2375
Perfusion analyses of breast benign and malignant lesions using super high frame rate reconstruction with stack-of-stars acquisition1University of Yamanashi, Chuo, Japan, 2MR Collaboration and Development, GE Healthcare, Hino, Japan, 3MR Collaboration and Development, GE Healthcare, Tucson, AZ, United States, 4MR Collaboration and Development, GE Healthcare, Madison, WI, United States
Synopsis
Dynamic contrast-enhanced MRI (DCE-MRI) is used to diagnose breast cancer. Although 3-phase DCE-MRI is used in clinical settings according to BI-RADS, higher temporal resolution with perfusion analyses may be essential to precisely distinguish between benign and malignant breast lesions. Stack-of-stars (SOS) acquisition enables motion-robust DCE-MRI with arbitrary high temporal resolution. We performed perfusion analyses of breast lesions using super-high frame rate reconstruction (3.2 s/phase) with SOS acquisition, compared with BI-RADS-based enhancement category using typical temporal resolution (32 s/phase), and found that two more lesions were accurately diagnosed via perfusion-based analyses using super-high frame reconstruction compared to BI-RADS-based evaluation.
Introduction
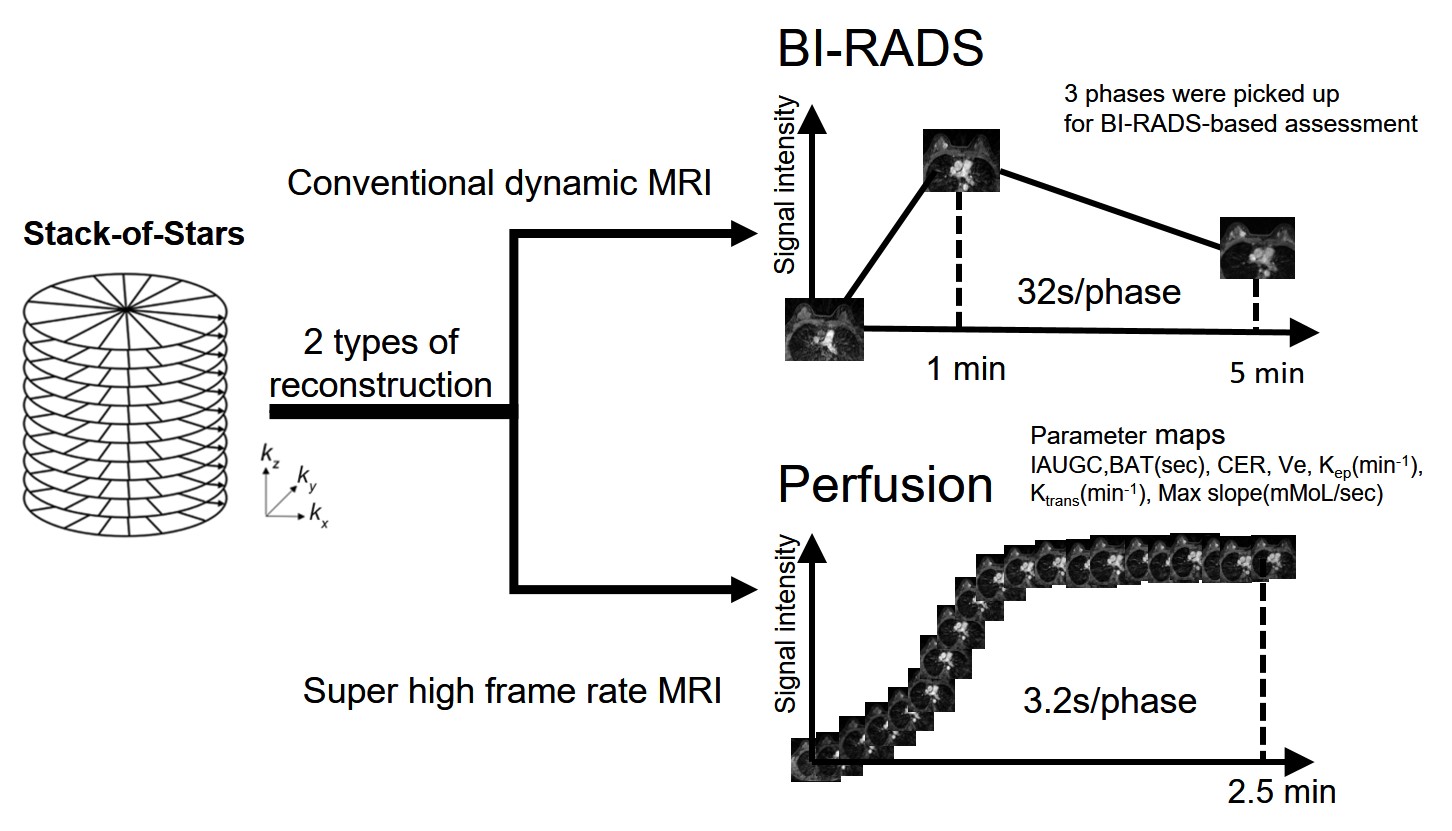
Stack-of-stars (SOS) is a technique that enables motion-robust dynamic contrast-enhanced MRI (DCE-MRI) with high temporal resolution. Breast lesions are typically assessed based on DCE-MRI-based interpretation according to the Breast Imaging Reporting and Data System (BI-RADS). In clinical settings, we typically acquire triple-phase DCE-MRI (pre-contrast, early phase, and late phase). However, multiple-phasic DCE-MRI with >3 phases can be essential for the differential diagnosis of benign and malignant lesions1,2.Specifically, when using SOS acquisition, extremely high temporal resolution can be achieved by sharing the views of k-space, which is considered to be useful to ensure accurate perfusion analyses. This study aimed to investigate the usefulness of perfusion analyses using super-high frame rate reconstruction with SOS acquisition to distinguish between benign and malignant breast lesions.Methods
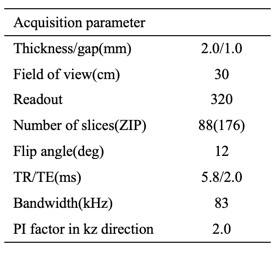
This retrospective study was approved by the relevant institutional review board, and informed consent was waived. We included 14 patients suspected of breast cancer who underwent DCE-MRI with SOS followed by biopsy or breast surgery from January 2019 to May 2019 (mean age, 55.9 years, range, 33-69; 14 women). We examined 27 breasts of 14 patients separately (with malignant leasons: 13 breasts, with benign lesions: 14 breasts). DCE-MRI was performed using a 3-T MR system (Discovery 750; GE Medical Systems, Waukesha, WI, USA) with a 32-channel phased-array coil. MR parameters are presented in Table 1. Gadobutrol (1.0 mL/kg) was administered at a rate of 1 mL/s followed by a 20-mL saline flush. The scan was commenced immediately before injecting the contrast agent to acquire 1100 spokes within 5 minutes. Two retrospective reconstructions were performed using the data sets: 1) typical temporal resolution (total of 11 phases with 32 s/phase, from which 3 phases were picked up for BI-RADS-based assessment) and 2) super-high frame rate (total 110 phases with 3.2 s/phase) creating time-to-intensity curves (TIC) and perfusion analyses (GenIQ, AW, GE Medical Systems,Waukesha, WI, USA) (Figure 1). The images with typical temporal resolution were evaluated by a radiologist to determine the enhancement patterns based-on the BI-RADS rules: rapid (reflecting malignancy), medium, and slow. Perfusion analyses (GenIQ) was conducted using images with a super-high frame rate to generate the following parametric maps: initial area under gadolinium contrast agent concentration-time curve (IAUGC); bolus arrival time (BAT[s]);contrast enhancement ratio (CER); wash-out rate (Kep[min-1]); wash-in rate (Ktrans([min-1]); maximum slope of signal-increase (Max slope [mMoL/s]);and extravascular extracellular space volume (Ve). Cutoff values of these parameters were determined to calculate diagnostic accuracy for distinguishing malignant breast lesions from benign breast lesions. These diagnostic accuracies were compared with those of a BI-RADS-based enhancement pattern.Results
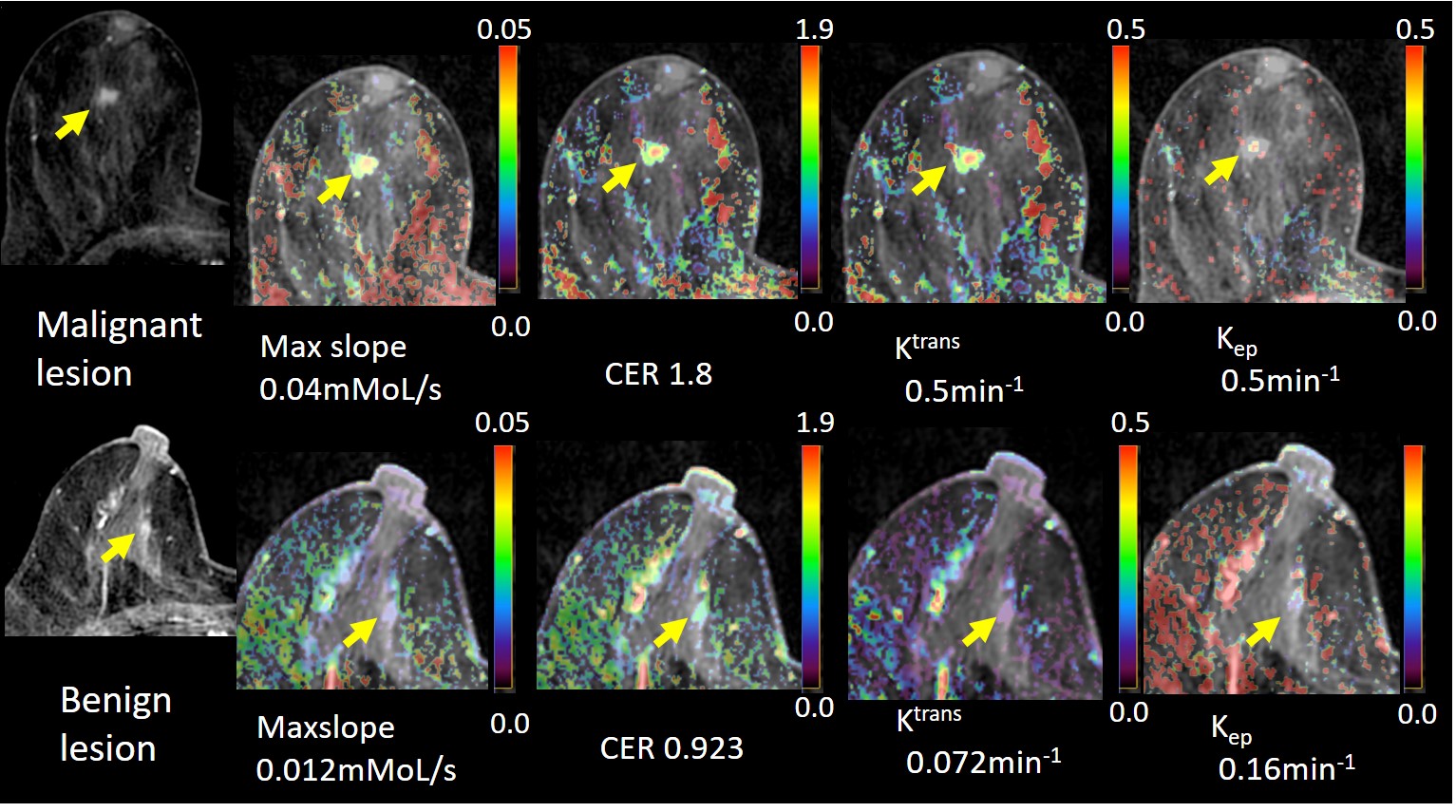
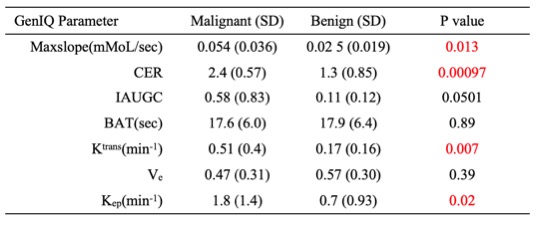
The mean values of Max slope, CER, Ktrans, and Kep were significantly different between benign and malignant lesions (Table 2). Rapid enhancement pattern by BI-RADS was more frequently observed in malignant lesions than in benign lesions. Comparisons with regard to pattern analyses based on BI-RADS revealed that two more lesions were accurately diagnosed via perfusion-based analyses using super-high frame reconstruction (Table 3).Discussion
In this study, we revealed the usefulness of perfusion analyses of breast lesions with the data of high frame rate reconstruction to distinguish malignant breast lesions from benign lesions. Characteristically, breast cancer is considered to have hyper-perfusion. According to perfusion analyses, the parameters predicting breast cancers were the greater Max slope (having more rapid enhancement), larger CER (more total enhancement), and bigger Ktrans(contrast rapidly moving into the extracellular space) and Kep (rapid wash-out of the contrast). These results are consistent with those of previous studies on breast cancer1,2. In this study, super-high frame rate reconstruction (image sets every 3.2 s) was available using SOS acquisition, which possibly ensured accurate perfusion results. Temporal resolution is one of the important factors that affect the results of perfusion analyses. Total blood flow, for example, can be underestimated by lower temporal resolution wide temporal window compared with sufficiently high temporal resolution narrow temporal window3.Conclusion
Super-high frame rate reconstruction with SOS acquisition is useful for distinguishing between benign and malignant breast lesions using perfusion analyses.Acknowledgements
No acknowledgement found.References
1. Maya H, Masako K, Natsuko O, et al. New parameters of ultrafast dynamic contrast‐enhanced breast MRI using compressed sensing. J Magn Reson Imag 2019; Epub ahead of Print.
2. Ritse M, Roel M, Jan Z, et al. A Novel Approach to Contrast-Enhanced Breast Magnetic Resonance Imaging for Screening High-Resolution Ultrafast Dynamic Imaging. Investigative Radiology. 2014;49(9):579‐585.
3.Tetsuya W, Daiki T, Kang W, et al. Influence of reconstruction parameters on Liver perfusion analysis in Stack-of-Stars dynamic liver imaging: A feasibility study. JSMRM 2019, P3-A-17
Figures