2428
Interobserver agreement of the PI-RADS Version 2.1 lexicon: A Multicenter Study of Six Radiologists with different levels of experience
Li Zhang1, Longchao Li1, Min Tang1, Yinzhong Wang2, and Xiaoyan Wang2
1Department of MRI, Shaanxi Provincial People’s hospital, Xi’an, China, 2Lanzhou university First Hospital, Lanzhou, China
1Department of MRI, Shaanxi Provincial People’s hospital, Xi’an, China, 2Lanzhou university First Hospital, Lanzhou, China
Synopsis
PI-RADS Version 2.1 makes several minor modifications aimed at addressing these issues and simplifying the scoring system without changing the overall framework for acquisition or interpretation using the principles of the dominant sequence paradigm. Formal investigations of the Interobserver agreement of the PI-RADS version 2.1 scoring system are critical to confirm that it is attaining its primary aim of standardization.
BACKGROUND
PI-RADS version 2 has been widely adopted and tested in clinical practice. However, experience has highlighted ambiguities in the scoring and limitations in relation to inter-reader reproducibility. Version 2.1 recommends several minor adjustments aimed at simplifying assessment and reducing inter-reader variability, without changing the overall scope or principles of the original system.PURPOSE
To determine the interobserver agreement of PI-RADS version 2.1 lexicon among six radiologists from different institutions with varying levels of experience. Such investigations would greatly benefit from a multicenter approach given the potential greater propensity for readers from a single institution to have a similar approach to image assessment, a tendency that would bias the analysis. Evaluation of interobserver agreement of the version 2.1 lexicon is important to validate the uniformity of this widely used classification.METHODS
This retrospective study was institutional review board–approved. Six radiologists from three separate institutions, different experienced in prostate magnetic resonance (MR) imaging, assessed prostate MR imaging examinations performed at a single center by using the PI-RADS version 2.1.Six radiologists (two highly experienced, two moderately experienced, and two less experienced) independently read 245 lesions in the peripheral zone (PZ) and 197 lesions in the transition zone (TZ), blinded to clinical MRI indication and biopsy results. First-order agreement coefficient (AC1) was used to evaluate interobserver agreement. Percentage of concordance, k coefficients were also computed.RESULTS
Agreement for PI-RADS version 2.1 score of 4 or greater was 0.56 in peripheral zone (PZ) and 0.48 in transition zone (TZ). From the features evaluated on PZ lesions, definite extraprostatic extension (EPE)/invasive behavior on T2WI, DCE positive, size had good agreement (AC1 = 0.62-0.80), and the others had moderate to substantial for features agreement (AC1 = 0.48–0.58). In TZ, four had good agreement: definite EPE/invasive behavior (AC1 = 0.79), Encapsulated (AC1=0.62), and moderate hypointensity (AC1 = 0.68) on T2WI, size (AC1=0.63). Focal (vs indistinct) shape on DWI and ADC map, and marked hypointensity on ADC map/DWI (AC1 = 0.48 to 0.56) had moderate agreement, whereas heterogeneous and circumscribed (not obscured margins) on T2WI (AC1 = 0.39 to 0.48) had fair agreement. All six features in the PZ had worse agreement among less experienced readers as compared with highly and moderately experienced readers. As to nine features considered in TZ, less experienced readers had worse agreement than highly and moderately experienced readers in marked hyperintensity on high b-value DWI, marked hypointensity on ADC map, definitive EPE/invasive behavior on T2WI, focal (not indistinct) on DWI and ADC map, and size.CONCLUSION
Interobserver agreement in PI-RADS version 2.1 lexicon ranges from moderate to good among radiologists and improves with increasing experience, and neither required nor benefitted from a training session. Agreement tended to be better in PZ than TZ.Acknowledgements
No acknowledgement found.References
No reference found.Figures
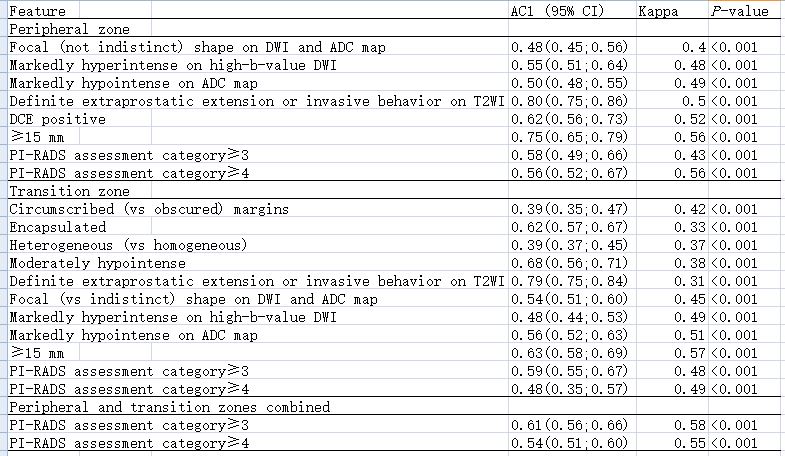
TABLE 1. Concordance Analysis Among Six
Reader