2416
Differentiate benign prostatic hyperplasia and prostatic cancer using APTw imaging and DKI Imaging1The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Philips Healthcare, Beijing, China
Synopsis
The present study aimed to explore the value of amide proton transfer-weighted (APTw) imaging combined with diffusional kurtosis imaging (DKI) in the differential diagnosis between benign prostatic hyperplasia (BPH) and prostatic cancer. The results showed that the combined technique had a good diagnostic effect. When APT value was combined with 3 DKI parameters (FA, MK, Ka), the diagnostic efficacy significantly enhanced (AUC: 0.872; sensitivity: 76.5%; specificity: 90.9%).
Introduction
Amide proton transfer-weighted (APTw) imaging, which is a molecular MRI tool based predominantly on endogenous substance in tissue, namely the amide protons in mobile cellular proteins and peptides[1], has showed great value in diagnosing cervical cancer in previous study[2]. Diffusional kurtosis imaging (DKI) is advanced diffusion techinique and can reflect tissue complexity in cancer tissue. DKI has been demonstrated for great benefit in the differential diagnosis of prostate cancer, benign prostatic hyperplasia (BPH), and benign periphera zone (PZ)[4]. Thus, We combined the APTw valuses and the fractional anisotropy (FA), mean kurtosis (MK) and axial kurtosis (AK) derived from DKI to identify prostatic cancer from benign prostatic hyperplasia.Materials and Methods
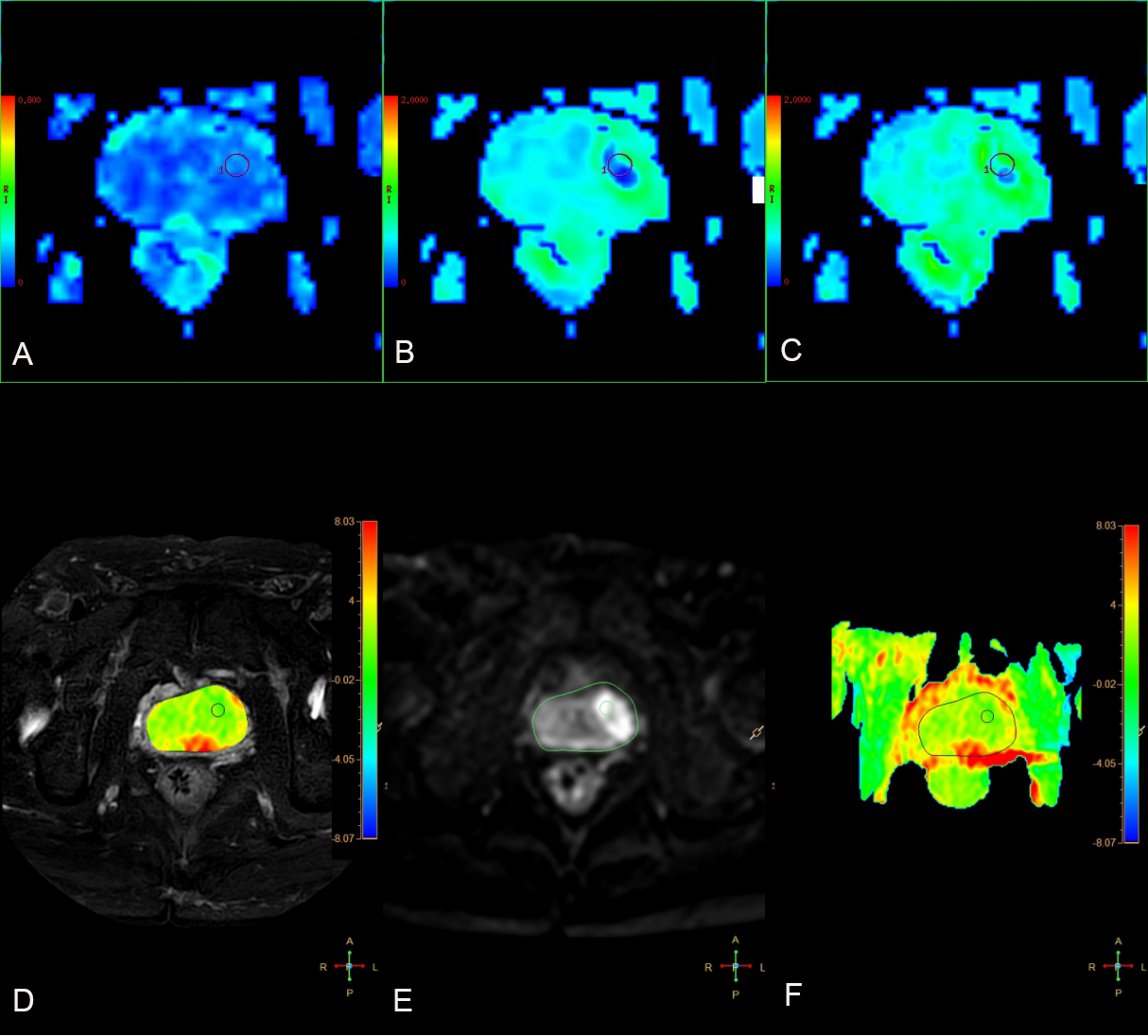
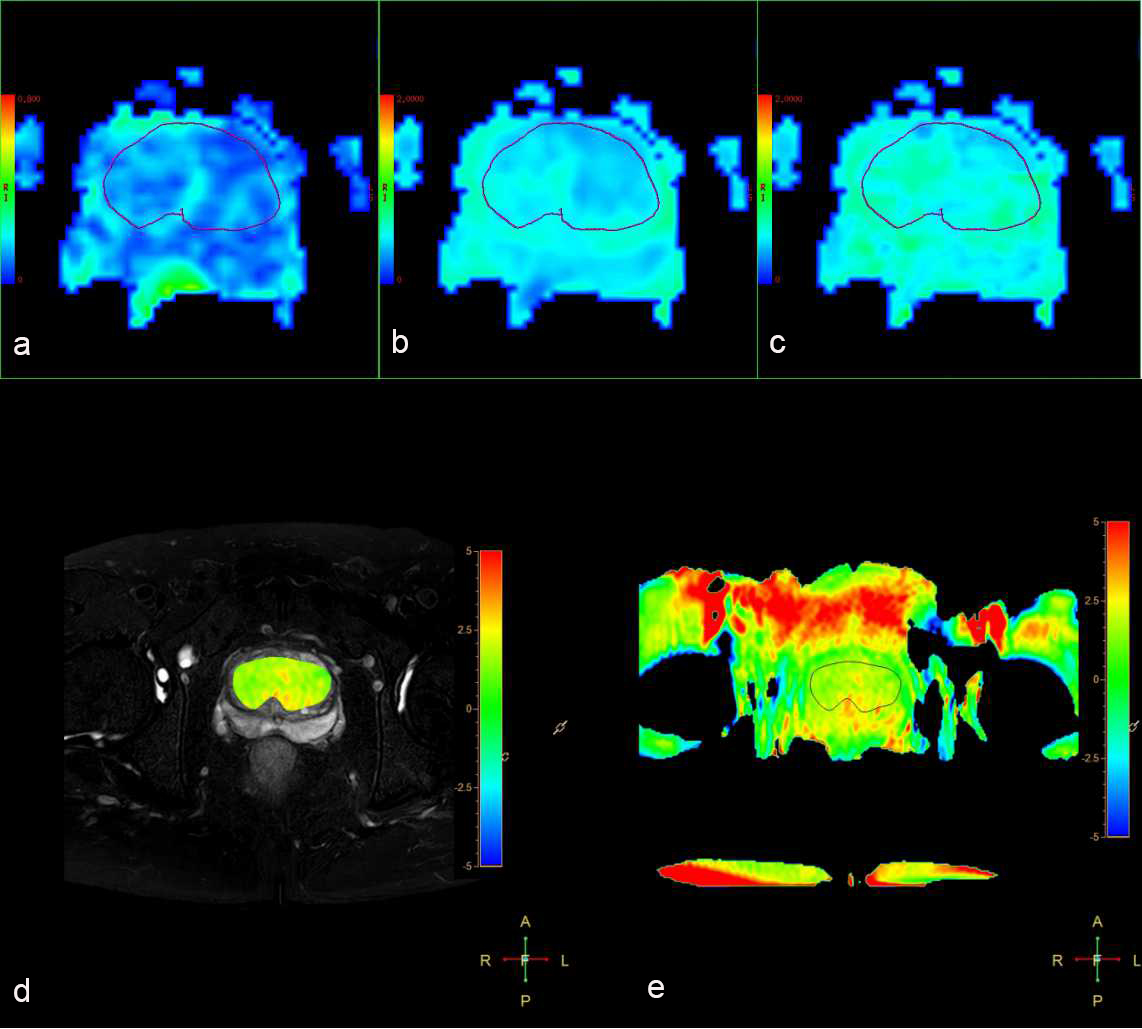
Our hospital retrospectively analyzed 39 patients with prostate disease, including 22 cases of benign prostatic hyperplasia (66.32±9.96) and 17 cases of prostatic cancer (69.06±7.17). T1w TSE, T2w-SPAIR TRA, DWI, APT and DKI were performed on a 3.0T MR scanner (Ingenia CX, Philips) (Table 1). In benign prostatic hyperplasia, ROIs were placed on the axial slice showing the largest area of the prostate referring to T2w images, and then were applied to APTw images and each parameter images of DKI by two radiologists independently (Figure 1). In prostatic cancer, ROIs were placed on the axial slice showing the largest area of lesion based on DWI and T2w images by the same radiologists independently, and also transferred to APTw and DKI parameter maps (Figure 2). we calculated the average APTw values and the mean values of MK, AK, FA within ROIs. The intra-class correlation coefficients (ICC) was used to evaluate APTw and DKI for each parameter values measured by the two radiologists using SPSS platform(IBM),. Due to all the data of image parameters were normally distributed, we used independent-sample T test in the analysis of prostate cancer and BPH. Logistic regression was used to calculate the value of APT combined with DKI parameters in the diagnosis of benign and malignant prostatic lesions, and ROC curve was used to evaluate the diagnostic performance of the above parameters in benign and malignant prostatic lesions identification.Result
There was a good agreement between the two observers. ICC with APTw, FA, MK and AK were 0.896, 0.941, 0.918, 0.885 in benign prostatic hyperplasia, and 0.958, 0.968, 0.974, 0.975 in prostatic cancer, respectively. According to independent-sample T test, APTw, FA, MK and AK were all statistically difference between BPH and PCa (Table 2). The values of all the parameters in PCa were significant higher than those of BPH(p<0.05). The area under the curve (AUC) of APTw, FA, MK and AK was 0.723, 0.680, 0.703, 0.845 respectively. The AUC of the combination of APTw, MK was 0.775, sensitivity was 64.7%, specificity was 90.9%. The AUC of the combination of APTw, FA, MK was 0.813, sensitivity was 58.5%, specificity was 95.5%. The combination of APTw, FA, MK, AK showed the optimal diagnostic efficiency, for which the AUC was 0.872, sensitivity was 76.5, specificity was 90.9 %(Table 3).Discussion
The combination of APTw, FA, MK, AK performed the optimal diagnostic efficiency for identifying PCa from BPH. The combination of multi-parameters MRI,including APT and DKI techiniques had a great clinical value in the differential diagnosis of BPH and PCa. However, the diagnostic value of AK was the highest diagnostic performance (AUC: 0.845; sensitivity: 88.2%; specificity: 77.3%) among the single parameter and even higher than that of the combination of APTw+MK and APTw+FA+MK, which showed that AK may have unique advantages in distinguish BPH and PCa and the changes associated with cancer tissue should be investigation.Conclusion
In summary, we found the combination of the APTw and multiparameter of DKI showed some positive signs to differentiate BPH and PCa. The AK parameter in DKI shows special and differential diagnosis efficiency.Acknowledgements
No acknowledgment found.References
[1]. Zhou Jinyuan, Heo Hye-Young, Knutsson Linda et al. APT-weighted MRI: Techniques, current neuro applications, and challenging issues. [J] Magn Reson Imaging, 2019, 50: 347-364.
[2]. He Yong-Lan, Li Yuan, Lin Cheng-Yu et al. Three-dimensional turbo-spin-echo amide proton transfer-weighted mri for cervical cancer: A preliminary study. [J] Magn Reson Imaging, 2019, 50: 1318-1325
[3]. Jensen Jens H,Helpern Joseph A,Ramani Anita et al. Diffusional kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imaging.[J] .Magn Reson Med, 2005, 53: 1432-40.
[4]. Tamura Chiharu,Shinmoto Hiroshi,Soga Shigeyoshi et al. Diffusion kurtosis imaging study of prostate cancer: preliminary findings.[J] .J Magn Reson Imaging, 2014, 40: 723-9.
Figures
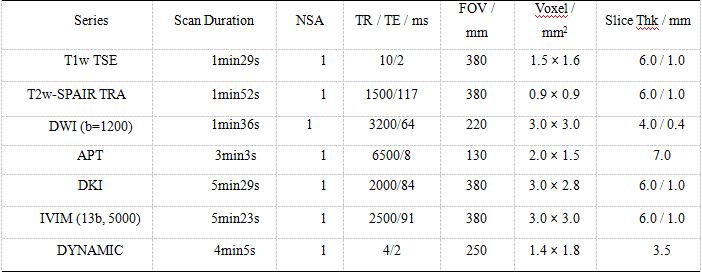

Table 2. Comparison of APTw, FA, MK and Ka between HBP and PCa (x±s)
*P<0.05 was considered statistically significant different
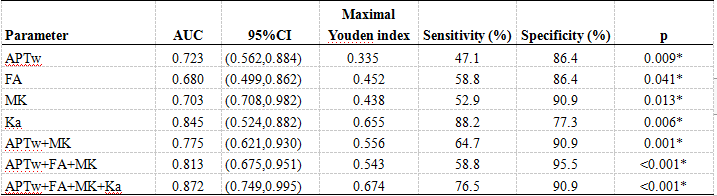
Table 3 Analysis of diagnostic efficacy of APTw value and DKI parameters FA、MK、Ka values as well as APTw value combined with DKI parameters
*P<0.05 was considered statistically significant different