2446
Tumor Estimation for PI-RADS v2 Assessment of Prostate Cancer using Multiparametric MRI1Centre for Biomedical Engineering, Indian Institute of Technology (IIT) Delhi, New Delhi, India, 2Delhi Technological University, Delhi, India, 3Department of NMR, All India Institute of Medical Sciences Delhi, New Delhi, India, 4Department of Radiology, All India Institute of Medical Sciences Delhi, New Delhi, India, 5Department of Biomedical Engineering, All India Institute of Medical Sciences Delhi, New Delhi, India
Synopsis
Accurate estimation of tumor size is a challenging task due to the large variation in shape of prostatic tumors. Measurement of diameter and volume of tumor are useful for the staging of prostate cancer(PCa). Therefore, an appropriate method for tumor assessment is essential to assist clinical management of PCa. The goal of this study was to investigate the role of tumor size estimation methods (2D vs. 3D) for the Prostate Imaging Reporting and Data System version-2(PI-RADS v2) assessment of PCa using multiparametric MRI. Automatic tumor size assessment using ellipse-fitting approach showed relatively better performance of PCa assessment compared to radiologist-assessment.
Introduction
Prostate cancer (PCa) is the fifth leading cause of cancer death among men worldwide.1 Multiparametric-MRI(mpMRI) [T2-weighted(T2w) imaging,diffusion-weighted imaging (DWI),its derivative apparent-diffusion-coefficient (ADC),and dynamic contrast-enhanced(DCE) MRI, etc.] have significantly improved the diagnostic accuracy of PCa.2 PI-RADS v2 helps to identify clinically significant PCa using mpMRI and therefore,can aid in clinical decisions regarding treatment.3 Tumor estimation plays an essential role in automated diagnosis of PCa.4 Based on the current uses of mpMRI,any tumor having longest-diameter>1.5cm,volume>0.5cc,and PI-RADS v2 score>3, is a high-grade cancer.4 PI-RADS v2 follows the 2D-approach for tumor marking and estimation. The creation of 3D prostate tumor mask could assist with radiotherapy treatment planning and for correlative pathology-imaging research.5 The objective of this study was to develop method for automated estimation of maximum tumor-dimension in both 2D and 3D;where in 3D the maximum-diameter could be in an oblique plane also. The major-axis of best-fit ellipse in 2D and ellipsoid in 3D was used as the longest-dimension of tumor and evaluated for automated assessment of PI-RADS v2.Methods
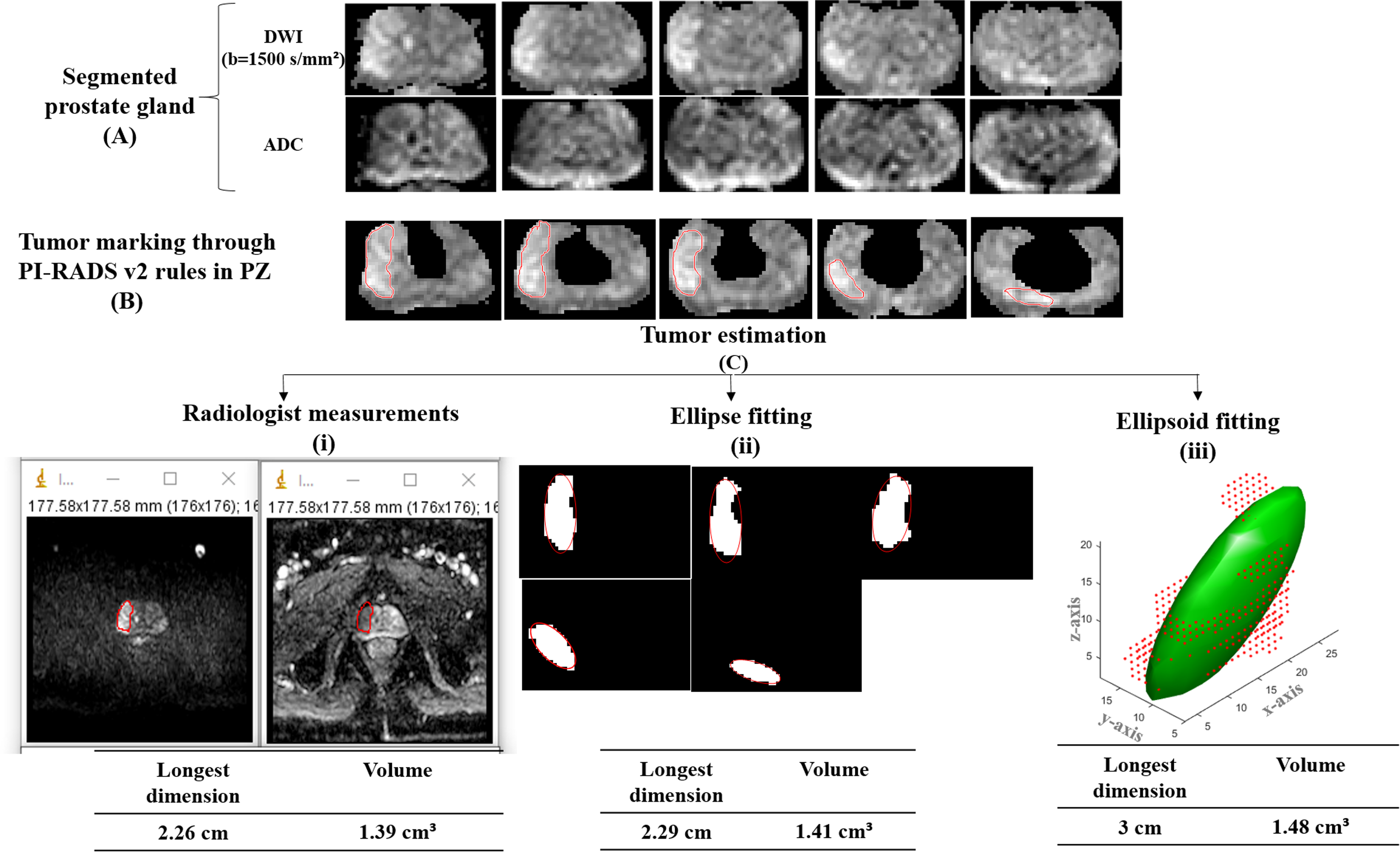
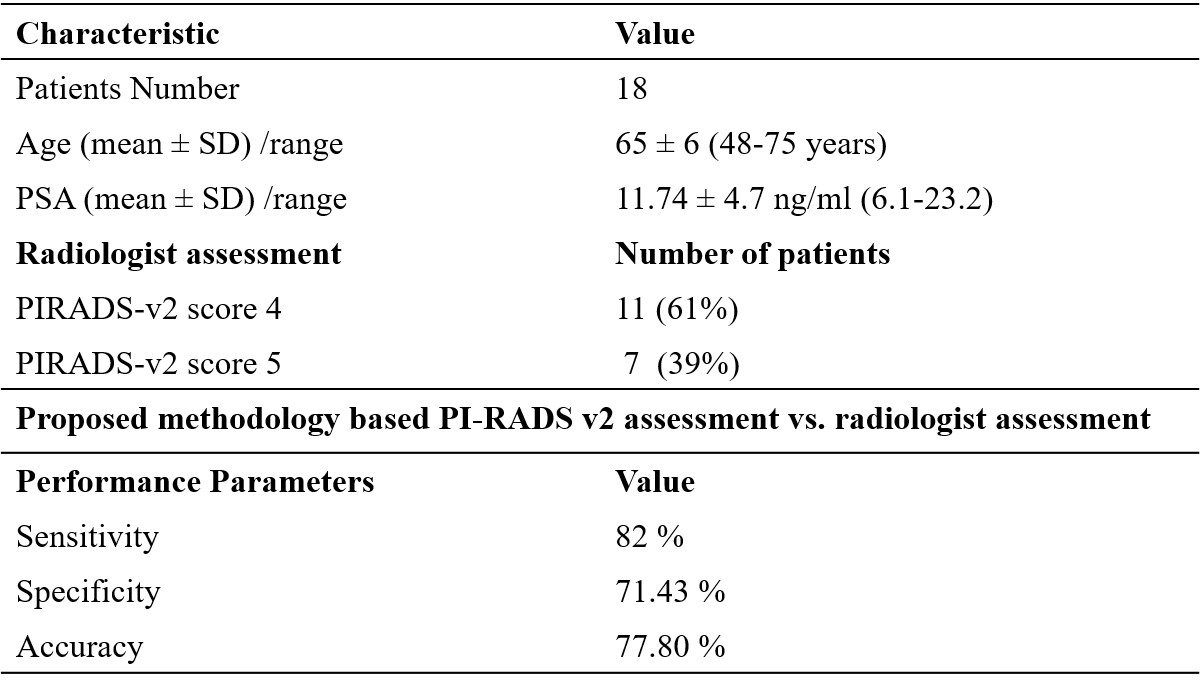
MRI data acquisition: A retrospective mpMRI dataset from 18 patients of PCa was used in this study. All prostate mpMRI examinations were acquired using a 3T MRI system (Ingenia,Philips,The Netherlands) using an external phased-array body coil. MRI sequences included axial turbo-spin-echo(TSE) T2w(TR/TE=3715/100ms;slice-thickness=3mm;field-of-view(FOV)=160×160mm2;acquisition matrix=400×400;number-of-slices=30) and echo-planar DWI(TR/TE=5521/75 ms; FOV=177.6×177mm2; acquisition-matrix=176×176;slice-thickness=4mm; number-of-slice =30;with four b-values of 0,500,800 and 1500s/mm2).Methodology: Data were processed using in-house developed codes in MATLAB-R2018a. In the pre-processing step,prostate-gland and zonal segmentation,6 ADC calculation, and 3D-affine registration were performed. Region of interest (ROI) of segmented prostate zones for T2w, high b-value DWI and ADC was extracted for tumors-marking. Tumors-marking was performed as per PI-RADS v2 guidelines with the help of expert radiologist(>10 years of experience in prostate imaging)
Tumor estimation methods: Based on the qualitative-classification,tumor configuration was divided into two categories: ellipsoid and non-ellipsoid shape. The tumor-size and volume were measured from 2D and 3D methods for estimation purpose.
Radiologist-measurements: The size and volume were measured within ROIs outlined by the expert radiologist on DWI and ADC maps. The analysis was done using image processing software (ImageJ,version-1.48, National Institute of Health,Bethesda,Md).
Ellipse-fitting: The dimension and volume of tumor were assessed in each MRI slices by 2D ellipse-fitting approach. The major-axis of the ellipse was computed as the longest-diameter of the tumor. Volume was calculated by the summation of all tumor areas in each slice and multiplication by slice-thickness.
Ellipsoid-fitting: The 2D-axial slices were stacked to form a 3D volume. Ellipsoid-fitting approach was used to best-fit the 3D anatomy of the tumor in any direction;calculating the major-axis of the best-fit ellipsoid as the longest-diameter. Volume of the ellipsoid was also calculated.
Based on tumor measurements, accuracy was calculated for PI-RADS v2 assessment of PCa compared to radiologist’s assessment. The workflow of our proposed methodology is shown in fig-1.
Results
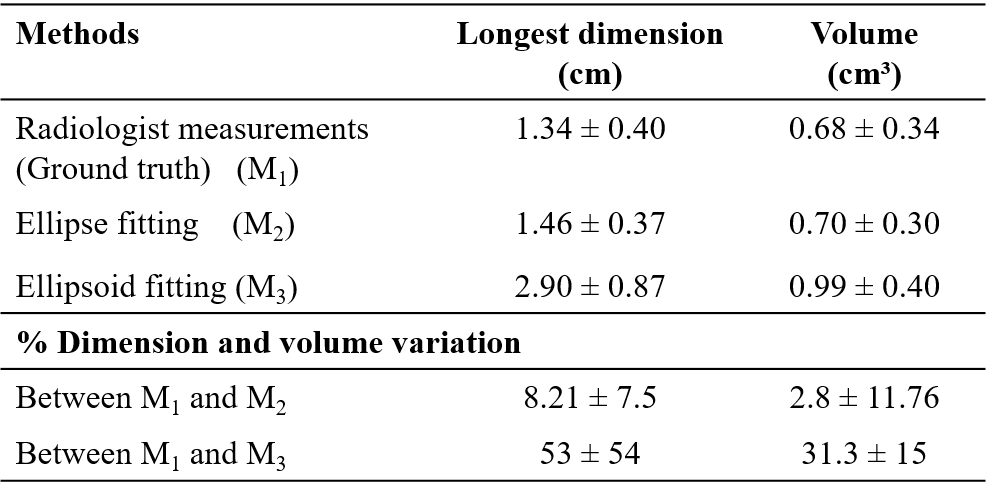
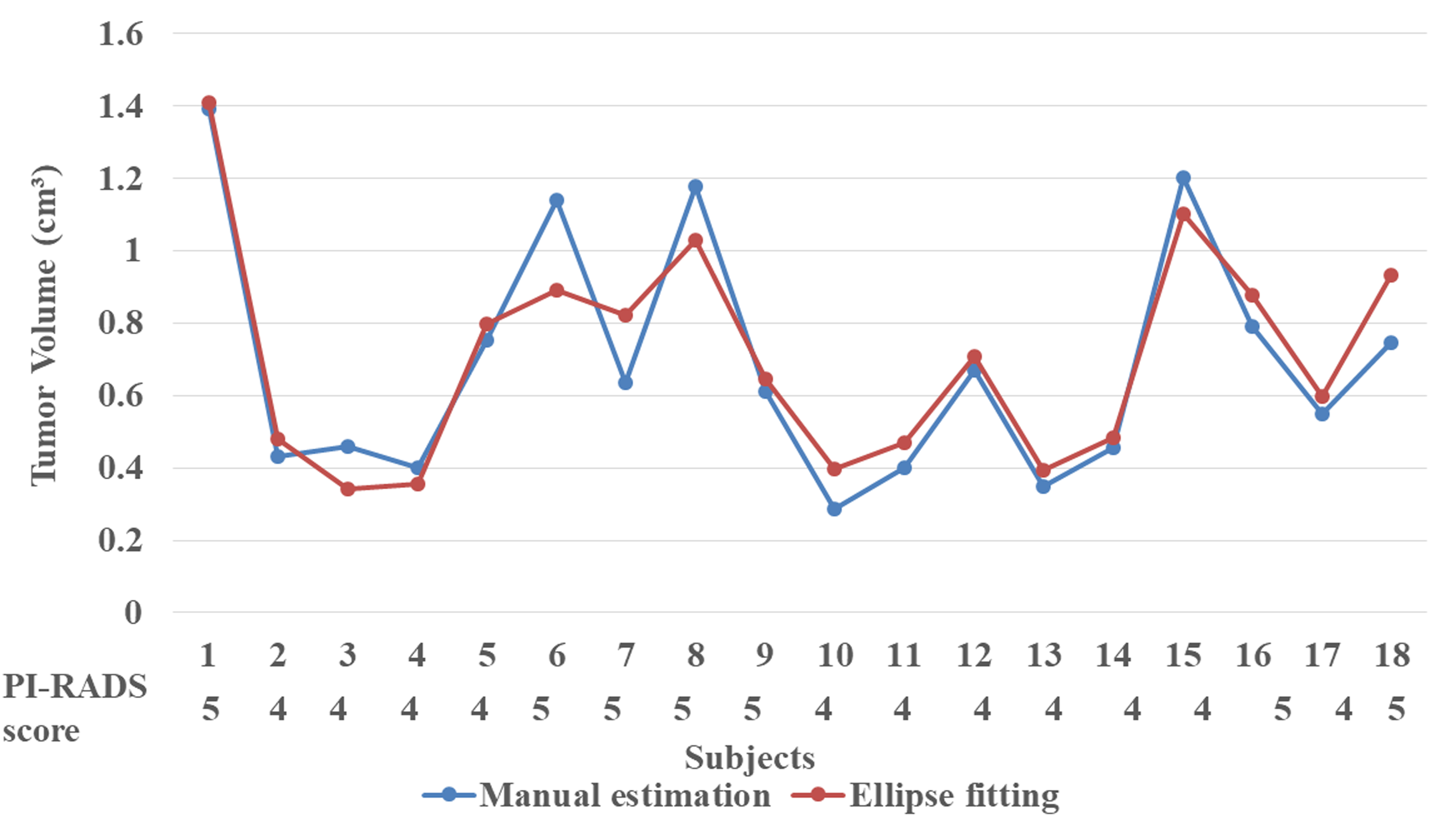
Fig-2 shows the tumor-estimation results of one patient(age=58years). The measurement of longest-dimension and volume of tumor using proposed 2D and 3D methods comparison with radiologist measurements using ImageJ software is shown in table-1. The longest-dimension and volume of tumor(mean±SD) from 18 subjects were 1.34±0.40cm and 0.68±0.34cm3 by radiologist,1.46±0.3cm and 0.70±0.30cm3 using ellipse-fitting,and 2.90±0.87cm and 0.99±0.40cm3 using ellipsoid fitting. The percentage of variation in dimension and volume between radiologist-measurement and ellipse-fitting were small(8.21±7.5%and 2.8±11.76%,respectively) compared to ellipsoid-fitting measurements(53±54% and 31.3±15%,respectively). Ellipse-fitting tumor-estimation based PI-RADS v2 assessment showed sensitivity,82%;specificity,71.43%;accuracy,77.80% compared to radiologist-assessment(table-2). Ellipsoid-fitting tumor-estimation based PI-RADS v2 assessment against radiologist-assessment showed large variation in sensitivity and specificity. All the patients(n=11) with grade-4 using radiologist-assessment were graded as grade-5 with ellipsoid-fitting approach. The variation of tumor-volume(from radiologist-measurement and ellipse-fitting method) with PI-RADS v2 scores is shown in fig-3.Discussion
Accurate non-invasive measurement of prostate tumor could significantly improve the determination of tumor-prognosis and assist in PI-RADS v2 assessment. Few prostate tumor-estimation methods have been presented in the past.7-9 In this study,2D ellipse-fitting and 3D ellipsoid-fitting approach were developed for tumor-estimation. Expert radiologist marked the tumor as considered as ground-truth. The tumor measurements between radiologist and ellipse-fitting were found similar,because PI-RADS v2 follows the 2D approach for tumor-marking and estimation. The ellipsoid-fitting method showed significantly higher values for the tumor-dimension and volume as compared to radiologist-measurement. In the literature few studies so far evaluate PI-RADS v2 for diagnosis of PCa;the pooled sensitivity and specificity were 85-89% and 71-73%,respectively.10,11 Based on the ellipse-fitting tumor-estimation method, proposed methodology has observed relatively better sensitivity,82%;specificity,71.43%;and accuracy,78% compared to radiological PI-RADS v2 assessment. As found in our study with ellipsoid-fitting approach all the patients with grade-4 were marked as grade-5,because of higher tumor-diameter. This led us to a bigger concern, if longest tumor-diameter is in oblique plane as estimated by ellipsoid approach then the grade of tumor can also change having potential impact on treatment plan as well. In future study, we intend to evaluate and validate this approach in a large number of patients towards improving the accuracy of proposed framework.Conclusion
The proposed automated framework based on 2D ellipse-fitting showed good agreement with radiologist-assessment, which might help to make the analysis process time-efficient. 3D tumor estimation can provide complementary information to clinicians compared to traditional methods due to multidimensional visualization, which needs further investigation.Acknowledgements
This work is supported by IIT Delhi, India and AIIMS New-Delhi, India. DS was supported with the research fellowship fund from the Ministry of Human Resource Development, Government of India.References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA CANCER J CLIN. 2018; 68: 394-442.
2. Mertan FV, Berman R, Szajek K, et al. Evaluating the Role of mpMRI in Prostate Cancer Assessment. Expert Review of Medical Devices. 2016; 13(2):129-141.
3. Park SY, Cho NH, et al. Prostate Imaging-Reporting and Data System Version 2: Beyond Prostate Cancer Detection. Korean J Radiol. 2018; 19(2):193–200.
4. Weinreb JC , Barentsz JO, Choyke PL, et al. PI-RADS Prostate Imaging Reporting and Data System: 2015, Version 2. European Urology. 2016; 69(1):16-40.
5. Malone SC, Haridass A, Nyiri B, et al. Creation of 3-dimensional prostate cancer maps: methodology and clinical and research implications. Arch Pathol Lab Med. 2014;138(6) :803-808.
6. Singh D, Kumar V, et al. Gland and Zonal Segmentation of Prostate using Diffusion-Weighted MR Imaging, Proc. Intl. Soc. Mag. Reson. Med. 2019; 27.
7. Perera M, Lawrentschuk N, Bolton D, et al. Comparison of contemporary methods for estimating prostate tumour volume in pathological specimens. BJU Int. 2014; 113(2):29-34.
8. Bratan F, Melodelima C, Souchon R, et al. How Accurate Is Multiparametric MR Imaging in Evaluation of Prostate Cancer Volume? Genitourinary Imaging. 2014; 275(1):144-154.
9. Priester A, Natarajan S, Khoshnood P, et al. Magnetic Resonance Imaging Underestimation of Prostate Cancer Geometry: Use of Patient Specific Molds to Correlate Images with Whole Mount Pathology. J Urol. 2017; 197(2): 320–326.
10. Woo S, Suh CH, Kim SY, et al. Diagnostic performance of prostate imaging reporting and data system version 2 for detection of prostate cancer: a systematic review and diagnostic meta-analysis. Eur Urol. 2017; 72:177-188.
11. Zhang L, Tang M, Chen S, et al. A meta-analysis of use of prostate imaging reporting and data system version 2 (PI-RADS V2) with multiparametric MR imaging for the detection of prostate cancer. Eur Radiol. 2017; 27:5204-5214
Figures