2356
High Time Resolution 2D Chest Imaging Using A 0.5T Upright Paramed MRI Scanner.
James Harkin1, Michael Barlow2, Alan Smyth3, Ian Hall1, and Andrew Prayle3
1University of Nottingham, Nottingham, United Kingdom, 2Faculty of Medicine & Health Sciences, University of Nottingham, Nottingham, United Kingdom, 3Medicine and Health Sciences, University of Nottingham, Nottingham, United Kingdom
1University of Nottingham, Nottingham, United Kingdom, 2Faculty of Medicine & Health Sciences, University of Nottingham, Nottingham, United Kingdom, 3Medicine and Health Sciences, University of Nottingham, Nottingham, United Kingdom
Synopsis
Using a 0.5T Paramed MROpen Upright MRI scanner, adult and paediatric cohorts as young as 3 can be scanned without sedation. 2D images can be acquired every <0.5s allowing for diaphragm movement to be characterised. Lung density variation through the breathing cycle can also be extracted.
Introduction
At Nottingham the 0.5T Paramed MROpen Upright MRI scanner has two parallel TechMag Redstone spectrometers; making it the first of its kind to allow for both proton and multinuclear imaging (figure 1). The subject can be imaged in a variety of positions, including supine, seated or standing. The open design is also excellent in terms of patient experience; claustrophobic reactions are virtually eliminated and the easy access and different orientations can be exploited to make the scanner better suited to disabled or paediatric cohorts.Many lung conditions are characterised by heterogeneity of ventilation within the lung fields (caused by obstruction to bronchi, or lung parenchymal disease) which manifest as regions of fixed density throughout the respiratory cycle, in comparison to well ventilated areas, where the density fluctuates with each respiratory cycle. Other lung diseases are characterized by deformation of the lung architecture (through lung or thoracic malformation or weakness), and understanding the changes of lung geometry of the malformed or weakened thorax during the respiratory cycle would aid our understanding of these diseases.
Current options for non MR real time in-vivo imaging include ultrasound and fluoroscopy (continuous X-ray image). Both allow for the acquisition of high time resolution data. However, ultrasound is very operator dependent and fluoroscopy is both ionising and provides an infinite slice through the body.
We hope to be able to accurately characterizes the diaphragm movement throughout the breathing cycle and also investigate regional lung density changes. Sections of the lung may become transiently blocked by mucus. This will result in them not inflating efficiently and consequently the lung density won’t drop in this region.
The majority of high time resolution MRI scans are currently performed supine, horizontal. For chest imaging this isn't from ideal. Lung function, volume, and arterial oxygen levels are affected by body position1. By lying supine lung function is reduced and for patients at the latter stages of chronic conditions, such as COPD, many can’t lay in a supine position for extended periods.
The Paramed does have limitations for obtaining high time resolution data: The Paramed has a slow slew rate of 33Tm-1s-1; limiting the minimum TR. The Paramed is also normally ran conventionally through a clinical interface. Through this there are limitations on the minimum resolution of a scan and consequently the minimum acquisition time. The minimum time for a GRE scan is >1 minute. However, the clinical interface is built on TNMR allowing huge flexibility in sequence design.
Methods
The minimum TE and TR of a GRE sequence on the Paramed was 8ms and 18ms respectively. In TNMR a 2D Spoiled GRE sequence was developed with TE=4.65ms, TR=12.90ms. The resolution was reduced to 160 frequency encodings and 64 in the phase encodings. Between each slice a 50ms gap was introduced to prevent coherences building up. This resulted in an image being acquired every 875.6ms. By halving the number of phase encodings this time is reduced to 462.8ms. Scans were performed at approximately the Ernst angle for lung tissue (T1 lung ~1008ms2) and ran for 5 minutes.Scans on pediatric volunteers were performed with them sitting on a parents lap. This meant they stayed approximately central in the magnet. Volunteers as young as 3 years old have been inside the scanner without sedation.
As the volunteer inhales the lungs expand and their proton density reduces; producing a lower signal. However, this also results in alveoli shifting between voxels. For lung density variation investigations ATNsR software3 was used to map each image onto the first image. This ensures the shape of the lungs is the same throughout the time course and should allow for the assumption that each alveoli stays in the same voxel. The lungs can then be segmented out and a FT taken over the time domain. The highest peak of this should correspond to the average breathing rate throughout the scan.
Results
Figure 2 shows 1 frame from the 32 phase encoding time course (1cm thick slice) and figure 3 shows one frame from the 64 resolution time course (3cm thick slice). For both the outline of the diaphragm could clearly be seen to rise and fall with breathing. For the 32 phase encoding time course the volunteer breathed on average every ~6s. The Fourier transformed time course can be seen in figure 4 The largest peak was found at every 5.8s.Discussion
In real time videos of both 32 and 64 phase encoding it was easy to distinguish the diaphragm movement. By moving to a projection k-space sampling with each k space spoke at the golden angle we hope to increase the time resolution further. Over the whole lung it was also possible to extract the average breathing rate. By looking at smaller regions we hope to see explore regional lung density changes.Conclusion
The diaphragm movement throughout the breathing cycle has been imaged at a time resolution of 462.8ms. The lung density average variation frequency was also extracted at the same as the average breathing frequency. The Upright Open design of the scanner has allowed for volunteers as young as 3 to be comfortable inside the scanner without need for sedation.Acknowledgements
Thank you to the Haydn Green Foundation for funding my PhDReferences
- Dean, Elizabeth. "Effect of body position on pulmonary function." Physical Therapy 65.5 (1985): 613-618.
- Gai, Neville D., Ashkan A. Malayeri, and David A. Bluemke. "Three‐dimensional T1 and T2* mapping of human lung parenchyma using interleaved saturation recovery with dual echo ultrashort echo time imaging (ITSR‐DUTE)." Journal of Magnetic Resonance Imaging 45.4 (2017): 1097-1104.
- ANTsR software. https://github.com/ANTsX/ANTsR Accessed June 15th 2019
Figures
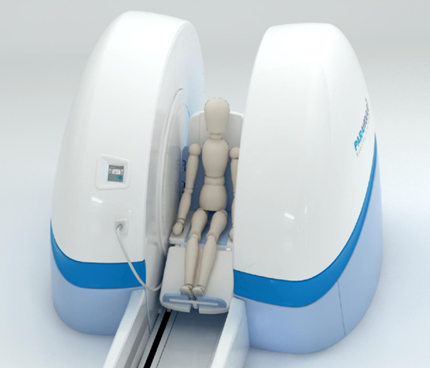
Figure 1. Paramed Medical Systems MROpen Upright MRI Scanner.
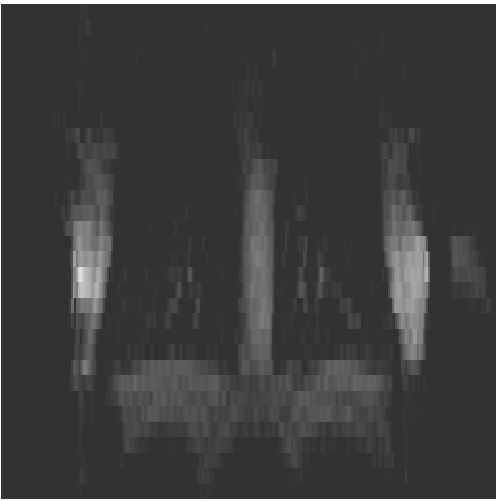
Figure 2. 32 phase encodings 1cm thick slice centered behind heart. Image every 462.8ms.
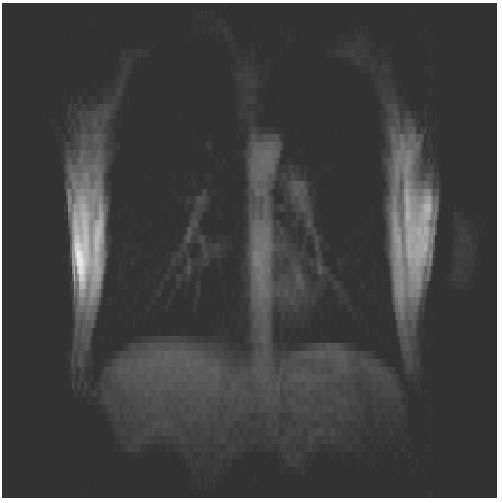
Figure 3. 64 phase encodings 3cm thick slice centered behind heart. Image every 875.6ms.
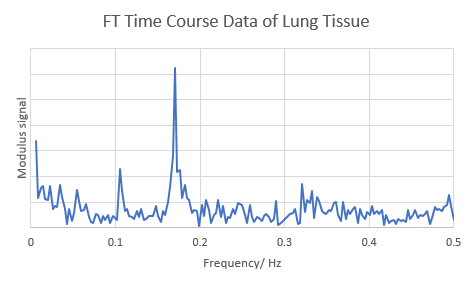
Figure 4. Fourier transformed time course data of lung tissue.