2381
Ultra-fast DCE breast MRI protocol using Compressed-SENSE: A quantitative comparison study with standard protocol in Breast Cancer detection
Shikha Panwar1, Rupsa Bhattacharjee2, Vivek Pawar3, Stanley PK2, and Harsh Mahajan1
1Mahajan Imaging, Gurugram, India, 2Philips Health Systems, Philips India Limited, Gurugram, India, 3Philips Health Systems, Philips India Limited, Pune, India
1Mahajan Imaging, Gurugram, India, 2Philips Health Systems, Philips India Limited, Gurugram, India, 3Philips Health Systems, Philips India Limited, Pune, India
Synopsis
Main challenge associated with conventional DCE-MRI of breast is compromise between spatial and temporal-resolution. In this study our objective is to develop an ultra-fast breast dynamic protocol keeping both spatial and temporal resolution sufficiently high. This is enabled by using compressed SENSE acceleration technique. Proposed Compressed-SENSE enabled ultra-fast dynamic breast DCE protocol design has the potential to be used as alternative of conventional DCE protocol. It gives contrast wash-in information from arteries and veins within very short time, and can significantly differentiate between malignant and benign breast lesions quantitatively (validated on proven 10 malignant and 10 benign cases).
Purpose
Breast MR imaging is now a well established modality for cancer detection due to its high sensitivity and reasonably good specificity in patients with dense breast, high-risk screening, preoperative staging in newly diagnosed disease, neoadjuvant therapy monitoring, and residual disease evaluation [1-3]. Dynamic-contrast-enhanced (DCE) MRI is the mainstay of breast MR protocol, which characterizes the lesion in terms of morphology and contrast kinetics enabling breast cancer detection. Main challenge associated with conventional DCE-MRI of breast is compromise between spatial and temporal-resolution. As reported in studies, need of high-spatial-resolution trades off the achievable temporal resolution/ dynamic sequence time to a minimum of 1 minute or more. This long temporal resolution limits conventional DCE-MRI in differentiating contrast uptake between internal mammary artery and vein. Studies have been reported exploring different ways of developing an ultra-fast breast dynamic protocol that can capture the inflow contrast in lesions, and hence can be used for contrast wash-in analysis qualitatively or quantitatively[4-5]. In this study our objective is to develop an ultra-fast breast dynamic protocol keeping both spatial and temporal resolution sufficiently high. This is enabled by using compressed SENSE acceleration technique that combines parallel imaging and compressed sensing by adopting balanced sampling method. Performance of proposed ultra-fast technique has been compared quantitatively with conventional DCE breast protocol.Methods
This Institutional Ethical Committee-approved study included a total of 20 patients between the ages of 30 – 82 years with 20 lesions (10 malignant, histopathologically proven and 10 benign, some biopsy proven, others typically benign & stable on serial imaging). All patients underwent conventional and ultra-fast DCE-MRI in a 3.0T MRI multi-transmit (Ingenia, Philips Healthcare, The Netherlands) using a dedicated multichannel phased array breast coil. The dynamic series utilized T1 high-resolution isotropic volume examination (eTHRIVE) sequence demonstrated in Figure 1 consisting of a) conventional pre-contrast dynamic (1 min 05 secs) run followed by b) a range of 10 ultra-fast dynamics (5.19 secs each) enabled by Compressed SENSE acquisition after intravenous administration of gadolinium contrast (Gadoteric Acid Clariscan, GE) at 0.1 mmol/kg followed by 20 ml saline flush injected at 2nd ultra-fast dynamic at the rate of 2 ml /sec. This is again followed by c) 4 conventional dynamic post-contrast sequence (part-a). The dynamic scans have no inter-dynamic gap. Image acquisition parameters are described in figure 2.One radiologist with 14 years of experience in reading breast MRI, manually identified a single voxel within each suspicious lesion on 1st conventional post-contrast sequence and obtained values on corresponding voxels on ultra-fast and conventional dynamics as explained in figure 2. The signal intensities are defined as explained in figure 3. Independent t-test has been carried out in Medcalc [6] between IER values of conventional and ultra-fast as well as DER conventional and ultra-fast to check if they can differentiate between malignant and benign lesions significantly.
Results and Discussion
The study results are summarized in Figure 4. The independent t-test shows that DER values calculated from Ultra-fast protocol can significantly (p<0.001) differentiate between malignant and benign similar to DER values calculated from conventional protocol. Similar results were found in case of IER values. IER values calculated from Ultra-fast protocol significantly (p<0.001) varies between malignant and benign similar to IER values calculated from conventional protocol. This is turn indicates, the ultra-fast dynamic protocol can quantitatively behave as the conventional protocol in terms of differentiating malignant vs benign cases. This protocol is less than a minute, saves time and increases patient comfort in lying prone for shorter time. In terms of clinical information, it contains pre-contrast, early and delayed contrast enhancement as well as wash-in patterns, i.e. how the contrast is washed into internal mammery artery and veins are visible in different acquisitions. Sample case results are shown in figure 5. In case of conventional protocol, the early-enhancement dynamic itself is long enough to get all the arteries and veins enhanced simaltaneously; thereby making it difficult for radiologists to diagnose wash-in information. The ultra-fast protocol preserves spatial resolution almost equivalent to conventional dynamic protocol. This has been achieved by the Compressed-SENSE technique. It also opens up the potential for Ultra-fast dynamics to contribute to pharmacokinetic modelling whereas higher-spatial-resolution can help to determine curve and signal-enhancement patterns within such higher temporal resolution. Further studies are being formulated to evaluate this protocol in differentiating between grades of breast tumors based on the contrast-information it can provide.Conclusion
Proposed Compressed-SENSE enabled ultra-fast dynamic breast DCE protocol design has the potential to be used as alternative of conventional DCE protocol. It is compact, gives contrast wash-in information within very short time, and can significantly differentiate between malignant and benign breast lesions.Acknowledgements
No acknowledgement found.References
[1] Kuhl CK, Schrading S, Strobel K, Schild HH, Hilgers RD, Bieling HB, et al. Abbreviated breast magnetic resonance imaging (MRI): First postcontrast subtracted images and maximum-intensity projection-a novel approach to breast cancer screening with MRI. J Clin Oncol. 2014;32:2304–10. [2] Santoro F, Podo F, Sardanelli F. MRI screening of women with hereditary predisposition to breast cancer: Diagnostic performance and survival analysis. Breast Cancer Res Treat. 2014;147:685–7. [3] Martincich L, Montemurro F, De Rosa G, Marra V, Ponzone R, Cirillo S, et al. Monitoring response to primary chemotherapy in breast cancer using dynamic contrast-enhanced magnetic resonance imaging. Breast Cancer Res Treat. 2004;83:67–76. [4] Le Y, Kipfer H, Majidi S, Holz S, Dale B, Geppert C, et al. Application of time-resolved angiography with stochastic trajectories (TWIST)-Dixon in dynamic contrast-enhanced (DCE) breast MRI. J Magn Reson Imaging. 2013;38(5):1033–42. https://doi.org/10.1002/jmri.24062. [5] Mus RD, Borelli C, Bult P, Weiland E, Karssemeijer N, Barentsz JO, et al. Time to enhancement derived from ultrafast breast MRI as a novel parameter to discriminate benign from malignant breast lesions. Eur J Radiol. 2017;89:90–6. https://doi.org/10.1016/j.ejrad.2017.01.020. [6] MedCalc Statistical Software Version 14.8.1 (2014) MedCalc Software, Ostend, Belgium.Figures
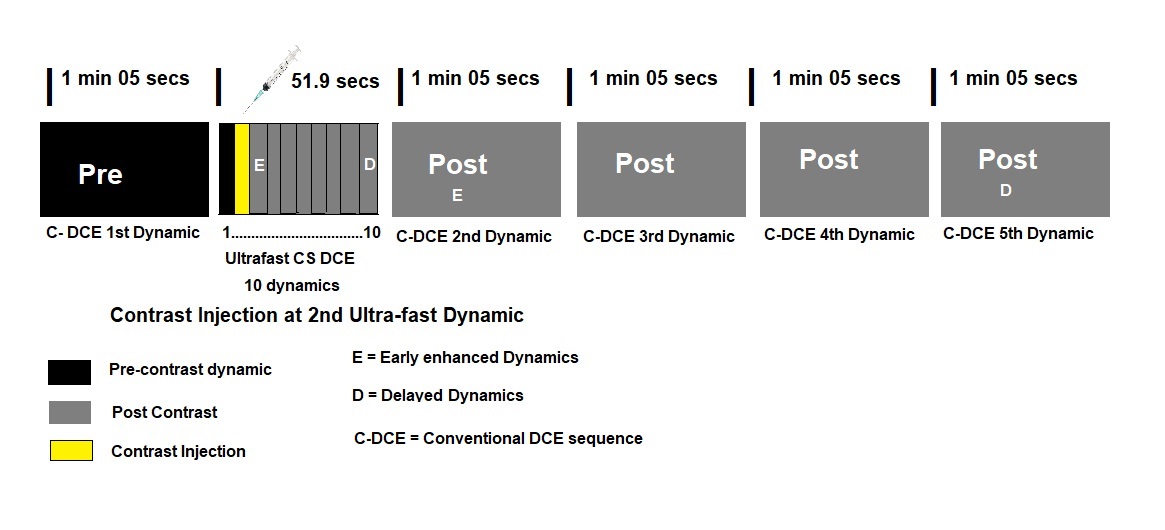
Figure 1: Sequence Design of the Ultra-fast dynamic protocol

Figure 2: Parameter details and comparison between ultra-fast and conventional dynamic sequence

Figure 3: Definition of parameters used for calculation and comparison
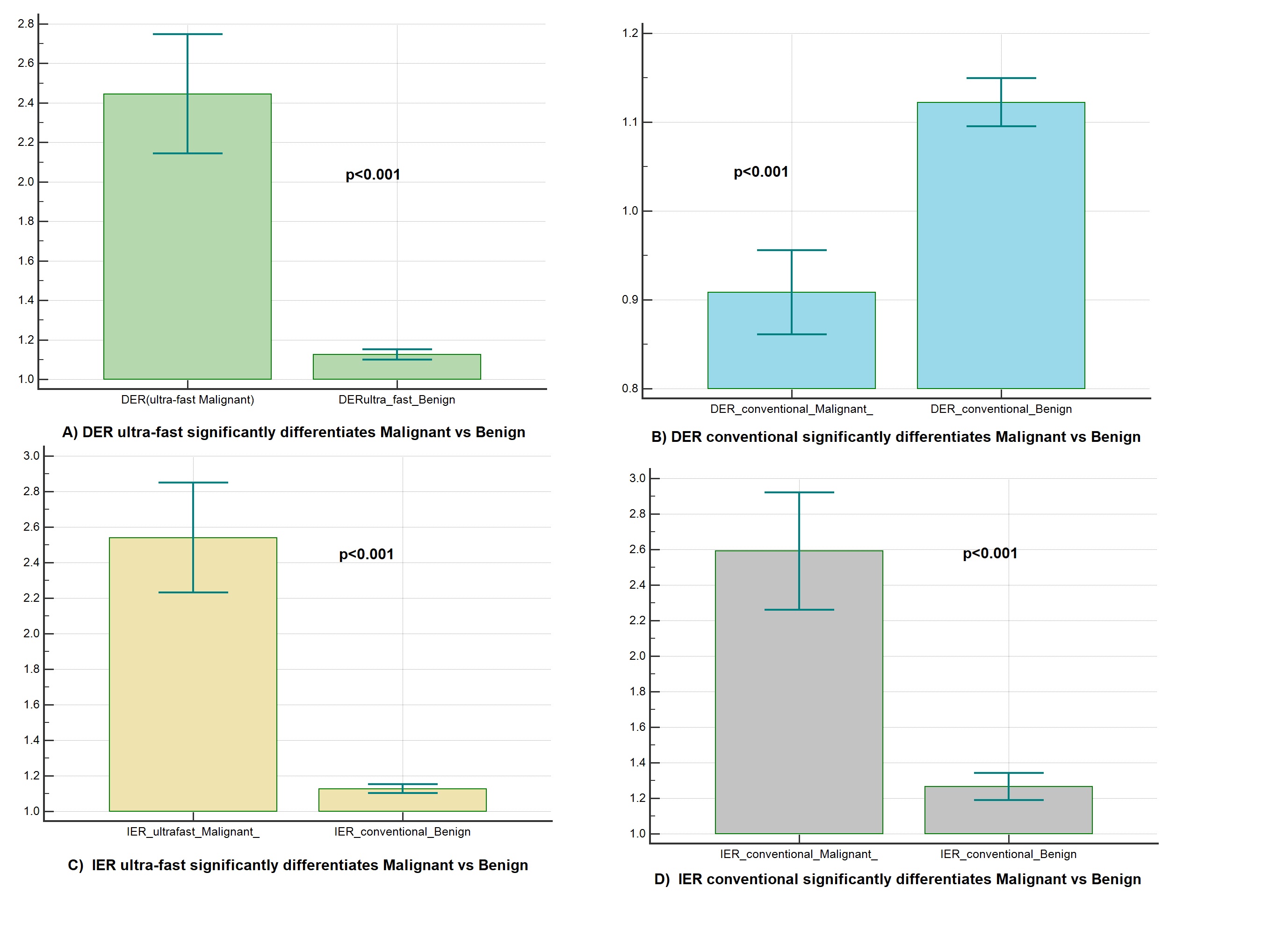
Figure 4: Results
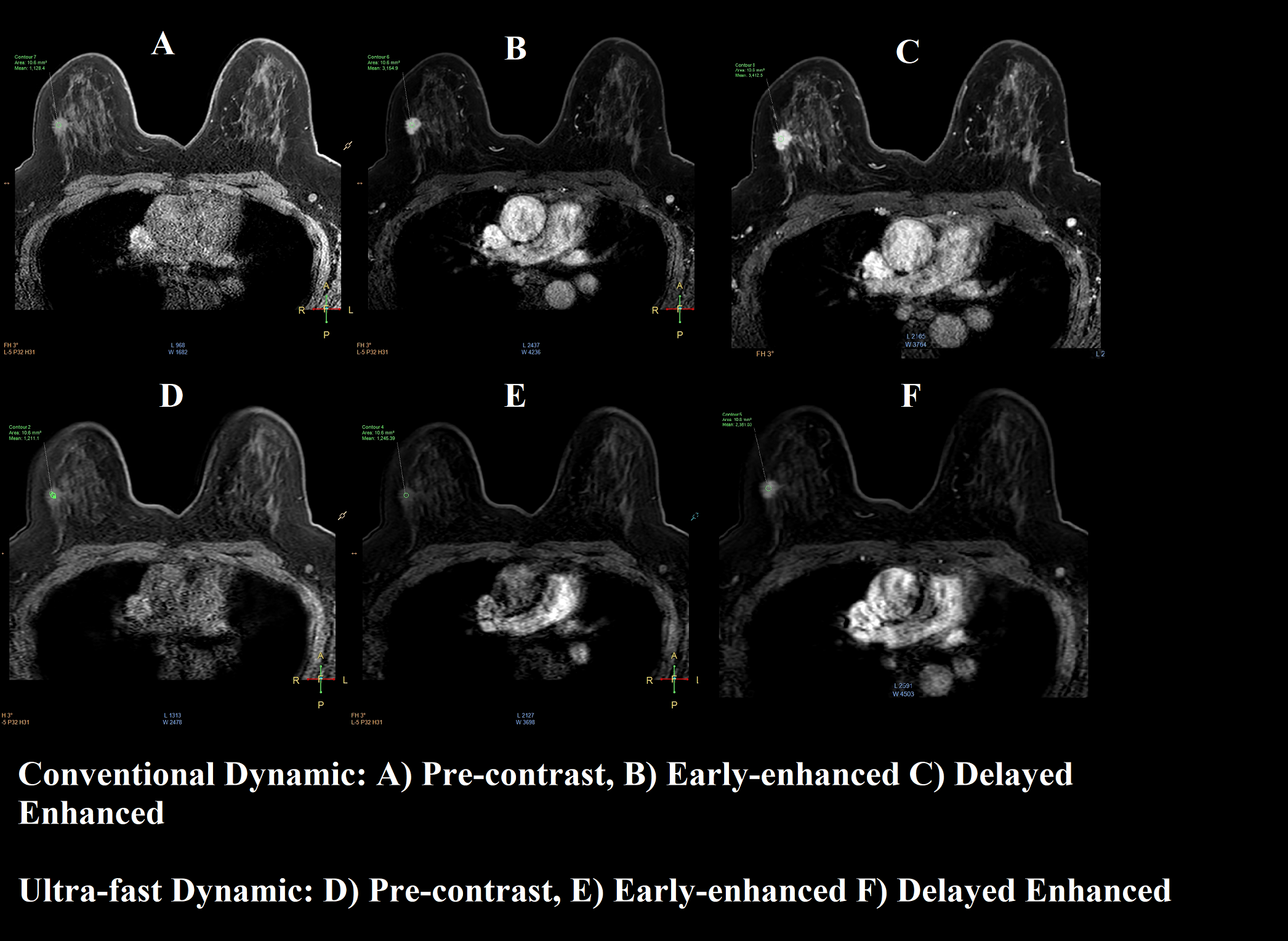
Figure 5: Sample Images of Conventional and Ultra-fast Dynamic