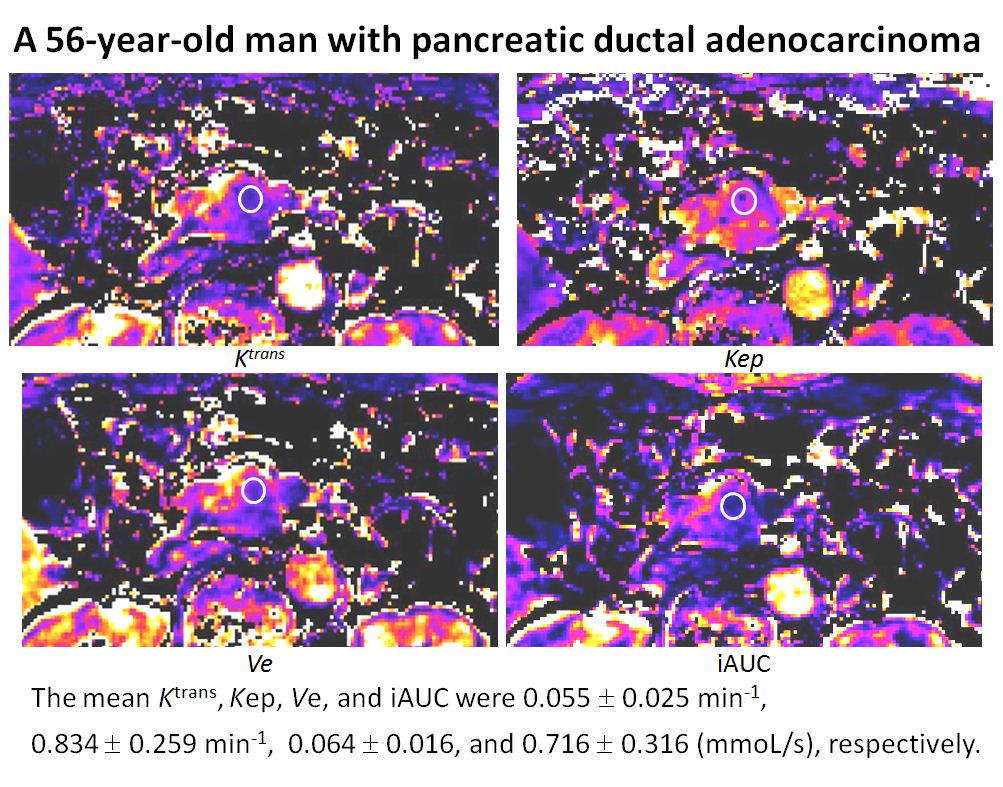
Forty-four patients with PDAC (mean size, 29.8 mm; size range, 12–72 mm) underwent Gd-EOB-DTPA-enhanced MRI. DCE-MRI was obtained using a prototype sequence of free-breathing csVIBE with motion-resolved reconstruction (TR/TE, 3.9/1.4 ms; flip angle, 12°; matrix size, 151 x 288; slice thickness, 2.5 mm; FOV, 360 mm; slice number, 88; compressed sensing factor, 6; temporal resolution, 10 sec; acquisition time, 320 s). Pharmacokinetic parameters of DCE-MRI including Ktrans, Kep, Ve, and iAUC were calculated inline (Fig. 1). For T1 mapping, modified Look-Locker inversion recovery sequences using single-shot steady-state free precession readout (repetition time, 2.7 ms; echo time, 1.12 ms; flip angle, 35°; inversion time, 14 points; number of inversion puls, 2; recovery duration, 4000 ms; acceleration factor, 2; field of view, 350 mm; matrix, 192 x 256; thickness, 10 mm; acquisition time, 9.7 s; number of slice, 1) were performed before and 5 min after Gd-EOB-DTPA administration. ECV fraction of tumor was calculated using the following formula: ECV= (1-Hct) x [R1 (tumor pre) - R1 (tumor 5min)] / [T1 (aorta pre) - R1 (aorta 5min)]. Where R1 = 1/T1; R1 (tumor pre) and R1 (tumor 5min) are R1 values of the tumor before and 5 min after Gd-EOB-DTPA administration, respectively; R1 (aorta pre) and R1 (aorta 5min) are R1 values of the aorta before and 5 min after Gd-EOB-DTPA administration, respectively. Spearman’s bivariate correlation was used to assess the relationship between ECV fraction and pharmacokinetic parameters of DCE-MRI.Results
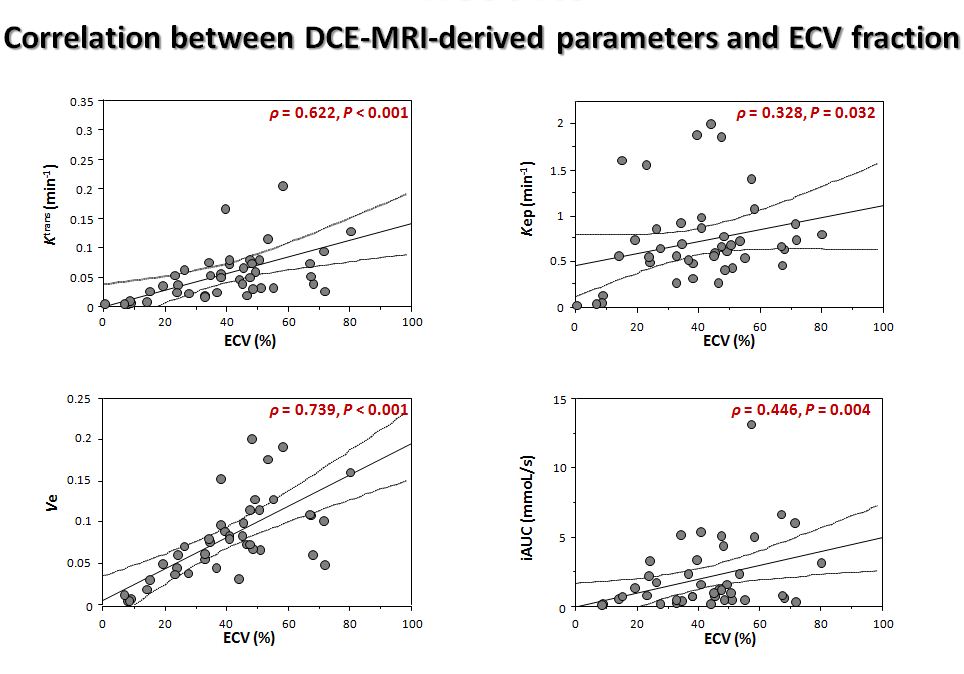
The mean tumor ECV fraction, Ktrans, Kep, Ve, and iAUC of PDAC were 39.9%, 0.053 min-1, 0.713 min-1, 0.079, and 1.574 mmoL/s, respectively. Tumor ECV fraction showed a significant positive correlation with Ktrans (P < 0.001, ρ= 0.622), Kep (P = 0.032, ρ= 0.328), Ve (P < 0.001, ρ= 0.739), and iAUC (P = 0.004, ρ= 0.446) (Fig. 2).Discussion
Our results of pharmacokinetic parameters were similar to those of a previous study with DCE-MRI obtained with the radial k-space sampling gradient-echo sequence with k-space–weighted image contrast in which tumor Ktrans, Kep, Ve, and iAUC values were 0.042 min-1, 0.761 min-1, 0.080, and 2.841 mmoL/s, respectively [4]. Therefore, DCE-MRI obtained with a free-breathing csVIBE and motion-resolved reconstruction may be feasible for the assessment of PDACs.Previous researches reported the Ktrans can predict tumor response to chemotherapy, radiotherapy, or angiogenic therapy in PDAC patients [2, 3]. The Ve has the potential to predict the response to chemotherapy or prognosis in patients with neck tumor, rectal cancer, and osteosarcoma [5]. However, the use of DCE-MR imaging is technically demanding and requires multiple repeat studies and complex post-processing steps that are difficult to perform in routine clinical studies.
Our results showed a significant positive correlation of tumor ECV fraction with Ktrans and Ve. The ECV fraction is the sum of Ve and intravascular space fraction. The contribution of the intravascular space fraction to the total attenuation in PDAC can be ignored because PDAC is known to be a hypovascular tumor, which is reflected by the small intravascular component in the tumor. Previous researchers also reported the positive correlation between Ktrans and Ve within PDAC [6]. Therefore, the ECV fraction within PDAC could offer an alternative imaging biomarker to the Ktrans and Ve obtained with DCE-MRI.
Conclusion
DCE-MRI obtained with a free-breathing csVIBE and motion-resolved reconstruction may be feasible for the assessment of PDACs. ECV fraction could offer an alternative imaging biomarker predicting the response to chemotherapy or prognosis in patients with PDAC.Acknowledgements
No acknowledgement found.References
1. Fukukura Y, et al. Extracellular volume fraction determined by equilibrium contrast-enhanced multidetector computed tomography as a prognostic factor in unresectable pancreatic adenocarcinoma treated with chemotherapy. Eur Radiol. 2019; 29:353-61.
2. Park MS, et al. Perfusion CT: noninvasive surrogate marker for stratification of pancreatic cancer response to concurrent chemo- and radiation therapy. Radiology. 2009;250:110-7.
3. Akisik MF, et al. Pancreatic cancer: utility of dynamic contrast-enhanced MR imaging in assessment of antiangiogenic therapy. Radiology. 2010;256:441-9.
4. Kim JH, et al. Solid pancreatic lesions: characterization by using timing bolus dynamic contrast-enhanced MR imaging assessment: a preliminary study. Radiology. 2013;266:185-96.
5. Tong T, et al. Dynamic contrast-enhanced MRI: Use in predicting pathological complete response to neoadjuvant chemoradiation in locally advanced rectal cancer. J Magn Reson Imaging. 2015;42:673-80.
6. Klaassen R, et al. Repeatability and correlations of dynamic contrast enhanced and T2* MRI in patients with advanced pancreatic ductal adenocarcinoma. Magn Reson Imaging. 2018;50:1-9.
Figures